INTRODUCTIONThe diagnosis of a Chronic Rhinosinusitis (CRS) was difficult to achieve for many years for being based only on isolated symptoms. After some time, there was a need of a more accurate diagnosis. Then the association of signs and symptoms was used to perform such diagnosis, as CRS would affect more than 30 million of Americans and costing US$3.4 billion per year in medical appointment(1).
American Academy of Otorhinolaryngology-Head and Neck Surgery (AAO-HNS), American Academy of Otorhinolaryngologic Allergy (AAOA) and American Rhinologic Society (ARS) met in 1996 with the purpose of developing a consensus in task force. In 1997, soon after the meeting, it was published "Definitions of Rhinosinusitis in Adults"(2). Such consensus classified rhinosinusitis in five clinical categories: acute; sub acute; chronic, recurrent acute and acutized chronic one. New studies on rhinosinusitis origins have been changing this classification into acute bacteria sinusitis, CRS with polyps and CRS without polyps(3). Acute rhinosinusitis presents clinical symptoms in less than 4 weeks; the sub acute one in more than 4 and less than 12 weeks and the chronic rhinosinusitis in more than 12 weeks.
Besides evolution time, there is the association of symptoms (from the AAO-HNS consensus) for diagnosing CRS (Table 1), being 2 or more higher criteria, 1 higher criterion and 2 or more minor criteria needed to confirm it.
Rhinosinusitis in Adults"(2). Such consensus classified rhinosinusitis in five clinical categories: acute; sub acute; chronic, recurrent acute and acutized chronic one. New studies on rhinosinusitis origins have been changing this classification into acute bacteria sinusitis, CRS with polyps and CRS without polyps(3). Acute rhinosinusitis presents clinical symptoms in less than 4 weeks; the sub acute one in more than 4 and less than 12 weeks and the chronic rhinosinusitis in more than 12 weeks.
Besides evolution time, there is the association of symptoms (from the AAO-HNS consensus) for diagnosing CRS (Table 1), being 2 or more higher criteria, 1 higher criterion and 2 or more minor criteria needed to confirm it. Although CRS diagnosis is clinic and symptom-based, it was necessary to perform complemental exams in order to confirm diagnosis and also to indicate severity and origin of the disease. Then CT scan and nasal endoscopy were performed. They also helped to identify anatomical abnormalities(4).
OBJECTIVETo compare tomographic with endoscopic findings in patients with clinical diagnosis of CRS.
MATERIAL AND METHODSIn order to select 45 patients clinically diagnosed with CRS, it was used a study protocol with questions which covered the diagnostic criteria of chronic rhinosinusitis. This questionnaire was based on the consensus confirmed by the American Academy of Otorhinolaryngology, in 1997 (Table 2), and it was applied to patients assisted at Otorhinus Clinic.
Regarding inclusion criteria of patients, 35 of them presented 2 or more higher criteria or 1 higher criterion and 2 or more minor ones. All patients with previous rhinosinusal surgery history were not selected (10 patients).
After being selected, patients were submitted to nasofibroscopy exam and after that to paranasal sinus CT, with no previous therapy or preparation.
It was used flexible Mashida nasofibroscope to perform nasal fibroscopy and the protocol by Stankiewicz and Chow to classification(Table 3).
Endoscopy exam evaluated frontal recess, meatus variations, sphenoethmoidal recess and nasopharynx, being considered any possible abnormality.
In order to perform CT scan, it was used the tomographic classification by Metson and Gliklich(6) based on the international protocol of AA)-HNS(Table 4).
In the positive finding of CT, it was considered when disease reached at least the stage 1 of the protocol.
The tomographic and endoscopic analysis was preformed by an ENT doctor who had no precious knowledge of each case.
RESULTS17 (48.5%) women and 18 (51.5%) men (average age: 40) were evaluated. 10 of them were eliminated for reasons already mentioned.
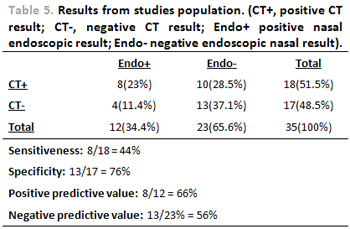
Results are displayed in table 5. 18 patients presented positive result on tomographic analysis and 17 presented negative one. Eight patients (23%) presented positive results on endoscopic analysis and on CT scan. Four of them (11.4%) presented positive results on endoscopy exam but negative ones on CT. Twelve patients (34.4%) presented positive endoscopic results and 23 (65.6%) presented negative ones. Ten patients (28.5%) presented CT positive results and negative endoscopic ones. Thirteen patients (37.1%), presented negative results for both CT and endoscopy exam.
DISCUSSIONNasosinusal alterations can course along with chronical rhinosinusitis as anatomical alterations (presence of Haller cell, paradoxical or bullosa middle concha, etc), nasal polyps, dyskinesia ciliary and others. That is why precisely diagnose CRS is still a challenge for the ENT physicians. American Academy of Otorhinolaryngology-Head and Neck Surgery came together in 1997 with the purpose of develop criteria for its diagnosis. According to their consensus, the criteria are based on subjective symptoms. Thereafter, it was suggested the division between CRS with and without polyps(3). That was the reason of a need to use complemental exams to diagnostic confirmation and therapy planning, depending on nasosinusal alterations found. Paranasal sinus and nose CT scan and nasosinusal endoscopy are the exams chosen to perform this evaluation.
In the literature, there is no consensus on the correlation between reported symptoms by patients and tomographic and endoscopic findings. Nassar et al (7) analysed 200 tomographic exams and concluded that findings do not necessarily mean CRS disease, thus 50% of the case had topographic alterations, but only 25% with CRS simultaneously. Vogel's et al(8), Stewart and Johnson(9) and Prune X(10) found similar results. Hwang ET al(4), on the other hand, carried a vast revision of the literature and reported that there is no consensus on the association.
There was no significant statistical correlation (seen in Table 5) for endoscope topographic alterations, unless patients had expressive alteration as polyp sis, purulent secretion, polypoid mucosa. With all this, it is observed correlation only between number of affected sinus and intensity of referred symptoms. The blockage of the osteomeatal complex is also related to symptoms and tomographic finding severity, which can indicate the importance to perform complemental exams to investigate it, mainly to dismiss polyposis, as suggested by Meltzer et al(3).
The therapy paradigm of all patients with clinical criteria of CRS is under questions, thus almost 50% of them had negative tomographic alterations and 65% with negative endoscopy exam. The association between them was not expressive as well, with sensitiveness of 44% and specificity of 76%. Although this might occur, they are still the best methods to evaluate patient and establish proper therapy.
CONCLUSIONBy analyzing the reported findings, nasal endoscopy is good only to confirm CRS in patients with supplied criteria. In case patients present polyposis, purulent secretion or congested mucosa, nasal endoscopy is good for CT scan.
By making use of the consensus by AAO-HNS associated to CT scan and nasal endoscopy, one might achieve a more precise diagnosis of CRS and then trace a plan of proper therapy in order to heal the disease. Thus, cost would be reduced and use of antibiotics would be made in a correct way.
That is why AAO-HNS board realized the need of developing a diagnosis protocol of CRS, in order to guide both ENT professionals and all other areas when diagnosing CRS.
REFERENCES1. Benninger MS; Ferguson BJ; Hadley JA; Hamilos DL; Jacobs M; Kennedy DW; Lanza DC; Marple BF; Osguthorpe JD; Stankiewicz JA; Anon J; Denneny J; Emanuel I; Levine H - Adult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg 2003, 129:S1-32.
2. Report of the Rhinosinusitis Task Force Committee Meeting. Alexandria, Virginia, August 17, 1996. Otolaryngol Head Neck Surg 1997, 117:S1-68.
3. Meltzer EO; Hamilos DL; Hadley JA; Lanza DC; Marple BF; Nicklas RA; Bachert C; Baraniuk J; Baroody FM; Benninger MS; Brook I; Chowdhury BA; Druce HM; Durham S; Ferguson B; Gwaltney JM; Kaliner M; Kennedy DW; Lund V; Naclerio R; Pawankar R; Piccirillo JF; Rohane P; Simon R; Slavin RG; Togias A; Wald ER; Zinreich SJ; American Academy of Allergy, Asthma and Immunology; American Academy of Otolaryngic Allergy; American Academy of Otolaryngology-Head and Neck Surgery; American College of Allergy, Asthma and Immunology; American Rhinologic Society - Rhinosinusitis: Establishing definitions for clinical research and patient care. Otolaryngol Head Neck Surg 2004, 131:S1-62.
4. Hwang PH; Irwin SB; Griest SE; Caro JE; Nesbit GM - Radiologic correlates of symptom-based diagnostic criteria for chronic rhinosinusitis. Otolaryngol Head Neck Surg 2003, 128:489-96.
5. Stankiewicz JA; Chow JM - Nasal endoscopy and the definition and diagnosis of chronic rhinosinusitis. Otolaryngol Head Neck Surg 2002, 126:623-7.
6. Metson R; Gliklich RE; Stankiewicz JA; Kennedy DW; Duncavage JA; Hoffman SR; Ohnishi T; Terrell JE; White PS - Comparison of sinus computed tomography staging systems.Otolaryngol Head Neck Surg 1997, 117:372-9.
7. Nassar Filho, Jorge; Anselmo-Lima, Wilma T; Santos, Antônio C. - Participaçäo das variaçöes anatômicas do complexo ostiomeatal na gênese da rinossinusite crônica, analisadas por tomografia computadorizada. Rev. bras. otorrinolaringol 2001, 67:489-495.
8. Voegels, Richard L; Goto, Elder Y; Chung, Daniel; Nita, Luciana M; Lessa, Marcus M; Butugan, Ossamu. Correlaçäo etiológica entre variaçöes anatômicas na tomografia computadorizada e a rinossinusite crônica. Rev. bras. otorrinolaringol 2001, 67:507-510.
9. Stewart MG; Johnson RF- Chronic sinusitis: symptoms versus CT scan findings. Curr Opin Otolaryngol Head Neck Surg 2004, 12:27-9.
10. Pruna X - Morpho-functional evaluation of osteomeatal complex in chronic sinusitis by coronal CT. Eur Radiol 2003, 13:1461-8.
1. 3rd year Resident ENT Doctor by Otorhinus Clinic
2. Master degree ENT doctor (preceptor of the Otorhinus Clinic)
3. 3rd year Resident ENT Doctor by Otorhinus Clinic
4. 2nd year Resident ENT Doctor by Otorhinus Clinic
5. 1st year Resident ENT Doctor by Otorhinus Clinic
6. 1st year Resident ENT Doctor by Otorhinus Clinic
Otorhinus Clinic
Rafael José Geminiani
Mail Address: Rua Cubatão, 1140 Vl. Mariana, Cep: 04013-004 - São Paulo/SP Phone: (11) 5572-0025 - Fax: (11) 5572-7373 - Cel: (15) 9774-7503 - E-mail: rafaelgeminiani@ig.com.br
This article was submitted to SGP (Sistema de Gestão de Publicações - Publication Management system) of R@IO on August 6th, 2007 and approved on October 27th, 2007 at 12:44:53.