INTRODUCTIONRespiratory function is the main subject of the phonoaudiology rehabilitation in the area of oral motricity(1-4).
Nose breathing is fundamental for proper development growth of the craniofacial complex, by providing good performance of the other stomatognathic functions(1,2,4,5,6).
The one who comes into an oral or oralnasal standard of breathing might develop dental or craniofacial changes, alterations on phonoarticulatory and oral activities, and body alteration in some of the cases 1,4-11).
Nasal and/or pharyngeal obstructions are the most frequent causes of oral breathing (1). Rhinitis diseases are the most frequent occurrence among nasal obstructions, some studies have even report their progressive spreading(12).
There are the allergic and non-allergic groups of rhinitis, and these two groups are divided into infective, non-allergic eosinophilic, idiopathic, irritative, hormonal ones, etc(12).
Allergic rhinitis is a nasal mucosa, with IgE in between, after being exposed to antigen substance. Its main characteristics are nasal obstruction (as usual the predominant symptom (13-17)), itching, sneezes and coryza.
According to the literature, there is a correlation between rhinitis and nasal obstruction (14,15,16,17,20) and the latter between morphofunctional alterations of the stomatognathic system (7,8,10,18,19), although few studies have reported such alterations on patients with rhinitis (21).
The target of this study was to verify alteration of respiratory, chewing and swallowing activities which are present in patients with allergic rhinitis from different ages and also to relate them with the intensity symptoms.
MATERIAL AND METHODThe current study was approved under protocol #355/06 by the Ethics Committee (CAPPesq) of the HCFMUSP.
This study was transversal-cut-based, in which 85 male and female patients aging from 4 and 60 year were analyzed. Patients were diagnosed with allergic rhinitis and assisted at Grupo de Alergia da Divisão de Clínica Otorrinolaringológica of HCFMUSP (Allergy Department of the ENT Clinic).
Patients who presented with neurological, neuromuscular, motor or skeletal alterations, or any other syndrome or disease did not take part in this study, unless patients with allergic rhinitis with nasal obstruction as associated symptom.
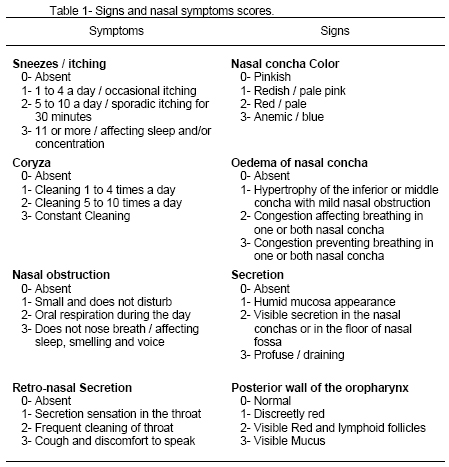
Patients were examined by an ENT doctor and data consisted of: age, gender and scores of signs and nasal symptoms (14,15) (Table 1).
Patients then were examined by a speech doctor who established data regarding oral breathing, chewing and swallowing activities and gathered information on patients' eating references.
Respiration was established by observing patient during phonoaudiological evaluation according to information provided by them or their companion. Respiration was classified as:
0) Nasal (day and night)
1) Oronasal (day and night)
2) Oronasal (day) and oral (night)
3) Oral (day and night).
Chewing activity, which was evaluated through a biscuit mastication, was classified as:
0) Normal, when lips were closed in bilateral way
1) Open mouth
2) Open mouth followed by food crushing with tongue
3) No chewing.
Swallowing, which was evaluated through observation of a glass of water deglutition, was classified as:
0) Normal, when closed lips, tongue placed on the palate and no periorbicular muscle use
1) Anterior projection of the tongue
2) Anterior projection of the tongue followed by periorbicular muscle tension or
3) Interposition
As a complementation of the masticatory standard evaluation, alimentary consistence was determined through information provided by patients or their companion. Such information was classified as:
1) Preferably solid
2) Preferably solid with inefficient food chewing (food pieces swallowing)
3) Preferably pasty
4) Preferably pasty (presence of choking)
At last, patients were divided into three groups, according to age: G1-children from 4 to 11 years old; G2-adolescents from 12 to 18 years old; G3-adults from 19 to 60 years old.
Data regarding respiratory, chewing and swallowing activities were compared in the three age groups through the Probability Ratio Test in order to verify the difference of the variables of each activity among the groups.
The sign and symptoms figures were also compared in the three groups through Kruskal-Wallis test in order to observe significant statistical difference among these score averages.
Spearman's rho test was used to verify the correlation between symptoms intensity of allergic rhinitis and the degree of activity alterations.
RESULTSIn the 85 evaluated patients, the average age was 7.6 years (+/- 2.3 years) in the children's group; 13.2 years (+/- 1.6 years) in the adolescents' group and 29.2 years (+/- 10.2 years) in the adults' group.
Gender distribution in the groups is displayed on Table 2.
Charts I and II display comparison of score average achieved during ENT evaluation, regarding signs and symptoms caused by allergic rhinitis (in the analyzed groups).
Chart I. Distribution of sign and symptoms scores - Signs: p = 0.910 Symptoms: p= 0.236.
Chart II. Distribution of total score - p = 0.399.
Table 3 displays a higher occurrence of nasal obstruction absence in the children's group and a higher occurrence of nasal obstruction (scoring 3) in the adolescents' group.
Regarding respiration, it was in accordance with nasal obstruction score in the three groups. It was noticed a high occurrence of nasal breathing during night and day in the children's group and a high occurrence of oral breathing during night and day in the adolescents' one (Chart IV).
Chart III. Distribution of breathing manner - p = 0.014*
Chart IV. Distribution of chewing manner - p = 0.173.
Normal swallowing was reported in 20% of the children, in 23.3% of the adolescents and in 20% of the adults. Presence of anterior mild projection during swallowing was reported in 43.3% of the children, in 36.7% of the adolescents and in 52% of the adults. Anterior projection associated to excessive use of periorbicular muscles was reported in 23.3% of the children, in 30% of the adolescents and in 24% of the adults. Presence of anterior interposition was reported in 13.3% of the children, in 10% of the adolescents and in 4% of the adults. There was no significant statistical difference among the above data (p = 0.861).
Charts IV and V display chewing activity and food consistence preferences among the three groups. It was noticed a high occurrence of open mouth masticatory standard and food crushing in the children's group and a significant statistical difference in children with pasty consistence food preference.
Chart V. Distribution of food consistence preference - p = 0.042*.
At last, it was observed the correlation between score increase of nasal obstruction and alteration intensity of breathing, chewing and swallowing activities. Significant correlation for breathing and chewing activities was (p < 0.001).
DISCUSSION By studying distribution of gender (Table 2), it was noticed a higher number of male in the children's and adolescents' groups. The same result was found by Di Francesco and col. (22) when studying 142 patients aging from 2 and 16 years. Yet, in the adults' group the lower of male could be explained due to fewer occurrences of allergic rhinitis symptoms for men and due to less time availability for searching assistance.
To observe and measure signs and symptoms of allergic rhinitis is important due to the fact that such disease is clinically classified as a sum of several of those signs and symptoms (12,16). In the current study, the frequency and intensity of such signs and symptoms did not present with significant statistical difference when compared to the score averages among the evaluated groups (Chart I and II), by showing that regardless age, patient can present signs and symptoms of same intensity as the ones from allergic rhinitis.
By analyzing distribution of nasal obstruction score (Table 3), the adolescents' group presented percentage rate higher than 3 for such symptom. The same result was reported in the breathing manner study (Chart III), when patients of the same age presented percentage rate higher than the exclusive oral breathing manner. It is believed that such results might show the low attendance of patients for therapy suggested by doctors, which does not provide improvement of nasal ventilation and a predominance of oral breathing standard. Though, it was not found studies reporting the same results in the literature.
Several studies have already reported clinical implications and orofacial alteration on patients with oral respiration (8,16,23,24,25), thus, the high occurrence of patients with oronasal and oral breathing, in the current study, prearrange them to functional alterations.
Junqueira and col (2002) studying patients aging from 2 to 13 years who suffered from adenotonsillar hypertrophy, reported 85.5% of alteration on masticatory activity and 78.1% on swallowing standard. The current study reported 40% of alteration on chewing activity in the children's group (chart IV) and 80% of alteration on swallowing standard despite the difference regarding obstruction condition of patients from the above mentioned study.
Food consistence preference analysis is extremely important for oral breathing patients (4-6, 26), as they present with difficulty in chewing solid food due to alteration on masticatory standard. The current study data agree on these findings, mainly for the children's group, in which there is a higher rate of pasty food preference (Chart V).
By comparing data of chewing and swallowing alteration in the three groups (Chart III and IV), significant statistical difference was not reported, which confirmed the similarity found between the sign and symptom scores and showed that functional alterations are present on patients with allergic rhinitis, regardless age. Such data were confirmed by the correlation found on the scores between nasal obstruction and degree of alterations on breathing manner and chewing standard for all groups.
CONCLUSION Based on the result analysis, it is concluded:
- Patients with allergic rhinitis present with alterations of breathing, chewing and swallowing activities.
- The increase on nasal obstruction symptoms is related to the presence of functional alterations.
REFERENCES 1. Marchesan IQ. Avaliação e terapia dos problemas respiratórios. Em: Marchesan IQ. Fundamentos em Fonoaudiologia: aspectos clínicos da motricidade oral. Rio de Janeiro: Guanabara-Koogan; 1998. p.23-36.
2. Marchesan IQ, Krakauer LRH, Di Francesco RC. Respiração Oral: abordagem interdisciplinar. São Paulo: Pulso; 2003. p.167.
3. Comitê de Motricidade Oral da Sociedade Brasileira de Fonoaudiologia. Em: Documento Oficial 02/2002; 2002. p.35.
4. Marchesan IQ, Krakauer LRH. A importância do trabalho respiratório na terapia miofuncional. Em: Tópicos em Fonoaudiologia. São Paulo: Lovise; 1995. p.155-160.
5. Rahal A, Krakauer LRH. Avaliação e terapia fonoaudiológica com respiradores orais. Em: Tópicos em Fonoaudiologia. Rio de Janeiro: Revinter; 2003. p.261-267.
6. Tanigute C.C. Desenvolvimento das funções estomatognáticas. Em: Marchesan IQ. Fundamentos em Fonoaudiologia: aspectos clínicos da motricidade oral. Rio de Janeiro: Guanabara-Koogan; 1998.p.1-6.
7. Junqueira PAS, Di Francesco RC, Trezza P, Zeratti FE, Frizzarini R, Faria MEJ. Alterações funcionais do sistema estomatognático pré e pós-adenoamigdalectomia. Pró-fono 2002; 14(1):17-22.
8. Coelho MF, Terra VHTC. Implicações clínicas em pacientes respiradores bucais. Rev Bras Patol Oral 2004; 3(1):17-19.
9. Di Francesco RC. Respirador bucal: a visão do otorrinolaringologista. J. bras ortodon ortop facial 1999; 4(21):241-247.
10. Cintra CFSC, Castro FFM, Cintra PPVC. Alterações oro-faciais apresentadas em pacientes respiradores bucais. Rev bras alergia imunopatol 2000; 23(2):78-83.
11. Krakauer LRH. Relação entre respiração bucal e alterações posturais em crianças: uma análise descritiva [dissertação]. São Paulo (SP): Pontifícia Universidade Católica de São Paulo; 1999.
12. Mello Jr JF, Mion O. Rinite Alérgica. Em: Campos CAH, Costa HOO. Tratado de Otorrinolaringologia. São Paulo: Rocca; 2002. p.68-87.
13. Bozkurt B, Karakaya G, Kalyonai AF. Seasonal rhinitis, clinical characteristics and risk factors for asthma. Int Arch Allergy Immunol 2005; 138(1):73-79.
14. Balbani APS; Mello Júnior JF; Mion O; Butagan, O. Atualização em rinites. RBM - Revista Brasileira de Medicina 2002; 59:2-13.
15. Costa GGO, Ctenas B, Mion O, Mello Júnior JF. Comparação entre a rinometria acústica e o peak flow nasal inspiratório frente à correlação com sintomatologia e sinais clínicos em pacientes com rinite. Arq Otorrinolaringol. 2005; 9(3):203-11.
16. Sollé D, Mello Júnior JF, Weckx LLM, Rosário Filho NA. II Consenso sobre rinites 2006. Rev. Bras. Alerg. Imunopatol. 2006; 29(1).
17. Fomin ABF, Souza RGL, Fiorenza RF, Castro APBM, Pastorin AC, Jacob CMA. Rinite perene: avaliação clínica e epidemiológica de 220 pacientes em ambulatório pediátrico especializado. Rev bras alergia imunopatol 2002; 25(1):10-15.
18. Ciprandi G, Marseglia GL, Klersy C, Tosca MA. Relationship between allergic inflammation and nasal airflow in children with persistent allergic rhinitis due to mite sensitization. Allergy 2005; 60(7):957-960.
19. Berger WE. Allergic rhinitis in children: diagnosis and management strategies. Paediatr Drugs 2004; 6(4):233-50.
20. Amaral CSF, Martins ER, Rios JBM. A respiração bucal e o desenvolvimento do complexo dentofacial. Rev bras alergia imunopatol 2002; 25(4):131-135.
21. Freitas FCN, Bastos EP, Primo LS, Freitas VL. Evaluation of the palate dimensions of patients with perennial allergic rhinitis. Int J Paediatr Dent 2001; 11(5):365-71.
22. Di Francesco RC, Passerotti G, Paulucci B, Miniti A. Respiração oral na criança: repercussões diferentes de acordo com o diagnóstico. Rev Bras Otorrinolaringologia 2004; 70(5).
23. Ferreira LP, Silva MAA, Natalini V, Ramires RR. Análise comparativa da mastigação de crianças respiradoras nasais e orais com dentição decídua. Revista Cefac 2007; 9(2).
24. Lessa FCR, Enoki C, Feres MFN, Valera CP, Lima WTA, Matsumoto MAN. Influência do padrão respiratório na morfologia craniofacial. Rev Bras Otorrinolaringol. 2005; 71(2):156-60.
25. Cintra, CFSC, Castro FFM, Cintra PVC. As alterações oro-faciais apresentadas em pacientes respiradores orais. Rev bras alergia imunopatol 2000; 23(2):78-83.
26. Tomé MC, Marchiori SC, Pimentel R. Mastigação: implicações na dieta alimentar do respirador bucal. J Bras Fonoaudiol. 2000; 3:60-5.
1. Master degree student - Speech Doctor at the ENT department of HCFMUSP.
2. Teacher at HCFMUSP - Assistant at ENT department of HCFMUSP.
3. PhD by HCFMUSP. Assistant at the ENT Department of HCFMUSP.
HCFMUSP - Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo - Hospital of Medical School of University of São Paulo.
Study done at the ENT Department of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo
Fga. Catiane Maçaira de Lemos
Address: Rua Pde. Estevão Pernet, 783, Tatuapé, São Paulo/SP - Phone: (11) 2294-2725 - E-mail: catianemacaira@terra.com.br
This article was submitted to SGP (Sistema de Gestão de Publicações - Publication Management system) of R@IO on June 24th, 2007 and approved on October 10th, 2007 at 23:17:01.