INTRODUCTIONAt the present moment there are a great number of technologies available to evaluate several aspects of deglutition function and disfunction. Such technologies allow measuring structure movements in it and also muscular action through space and time aspects. This number of technology can provide analysis of the whole process. Chosing the right method for evaluations will be specific for each case or target depending on the clinical situation.
Among methods for swallowing evaluation, monitoring and biofeedback, there are the videofluoroscopy (VF) and endoscopic evaluation of swallowing (1,2); cervical auscultation with stethoscope, accelerometer or microphones (3); surface electromyography (4); swallowing ultrasound (5), virtual endoscopy by CT with software of reconstruction (6).
Understanding production of sound during swallowing has been a complex job to several authors who has studied such subject. The nech area presents an expressive amount of acoustic activity. Part of this activity is hydraulic, such as arterial and venous blood vessels, cerebrospinal fluid and frequent swallowing of secretion as well as gas exchanges in restriction valves.
HAMLET (7) has pointed that one of the most important acoustic signals of swallowing sound correspond to food moving through cricopharyngeal muscle and has identified a periodic noise, propably from larynx, which 'burst' next to the closing of this muscle, the other signs are aperiodic. Authors also pointed that the movement of hyoid, larynx and epiglottis can contribute to acoustic sign of swallowing. Later, HAMLET (8) described three componets that would cover the sound of swallowing: 1. Weak sign associated to larynx uprising and to passage of food through pharynx; 2. Strong sound associated with cricopharyngeal opening and 3. A weak sound associated with larynx fall.
These data agreed with other studies that reported respiratory action of superior air pathways or sudden changes on muscle during swallowing when in pharynx area as components of sound (9), and that larynx uprising would also contribute as a possible acoustic component of deglutition (3).
TAKAHASHI (10) in his study on digital analysis of sound of swallowing selected the best type of adhesive for fixation of neck detector, the best acoustic detector and the best place for detecting sound of pharyngeal swallowing in adults. Two types were compared, accelerometer with double-sided Sellotape. This showed a large frequency reach. In order to indicate the best place, it was performed a sweeping in 24 points of the neck. From those, point number 5 was indicated to cervical auscultation, described as a medium one between the low point of the cricoid cartilage, just above jugular incision; point number 11, over lateral area of trachea, just inferiorly to cricoid cartilage, and point number 4 over the center of cricoid cartilage.
The acoustic trace of swallowing can be analized in terms of duration, sign frequency and wave amplitude. Russo (11), in his study on acoustic and psychoacoustic describes frequency (f) as a number of cycles perform by particles in one second. The expression cycles was replaced by (Hz), paying homage to Heinrich Hertz, and such unit of measure is internationally used. In BEHLAU´s viewpoint (12) frequency is the speed in which a wave repeats itself by unit of time, indicated by c/s (cycles per second), in older literature, or by Hz in modern one, i.e. 1 Hz = 1 c/s. According to RUSSO (11), amplitude is defined as measurement of deviation or displacement of the particles from its balance position.
Regarding acoustic sign length, there are differences to dry, liquid and pasty swallowing. CICHERO & MURDOCH (13), in their revision on physiological causes of the swallowing sounds, agreed with most of the researchers who say that length of sound sign to liquid swallowing is 500 ms. Though, it was described the length of 250 ms to swallow 1/3 of teaspoon of pasty food. McKAIG (3), points that time is specific for each individual. Some people might swallow food in one second, while other in 3 seconds withough dysphagia.
McKAIG (3), when studying features of frequency of swallowing sign, said that sound energy of the process is between 0 and 2000 Hz. TAKAHASHI (10) observed two peaks, one below 110 Hz and another in 621 Hz. HAMLET (14) found a initial peak of sound in 556 Hz and another in 1.384 Hz.
VICE et. al. (9), when studying babies, said that sound of swallowing changes in amplitude and standard, probably because of food physical features. They report 'initial discreet sound' and 'final discreet sound' that anteceded and precceded, respectively, swallowing from 10 to 30 ms.
Several studies have been invetigated, specially using microphone attached to the neck and digital analysis of sound, what one might know through swallowing sounds, discussing acoustic trace in terms of length, sound frequency and sound wave amplitude of swallowing (10).
McKAIG (3), in his aricle on cervical auscultation, describe that there are in general three strong sounds when food goes through pharynx in a nondysphagic swallowing: two audible clicks follwoed by a expiratory blow. Yet, the author discusses the need of a new lexicon which might help to decribe the sound of swallowing. The term 'busrt' is used to name "clicks" of swallowing and the term 'pop' to identify the noise of high frequencies that occur between bursts of each swallowing. The short length issue, less than 25 s in general, is considered by the author as a time marker when identified through frequency analysis.
Computer is able to show sounds and to process noise produced by swallowing through visual representation in wave format, what allows accurate measures and then a precise description of them.
SABINO (15) describes sound as a propagation of energy by a mechanical wave through environment, i.e., sound is a logitudinal mechanical wave (compressional), in which the movement of particles is parallel to the direction of wave propagation. A sound wave needs the environment to be transmitted. It does not propagate through vacuous, opposed to electromagnetic waves, radio and light, which do not require physical environment to their propagation.
McKAIG (16) says that sound is a mechanical wave that propagates through physical environment. It is produced from a vibrating source. Propagation from source occurs by the vibration of the particles from the environement, alternating compression and rarefaction areas of these particles. When vibration stops, particles go back to rest. In ultrasound event, with a sound wave, particles do not move, they only suffer compression and rarefaction, returning to initial condition after sound stimulus of source stops.
According to TAYLOR (17) the basic principles from Doppler have been long used by detectors of fetal heart frequency (sonar). Posterior development in Doppler technology enlarged its medical application area. Features from blood flow can be accessed by Doppler having waves as typical standard of frequency to medical job in interval of 1 to 5 MHz. A level of average potency to applications in diagnosis is per square centimeters. Pulses of ultrasound are sent to the body placing a vibrating crystal in contact with skin, using water or gel to eliminate air. This provides a good connectin with skin and increases the ultrasound transmission in the body and the echo back to detector.
ZAGZBEBSKI (18) describe Doppler equipment as containg a diagram of simplified block diagram (Picture 5). Transmissor continuously stimulates the ultrasonic transducer with a sinusoidal electric signal of frequency fo. Transducers of ultrasound in medicine use ceramic piezoelectric material in order to generate and detect sound waves.

Picture 1 - Doppler equipment.
Picture 2 - Computer conection.

Picture 3 - Transducer position for evaluation.
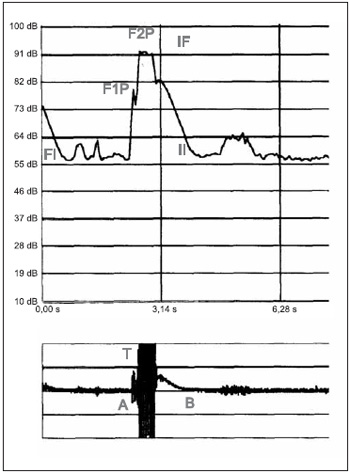
Picture 4 - Sound wave of swallowing captured by Sonar Doppler.
Transducer changes this electrical energy into ultrasonic one, which propagates through the environment. Echo signals resulting from reflection and dispersion go back to the transducer, creating an electrical signal that is applied to amplifying receptor. Inside the amplifier, the signal is intensified and applied to a demodulator and a low-pass filter, whose result is to allow signals of Doppler variations of low frequency to be presented at the output. Output is a complex signal whose frequency is related to velocity of all reflectors and dischargers inside of the beam.
PATIENTS AND METHODFifty normal individuals, with no swallowing complaints, were studied through Sonar Doppler, from February to August, 2003. All analyses were performed at the Phonoaudiology services at Universidade Tuiuti do Paraná - Curitiba
Twenty five patients were female (50%) and the other thwenty five were male (50%). The average age was 32 years, with the minimum of 18 and maximum of 50 years.
All of them were informed about the research and were asked to take part of it. After agreeing, they were also asked to sign a free and clear Consent Ter. This research was submmited to the Comitê de Ética em Pesquisa (Research Ethics Committee) from Universidade Tuiuti do Paraná. Of. CEP-UTP, protocol number 27/2004.
All subjects involved approved the research perfromance and its divulgation according to Law 196/96 - October 10, 1996, which approves researches involving human beings. (Brasil. Resolução MS/CNS/CNEP nº. 196/96 de 10 de outubro de 1996. Aprova diretriz e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília, 1996. 24p.).
Inclusion Criteria: Individuals with no complaints of swallowing established by its clinical evaluation performed by the researcher; both men and women, aging from 18 to 50 years.
Exclusion Criteria: Individual with neurological disease diagnosis and/or submitted to any therapy on head and neck, such conditions were obtained from a questionnaire to collect clinical information.
Sonar Doppler equipmentThe equipment used to perform swallowing study with Sonar Dppler was ULTRASONIC DETECTOR (portable), DF-4001, MARTEC (Picture 6). A transducer of flat disc and single crystal (Picture 1), provides interface to Doppler. Ultrasound frequence by Doppler effect is 2.5 MHz, and output 10 mW/cm². Potency of sound output is 1W.
Doppler continuous equipment was connected to a IBM computer (Picture 2), with a Pentium processor 200 Mhz, 32 MB Ram, video board with high color support (16 bits - 800 x 600), 8x CD-Rom drive, sound board, speakers, Windows 98 and VOX metria Software (12).
Swallowing DefinitionsAll individulas had the same food in terms of cosistence during procedure. It was divided in dry, liquid and pasty swallowing. In each of the three types, it was required three swallowings with intervals of 2 minutes each. The definition was: dry swallowing - it was required individual would swallow saliva. Liquid swallowinf - it was administrated 10 ml of water to each swallow act. Pasty swallowing - 10 ml was used in order to prepare a pasty consistence to be swallowed.
Preparation for Pasty ConsistenceIt was used an instant thickening product Thick & Essy (HORMEL HEATH LABS. SWISS), composed by starch, having as a nutritional composition per 100 g: 375 kcal, 100g carbohidrate and 125 mg sodium.
Following instruction from manufacturer, to achieve pasty consistence, it was combined two tablespoon of starch to 100 ml of water. It was administrated 10 ml of the pasty food to each swallow.
Swallowing Evaluation with Continuous DopplerPatient remained seated with his/her free neck during evaluation. It was followed TAKAHASHI´s recommendation (10) for better placing the transducer, and point number 11, over lateral area of trachea inferiorly after cricoid cartilage at the right side (Picture 3), was chosen as a better adaptation of the transducer and better capture of sound signal. Transducerr was connected to patient´s neck using gel in order to make contact between transducer and skin easier. The transducer beam was placed in order to form an angle from 30° to 60°.
Acoustic Analysis of the Sound Sign of SwallowingVOX METRIA software was used to the acoustic analysis of sound signal, developed by CTS Informática and organized by BEHLAU & MIHAELIS (12). In order to capture sound signal by continuous Doppler equipment, the intensity of sound was number 3, for being the best adaptation to audio signal detected by the software.
Acoustic Parameters The following acoustic parameters were studied: (Picture 4)
• (FI) - Initial Frequency
• (F1P) - First Peak Frequency
• (F2P) - Second Peak Frequency
• (II) - Initial Intensity
• (IF) - Final Intensity
• (T) - Time
1) Initial Frequency (FI) from sound signal was defined as the first trace of the sound wave. In order to represent different types of swallowing, it was chosen the following subtitle: (FI1)- dry swallowing; (FI2)- liquid swallowing (FI3)- pasty swallowing.
2) First Peak Frequency (FIP) was defined as the first peak observed on sound wave from swallowing. Swallowing was defiend as: (FP1)- dry swallowing; (FP2)- liquid swallowing (FP3)- pasty swallowing.
3) Second Peak Frequency was represented as the second peak of the acoustic wave of swallowing. Swallowing was defiend as: (F2P1)- dry swallowing; (F2P2)- liquid swallowing (F203)- pasty swallowing.
4) Initial Intensity (I) was defined as the initial intensity of the acoustic trace recorded by Doppler during swallowing act. Values of intensity were analized in the limit below 10 bB and above 140 dB. Swallowing was defiend as: (II1)- dry swallowing; (II2)- liquid swallowing (II3)- pasty swallowing.
5) Final Intensity (IF) was defined as the final intensity, second peak from the wave recorded by Doppler during swallowing act, obtaining the amplitude from the audio signal. Values of intensity were analized in the limit below 10 bB and above 140 dB. Swallowing was defiend as: (IF1)- dry swallowing; (IF2)- liquid swallowing (IF3)- pasty swallowing.
6) Swallowing time in the acoustic analysis was defined as the one from the point of apnea when swallowing up to expiratory glottic releasing after swallowing, establishing total relation of swallowing as: T:dA (dA - deglutition apnea) according to MACKAIG (1999). Swallowing was defiend as: (T1)- dry swallowing; (T2)- liquid swallowing (T3)- pasty swallowing.
Statistical AnalysisFrequncy, intensity and time data when dry, liquid and pasty swallowing were put into Excel and sent to Statistic program 5,0, in order to develop tables and charts. It was calculated averages, Confidence Interval (CI) which represent results reproductibility in similar sample, in case it was studied again using the same method, with 95% if confiability. Student´s-t test to independent sample was used to significance analysis of values obtained from acoustic parameter average between men and women, considering a = 0.05 (5%), if p< 0.05 of significant difference.
To the level of significance of average from the three food consistence studied, it was used Analysis of variance (ANOVA), considering a = 0.05 (5%), if p< 0.05 of significant difference.
Acoustic ParametersThe variables time, frequency and intensity are repesented in their average, confidence interval of 95% (CI 95%) and standard error.
RESULTSThe initial frequency average (FI1) to dry swallowing was 567 Hz, and Confidence Interval 557.53 - 576.47 Hz and standard error of 33.31; to liquid swallowing, the average was 587Hz (FI2), and Confidence Interval 580.49 - 593.73 Hz and standard error of 23.29; to pasty swallowing the average was 592Hz, and Confidence Interval 585.09 - 599.89 Hz and standard error of 26.04.
To frist peak frequency, 46 individuals (92%) presented an initial peak of acoustic wave where average for swalling (FP1) was 905.92 Hz, and confidence interval of 893.06 - 918.79 Hz and standard error of 43.32. In liquid swallowing, 46 individuals (92%) presented first peak (FP2) with an average of 901 Hz, and confidence interval from 884 Hz to 918 Hz and standard deviation of 56.91. Nevertheless, 49 individuals (98%), in pasty swallowign, presented first peak of wave (FP3) with an average of 885 Hz, and confidence interval from 867Hz to 903 Hz and standard deviation of 62.33.
The frequency average of the second peak of dry swallowing (F2P1) was 1070.37 Hz, and confidenc interval from 1061.60 Hz to 1079.15 Hz and standard error of 30.88; in liquid swallowinf (F2P2) the average was 1095.89Hz, and interval of confidence from 1091.91Hz to 1099.86 Hz and standard error of 13.99; in pasty swallowing (F2P3) the average was 1096.44Hz and interval of confidence from 1089.12 Hz to 1103.77 Hz and standar error of 25.78.
The average of initial and final intensities (II) for dry (II1), liquid (II2) and pasty swallowing (II3) was 51 dB(IC of 95%= 50-52).
Average time for dry swallowing (T1) was 1.331s, and confidence interval from 1.25s to 1.44s and standard error of 0.25; in a 10 ml liquid swallowing (T2), the average was 1.679s, and confidence interval from 1,62s to 1.73s and standard error of 0.20; in a 10 ml pasty swallowing (T3), the average was 1.858s, and confidence interval from 1.82s to 1.89s and standard error of 0.12.
DISCUSSIONAt the present moment there are a great number of technologies available to evaluate several aspects of deglutition function and disfunction. Such technologies allow measuring structure movements in it and also muscular action through space and time aspects. This number of technology can provide analysis of the whole process.
When proposing the use of a new equipment to analyze swallowing sounds, it is necessary a project of a low cost, easy use piece of equipment, with the possiblitiy of interpreting results. Considerations that might help in the development of instrumental equipment were discussed by BLESS (19), who points that there should not be restriction to swallowing mechanism, allowing representation of tipical behavior; in verifying if equipment shows reproductibility when data from the same experiment are collected; in the existence of trustful data, from previous studies; to validate results of the new equipment and garatee that procedure routine from the new equipment prevents unnecessary acts making it efficient.
In the proposal of a new instrumental method to investigate swallowing sounds, it is necessary to know swallowing anatomy and physiology, besides basic knowledge of physics and mechanics in order to correctly handling of the instrument.
The non-invasive instruments for analysis are said to be objective and documentable. BEHLAU (12), when describing laboratories of acoustic analysis, defined the objectivity in terms of rigorous evaluation and also in terms of determining quantity and value. Regarding being documented, the author pointed the number of advantages of a analysis lab: a) it provides larger acoustic comprehension and reduces association between perception-auditive and acoustic analyses; b) it provides normative data to different features, such as age, gender, pathologies; c) it provides enough documentation to trace the individual´s basis; d) it monitors the effectiveness of a therapy and compares results from different procedures; e) it follows development for a period, and f) it works as an instrument of precocious detection of larynx problems. Though, there are limits of interpretation of data that should be followed in order to prevent failures with clinical correlation and with invasive post-instrumental evaluations.
The inclusion of only normal individuals with no complaints of swallowing allows to establish normal standards of acoustic parameters from sound wave of swallowing as well as to establish an information data base for future researches.
TITZE (20) describes that when defining standards, it is important to observe four basic aspects. First, standards teach, i.e., when developing standard data from any nature, it is necessary more attention to the topic, providing knowledge in direct or indirect way. Second, as standards simplify, it is possible to establish reference values in order to reduce variation of a certain studied event. The third aspect is that standards save time and money, and infomation can be achieved from a lager number of individuals. When normatization is established, standards make the use of new technologies more popular and cheaper. The fourth aspect is that standards certify. On the other hand, the author emphazises that standards should be questioned, improved, changed or even discarded, so knowledge can progress.
Knowing wave phenomena from nature (sound, light, etc.) allwed the development of a large quantity of techonology applied to almost all human activity, especially the discovery of Doppler Effect, which allowed an expressive advance when developing new measurement techniques.
As previously mentioned, the utilization of Doppler Effect in ultrasonic waves propagating through biological tissues is the basis of a series of techniques to study movable structures from the interior of human body, in a non-invasive way. ZAGZEBSKI (18) shows that the reception of reflected and diffused echo signals provides information on acoustic properties, what makes production of images possible and allows detection of structure movement in the environment.
It was not found, in the literature, any work that has studied acoustic standards of swallowing caputred by Doppler instrument, with similar technology. Some studies show observation through Doppler of fetus swallowing; sucking baby swallowing (21) and studies of Gastro-oesophageal reflux (GOR) in babies (22), though with no standards of evaluation.
In the next paragraphs, it will be discussed the results from parameters of sound wave of swallowing from evaluation using continuous Doppler.
In the analysis of such standards, the variable gender showed that there was no influence on the acoustic parameters of the sounds of swallowing. Other studies did not identify differences on acoustic standards of swallowing between the two genders as well (13).
The acoustic sign of swallowing can be discussed in terms of signal frequency; amplitude (intensity) and length (time) of the wave.
In relation to features of frequency from swallowing signal, McKAIG (3), highlighted that sound energy of the process is from 0 to 2000 Hz. TAKAHASHI (10), observed two peaks, one below 110 Hz and another in 621 Hz. Therefore, discrepancy was found in the studies by HAMLET (9), where it showed a initial peak of sound in 556 Hz and a second one in 1,384 Hz.
In the current study, it can be idientified, in the acoustic average representation, an initial frequency of the sound signal record with an average of 587 Hz. This representation is discussed by CICHERO & MURDOCH (13) as the first frequency of ressonance of the vocal tract in about 500 Hz.
The initial peak of the wave was 905 Hz to dry swallowing (FP1); average of 901 Hz to liquid swallowing (FP2) and 885 Hz to pasty one. It can be observed, in these data, an inverse ratio from a more fluid consistency to pasty one, the greater the consistency the minor the sound representation of frequency. From the 50 evaluated individual, 46 (92%) presented the first peak in dry swallowing, 46 (92%) in the liquid one and 49 (99%) in the pasty one. HAMLET (8) establishes the initial peak of wave as a weak signal associated with a laryngeal uprising and with food passage through pharynx.
The second peak or final peak of the wave, the average in dry swallowing (FF1) was 1,070 Hz; the final frequency to liquid swallowing (FF2) was 1,095 Hz and the final frequency to pasty one was 1,096 Hz. In HAMLET´s viewpoint (8), this signal represents a strong sound associated with cricopharyngeal opening.
The data from frequency of initial and final peak agree with findings by Hamlet (14).
In the analysis of acoustic representations from sound wave, the amplitude (intensity) of wave was observed and it was identified an initial intensity of 51 dB. In the acoustic signal record it was identified a final intensity of sound wave of 91 Hz to saliva, liquid and pasty swallowing.
Regarding acoustic signal length, studies point differences when swallowing liquid and pasty food (3). Researchers agreed that signal length to liquid swallowing is 500 ms. McKAIG (3), says that time length is specific for each individual, thus some people can present a type of swallowing that lengths 1 second, while others 3 seconds, without presenting dysphagia.
In this study, it was observed that time length to dry swallowing (saliva) is - T1 = 1.33 s; to a 10 ml liquid swallowing T2= 1.67 and to a 10 ml pasty one T3= 1.85 s. It is possible to identify that swallowing time length is greater according to material consistency.
Data from this study show the viability of continuous Sonar Doppler use as an auxiliary instrument for evaluating sounds of swallowing. It can be identified acoustic parameters of swallowing from normal adults.
Sonar Dopller, for not being invasive and cheap, is a promising method of therapy diagnosing and monitoring for adults, children and babies. With no doubt, information collected did not depend only on the experience of the examiner but also on the proper use of the technique and on the instrument. Future investigations on acoustic standards of swallowing obtained from Sonar Doppler in dysphagia and in children should be encouraged.
The acoustic analysis is the product from all equipment conditions, methodology and from the examiner associated with physiological and physiopathological events of swallowing. The acoustic analysis brings forth contribution to swallowing studies, qualifying and quantifying the development of swallowing disorders. And it has also been more demanded and discussed regarding scientific area.
Phonoaudiology is in constant development, presenting its clinical and scientific growth. Treating swallowing disorders requires important performance by the speech doctor who should integrate the whole team. The ability to select a proper therapy planning is connected to the abitliy of performing a comprehensive and detailed evaluation, as well as relating results with findings from complementary exams of diagnosis.
CONCLUSIONSOne can conclude, according to the analysis of sounds of swallowing using Sonar Dopller that:
1 - Frequency, amplitude and time length standards of sound wave were:
1.1. 567 Hz to dry swallowing; 587.11 Hz to a 10 ml liquid swallowing and 592.49 Hz to a 10 ml pasty one regarding initial frequency of swallowing;
1.2. 905.92 Hz to dry swallowing; 901.25 Hz to a 10 ml liquid swallowing and 885.51 Hz to a 10 ml pasty one regarding first peak of swallowing;
1.3. 1070.37 Hz to dry swallowing; 1095.89 Hz to a 10 ml liquid swallowing and 1096.44 Hz to a 10 ml pasty one regarding second peak of swallowing;
1.4. 52.85 Hz to dry swallowing; 50.93 Hz to a 10 ml liquid swallowing and 52.01 Hz to a 10 ml pasty one regarding initial intensity of swallowing;
1.5. 91.12 Hz to dry swallowing; 91.81 Hz to a 10 ml liquid swallowing and 91.07 Hz to a 10 ml pasty one regarding final intensity of swallowing;
1.6. 1.33s to dry swallowing; 1.67s to a 10 ml liquid swallowing and 1.85s to a 10 ml pasty one regarding time length of swallowing;
2 - The differences of frequency, amplitude and time length of sound wave feom dry (1), liquid (2) and pasty (2) swallowing presented statistical significance of p=0.167063, except frequency of the first peak.
Data from this study show the viability of continuous Sonar Doppler use as an auxiliary instrument for evaluating sounds of swallowing. It can be identified acoustic parameters of swallowing from normal adults.
Sonar Dopller, for not being invasive and cheap, is a promising method of therapy diagnosing and monitoring for adults, children and babies. Future investigations on acoustic standards of swallowing obtained from Sonar Doppler in dysphagia and in children should be encouraged.
With no doubt, the acoustic analysis brings forth contribution to swallowing studies, qualifying and quantifying the development of swallowing disorders. And it has also been more demanded and discussed regarding scientific area.
Treating swallowing disorders requires important performance by the speech doctor who should integrate the whole team. The ability to select a proper therapy planning is connected to the abitliy of performing a comprehensive and detailed evaluation, as well as relating results with findings from complementary exams of diagnosis.
REFERENCES1. Macedo-Filho ED. Estudo comparativo entre a Videoendoscopia da Deglutição (VED) e a Videofluoroscopia (VFC) na Avaliação da Disfagia Orofaríngea Pós-Acidente Vascular Cerebral (AVC). Curitiba, 2001.
2. Hartnick CJ, Hartley BEJ, Miller C, Willging JP. Pediatric Fiberoptic Evaluation of Swallowing. Ann Otol Rhinol Laryngol, v. 109, p 996-999, 2000.
3. McKaig TN. Ausculta - Cervical e Torácica. In: Furkin AM & Santini CS. Disfagias Orofaríngeas. Pro-Fono, S.P., 1999, p 171-187.
4. Crary MA & Baldwin BO. Surface Eletromyographic Characteristics of Swallowing in Dysphagia Secondary to Brainstem Stroke. Dysphagia, n 12, p 189-187, 1997.
5. Brown PB & Sonies BC. Diagnostic Methods to Evaluate Swallowing Other Than Barium Contrast. P. 227-253. In: Perlman AL & Schulze-Delrie K. [eds]. Deglution and its disorders. Singular Publishing Group Inc., San Diego, 1997.
6. Burke AJ et al. Evaluation of Arway Obstruction Using Virtual Endoscopy. Laryngoscope, v. 1110, p.23-29, 2000.
7. Hamlet SL, Nelson RJ, Patterson RL. Interpreting the sounds of swallowing; fluid flow through the cricopharyngeus. Ann. Otol. Rhinol. Laryngol., 99.749-52, 1990.
8. Hamlet SL, Patterson RL, Fleming SM, Jones LA. Sounds of swallowing following total laryngectomy. Dysphagia, n 7, p 160-165, 1992.
9. Vice FL, Heinz JM, Giuriat G, Hood M, Bosma JF. Cervical auscultation of sucke feeding in newborn infants. Dev Med Child Neurol 1990, 32:760-768.
10. Takahashi K, Groher ME, Michi K. Methodology for detecting swallowing sounds. Dysphagia, n 9, 54-96, 1994.
11. Russo ICP. Acústica e Psicoacústica Aplicadas à Fonoaudiologia. São Paulo: Editora Lovise, 1993.
12. Behlau & Michalis. VoxMetria - Software para Análise de Voz e Qualidade Vocal. CTS Informática, São Paulo, 2003.
13. Cichero JA, Murdoch BC. The phisiologic cause of swallowing sounds: Answer from heart sounds and vocal tract acoustics. Dysphagia. New York: n 13, p 39-52, 1994.
14. Hamlet SL, Penny DG, Formolo J. Stethoscope acoustic and cervical auscultation of swallowing. Dysphagia, n 9, p 44-51, 1994.
15. Sabino E,Araújo MJM, Hirsch R. Bases da Terapia Intensiva Neurológica. Cap.22. São Paulo : Livraria Santos, 1993.
16. McKaig TN & Stroud A. The comparison of swallowing sounds with simultaneously recorded fluroscopic imaging. Annual Meeting of the Dysphagia Society, 5. 1996. p 31.
17. Taylor KJW, Burns P, Wells PNT. Clinical Applications of Doppler Ultrasound. New York: Raven Press, 1988.
18. Zagzebski JA. Física e Instrumentação em Ultra-Sonografia pelo Dopple e pelo Modo-B. In: Zwielbel, WL. Introdução à Ultra-Sonografia Vascular. 3ed. Rio de Janeiro: Revinter, 1996.
19. Bless DM. Videostroboscopic Examination of the Larynx, Singular Publlishing, San Diego, l993.
20. Titze IR. Principles of Voice Production, Prentice Hall, Englewood Cliffs,1994.
21. Shaker TH, Sonies B, Stone M & Baum BJ. (1983) Realtime ultrasound visualization of tongue movement during swallowing. Journal of Clinical Ultrasound, Philadelphia: 11, 485-90, 1988.
22. Hirsch W, Kedar R, Preib U. Collor doppler in the diagnosis of the gastroesophageal reflux in children comparison with pH measurements and B-mode ultrasound. Pediatr Radiol 26:232,1996.
1. Master in Communication Disorder (Professor in the Phonoaudiology Course at Universidade Tuiuti - Paraná - Coordenator of post-graduation in Dysphagia)
2. PhD in Surgical Medicine by UFPR (ENT and Endoscopy doctor and PhD in Surgical Medicine by UFPR - Universidade Tuiuti - Paraná - Master Professor of Communication Disorder at UFPR)
Universidade Tuiuti do Paraná
Address: Rua Padre Oswaldo Gomes, 754 casa 3 Bairro Guabirotuba Curitiba Paraná CEP 80510100
This article was submitted to SGP - Sistema de Gestão de Publicações (Publication Management System) from RAIO on March 19, 2006 and was approved on August 20, 2006 13:32:18.

