INTRODUCTIONBenign work-related Laryngeal diseases have been reported for long time (1). The difficulty to settle legal-medical link between structural changes and phono-articulation effort has caused some questions, which were dispersed with knowledge evolution of vocal emission and of the confused factors that interfere in it (2).
Cyst of Vocal Cord is a structure covered by epithelial surface with its own internal content and separated from where it is immersed. It consists of an abnormality from superficial portion of its own lamina, below the epithelium, but out of vocal muscle (3), unilateral, and it is classified according to its localization, in submucosal surface for example where is the most common place.
Its origin is focused, affecting shape and edge of the vocal cord, having as consequence a disorder in mucosal wave spreading. One of its main features is the unilateral way that causes attrition reaction in contra-lateral vocal cord.
Both in its most superficial localization and profound one, it unbalances mucosal wave, resulting dysphonia as clinical symptom.
Etiology: phonotrauma causes an inflammatory process on vocal cord having cicatrix as result. One of the consequences is an obstruction of the duct of submucosal glands. There are some reports of symptoms of congenital etiology in some cases, but it is clear the distinction of the clinical development.
Phonotraumatic submucosal cyst is predominantly of intracistal epithelial type, what can obtain glands, ciliary or oncolitic features.
Epidermoid type, in some cases, provides aid to congenital etiology suspicion, which, together with prospective studies and laryngostroboscopic detection, does not present physiopathological basis (3).
There are incontestable clinical evidences that trauma develops an inflammatory process with hemorrhagic area and cicatricial result would peak with obstruction of gland ducts and cystic retention (5).
Clinical manifestation: in acute phonotrauma cases, dysphony installation is abrupt and, hemorrhagic areas in relation to laryngostroboscopia can be observed. If a prospective follow-up is maintained, cystic formation will become evident in 60 days. Dysphony is followed by dysphonic syndromes, which are: foreign body sensation, throat clearing, and sore throat. Together with those, it can be observed the process of functional adaptation of the organ in relation to phonation, causing an increasing circle of retroalimentation in which organic lesion develops functional disfuntion and an increasing worsening of dysphinc manifestation (5). In laryngostroboscopia we can find wave absence or monocorditis.
Prevalence among teachers: rare epidemiologic studies point out a prevalence of 4.2% for cysts. This is not expressive only for cysts, but also nodule, and polyps.
Target: describe clinical evolution of the disease-related to patient´s work.
CASE REPORTFemale patient, 39ys, working as a primary school teacher. She went to Subdelegacia do Trabalho SDT 1 Norte-SP (Labour Subdepartment in North District of São Paulo city) because she had been fired on the last day of school year, even been sick.
The patient reported that she had already presented cough spastics crisis followed by constat dysphonia with intermittent period one year before been fired. Espatic
With this procedure, she could keep her work activity in classroom, but dysphonia became worse. During classes, she started speaking less and writing more on the board, followed by a better oral hydration. She also reported that in her vacation period, dysphonic syndrome was less intense but not null.
At the beginning of the following term, she made use of a microphone of her own. This was the main factor, according to her, that avoided medical leaves, but dysphony remained constant and unchanged. She also assures that students, aware of her problem, cooperated in terms of being quiet during classes.
During that period, three videolaryngoscopy was carried out, which confirmed the diagnosis of submucosal cyst of left vocal cord. The last exam was done on October 14, 2004 (see Picture 1)
She was fired on June 30, 2004. In the demission medical evaluation, she was considered incapable and was sent to INSS investigation (National Social Security Institute) that concluded her "incapability to work", giving her sick pay.
Work antecedents: she started working as a primary school teacher at 17 year of age, and did it for 5 years. She returned to work in 1993 in double shifts in private and public schools, adding up 9 continuous daily work hours.
Self evaluation: As recommend by Comissão Tripartite de Normatização para a Voz Profissional (Tripartite Comission of Rule to Professional Voice) (7) we made a self evaluation which presented the following results:
Work Organization: up to June 2004 she was working at two educational institutions, teaching primary students. She worked more than 6 hours a day having less than 15 minute-break. The number of students in classroom was from 31 to 50, and being a teacher was her only activity.
Clinicla Symptoms: sore throat, foreign body sensation and throat clearing during the whole day and night, neck pain at night, constant hoarseness. She cares with her voice, doing hydration and having balanced diet.
She has neither smoked nor drunk alcohol, nor made use of drugs nor use of continuous medicine; she has always practiced sports such as jogging and swimming.
Vocal qualitative evaluation: predominant intercostal respiration with presence of pneumophonoarticulatory incoordenation, reduced maximum phonation time, vocal laryngopharynx resonance; moderate degree roughness in throat, serious tension, moderate breathiness, light hoarseness, Oscillating facial and cervical tension according to installation of clear vocal fatigue.
DISCUSSIONWork-related laryngopathies consist of such diseases that affect professional who make use of their voices as main work tool, and dysphony is the main clinical symptom (8).
Laryngopathies with organic lesion are similar in their natural history. Thus, we observe common clinical pre-pathogenic nature of the nodules, polyps and cysts of vocal cords (2). To establish causes with their respective legal-medical implications, it is needed to integrate factors. Though, to apply concepts, it is necessary to define such factors:
1. Individual factors: sex, age, vocal hygiene;
2. Environment factors: noise, acoustic, microphones, ergonomy, work organization, dust;
3. Pre-disposition factors: physiologic hormone alterations or not, acid larynx followed or not by gastro-esophageal reflux, inflammatory and allergic process of the mucosa, tabagism, alcoholism, self-medication, caffeine, stress.
4. Provoking factors: vocal badly-use and abuse.
The isolated provoking factors are not able to work on disease manifestation as a single etiologic cause.
Thus, the four types are essential because they associate with and work on the appearing of pathogenic process (7, 8).
Therefore, when we detect a multifactorial action on the disease installation, its prevention is more comprehensive although it can be an aim of efficient performance.
The preventive and popular procedures can help on early detection of cases subjected to high risk of disease.
The reported case explains well this fundamental question.
Although she has been a teacher for 19 years, the vocal risk was not considerable on periodic precedent evaluations and, although she had already been sick with cyst videolaryngoscopic diagnosis of left vocal cords, she was considered incapable only in the demission process.
This is a typical case when dissociation between the control made on teachers who do a periodic occupational exam faces detected disease by a specialist who works with sophisticated technique of investigation.
In order to have a rational entailment to provoke the indication of more complex procedures, such as syndrome symptom detection of early dysphony, we have developed and applied a self-evaluation which will be useful to doctors who control people (teacher) to select the cases which will undergo specific evaluation or even will be target of preventive performance.
We consider that laryngopathies develop themselves during years. Rationalizing and determining performance procedures, which are necessary for some occasions, leads to action taking, as well as it changes them according to prospective follow-up of self-evaluations.
This patient is incapable to work, but she has made an effort to keep her activity without being withdrawn (11).
The self-evaluation applied would detect early dysphony syndrome.
Dysphony syndrome develops itself with symptoms by: alterations of intermittent vocal emission, foreign body sensation, throat clearing, tiredness feeling when speaking, hoarseness, odinophagy, odynophonia
These symptoms precede the appearing of organic lesion and they should be systematically researched on people who make us of voice professionally.
In the literature revision, we have found evaluations applied with different purposes (12).
We consider that evaluations should have a part of standardized clinical symptoms and other questions, related to work organization and habits, suited to people under control.
Vocal cord cysts are related to vocal abuse as a result of inflammatory process, usually together with hemorrhage (5)
Its prevalence is not known, but on teacher (6).
On the process physiopathology is reported that repeated traumas and other present factors develop duct obstruction (2).
On clinical symptoms, it occurs variations related to type of vocal abuse and badly-use. Thus, singers present severe symptoms of dysphony installation (5). It can occur diplophonia when organic lesion is associated with vocal palsy (3).
Many of the times it has monocorditis appearance.
The vibration surface of the vocal cord consists of a stratified complex layer. The repeated traumas on this area are associated to the mentioned factors, forming benign lesions such as cicatricial consequence.
Thus, glottis closing is altered and diplophonia is installed.
The differential diagnosis should be done with other benign lesions of larynx such as nodules, polyps and intracordal tumors.
Treatment: surgery of cyst withdrawn ends the problem, but vocal quality is not always satisfactory. Phoniatric control is vital on pre- as much as post-surgery. The use of medicine is necessary in order to control individual and pre-disposition factors. An orientation to environment factors is also part of clinical control.
FINAL CONSIDERATIONSSubmucosal cyst of vocal cords can form clinical manifestation of work-related laryngopathy, and should be routinely checked on professionals of voice.
The proposed self-evaluation reported provides useful components for this professionals´ control as initial procedure with legal-medical feature, but not exclusive, it is necessary laryngoscopic evaluations.
I would like to thank Carlos Alberto Angelini, Labour Subdelegate in North part of São Paulo city, who has always helped in implementing prevention procedures of Occupational Dysphony Program.
BIBLIOGRAPHY1. Calas M, Verhulst J, Lecoq M, Dalleas B, Selhean M. La pathologie vocale chez l´enseignant. Revue de Laryngologie, 1989;110(4):397-406.
2. Johns M M. Update on the etiology, diagnosis and treatment of vocal fold nodules, polyps and cysts. Current Opin Otolaryngol Head Neck Surg, 2003;11:456-461.
3. Schweinfurth J, Ossof R. Vocal fold cysts. Disponível em www.emedicine.com/ent/topic604.htm
4. Rosen CA & Murry T. Nomenclature of the voice disorders and vocal pathology. Otolaryngol Clin North America, 2000;33(5):1035-1045.
5. Sataloff RT, Hawkshaw MJ. Vocal fold cyst, hemorrhage, and scar in a professional singer. Ear, Nose and Throat J., 2000;79(3):140.
6. Urrutikoetxea A, Ispizcua A, Matellanes F. Pathologie vocale chez les professeurs:une étude vidéo-laryngo-stroboscopique de 1046 professeurs. Rev. Laryngol. Otol. Rhinol, 1995;116(4):255-262.
7. Ministério do Trabalho e Emprego. Delegacia Regional do Trabalho no Estado de São Paulo. SDT 1 Norte/SP. Programa Disfonia Ocupacional de Professores. Cubas de Almeida SI & Angelini CA, 2003.
8. Ministério do Trabalho e Emprego.Subdelegacia do Trabalho SDT 1 Norte/SP.Comissão Tripartite de Normatização para a Voz Profissional.Questionário de auto-avaliação para professores.2002.
9. Jacqueline A, Mattiske J, Jennifer MO, Greenwood KM. Vocal Problems Among teachers: a review of prevalence, causes,prevention and treatment. Journal of Voice, 1998;12(4):489-499.
10. Russell A, Oates J, Greenwood M. Prevalence of voice problems in teachers. Journal of Voice, 1998; 12(4):467-479.
11. Sataloff RT, Abaza M. Impairment, disability, and other medical-legal aspects of dysphonia. Otolaryngol Clin North Am, 2000;33(5):1143-1153.
12. Jacobson BH. The voice handicap index (VHI): development and validation. Am J Speech-language Pathol, 1997;6:66-70.
13.Sulica L, Behrman, A. Management of benign vocal fold lesions: a survey of current opinion and practice. Ann. Otol. Rhinol. Laryngol,2003;112(10):827-833.
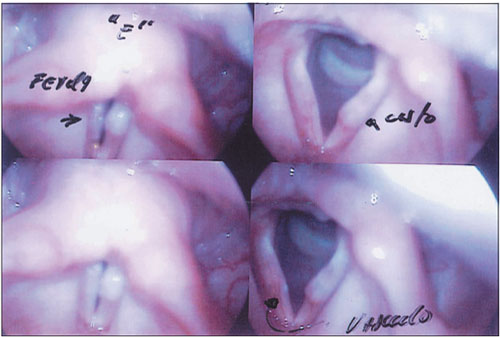
Picture 1. Cyst of Left Vocal Cord. On the superior and inferior left side, we can observe the appearance of vocal cords during phonation. On the right side, we observe the appearance of vocal cords during inhaling.

