INTRODUCTIONIn this article we present the case of a patient with nasal obstruction and bilateral bubble-like inferior turbinates, with large communication with maxillary sinuses and their surgical approach. It's a very uncommon clinical state with a very few cases described. In the English language literature 12 cases were described of bubble-like inferior turbinates, 06 of which were bilateral.
Nasal obstruction is one of the most common complaints in otorhinolaryngological consultations and it's proportionally related to the nasal cavities resistance. This in turn has as its main factor the inferior turbinates hypertrophy, in its anterior region (1), that makes the nasal valve region the minor diameter of the aerial column of the upper airways.
The inferior turbinates are composed of internal portion formed by the spongiform turbinate bone that articulates with the maxilla nasal surface and the palatine bone perpendicular lamina; and through the external portion that covers the bone, the mucous surface with an expansive capacity (2). The IT play an important role in the nasal physiology and for protection of the airways, by providing moistness and inhaled air temperature regulation. Both osseous and mucous components may, separately or jointly (more common), be responsible for the inferior turbinates hypertrophy, by manifesting clinically by the nasal obstruction.
The ITs may be classified in tomography according to their osseous configuration (3) in Type I, or lamellar, with the bone characterized by a thin lamella; Type II, or compact, with a voluminous osseous mass; Type III, mixed, combining the previous types characteristics; and Type IV, a rare variation of the inferior turbinate, the bubble-like type that has been diagnosed incidentally by the diffusion of the computed tomography (CT) (4).
CASE REPORT18-year-old, male patient presented in our service with a significant bilateral nasal obstruction without response to medication therapy. Without history of sinusopathy or nasosinusal surgery. He presented inferior turbinates hypertrophy and an intense septal deviation to the left upon anterior rhinoscopy.
The preoperative routine endoscopic exam appointed obstructive and non-responsive inferior turbinates volumetrically upon vasoconstriction, as well as septal deviation.
In the paranasal sinuses CT (Picture 1) we found bilaterally bubble-like inferior turbinates (pneumatized), both with a wide connection of its osseous cavity with the ipsilateral maxillary sinus.

Picture 1. Coronal CT showing the inferior turbinates pneumatization.
During the operative action we corrected the nasal septal deviation followed of the inferior turbinate approach, with mucous incision in the antero-inferior portion and subperiosteal dissection of the middle and lateral mucosas, with exposure of the turbinal bone. In the IT middle-posterior portion, corresponding to the bubble-like portion, the turbinal bone inferior portion was dried. Then maxillary antrostomy was made by the inferior turbinate, now with the disposition of two osseous laminas allowing for a lateral and medial laminas approaching the bubble-like portion was undone. The lateral and medial mucosas were placed so as to cover the bone (Picture 2).
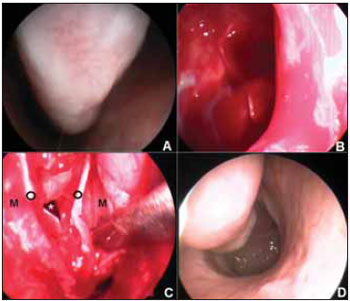
Picture 2. A- Preoperative. B- Intraoperative - Turbinal meatotomy. C- Intraoperative - Dissection and laminas mucosa(m), osseous(o) and maxillary (*). D- Postoperative aspect.
The postoperative follow-up had no particularities and in the third week of follow-up, with an improvement of the nasal breathing, a new nasal endoscopy allowed the viewing of the normal size inferior turbinate image without trace of communication of the inferior meatus with the maxillary sinus.
DISCUSSIONThe evaluation of the patient with complaint of nasal obstruction must include routine physical exam and nasal endoscopy to identify functional and anatomic alterations that are base for the clinical and/or surgical treatment. In patients with suspicion of rhinosinusitis it's fundamental to proceed tomographic study for surgical planning and follow-up.
Until two thirds of the upper airways resistance is generated by the inferior turbinate head in the nasal valve region (1), which makes this region the one of lowest transverse diameter of the upper airways. The mixed hypertrophy of the inferior turbinates (osseous and mucous) is generally noted in patients with nasal obstruction and many techniques are described and applied for this alteration treatment.
The surgical management is indicated when medication treatment with anti-histaminic and topical corticosteroids have failed and the patient has an obstruction cause surgically treatable, which can be made by means of cold lamina, electrocauterium, laser, microincision instrument etc. (2).
Bubble-like inferior turbinates (pneumatized) are rarely found and then taken for granted by many otorhinolaryngologists.
This bilateral finding is even rarer and must be treated (5) when it causes obstructive symptoms, as in the case presented. However, the large connection of the turbinate pneumatized region to the maxillary sinus has proven to be a challenge, in terms of approaching the turbinate without provoking a connection of the inferior meatus and the sinus.
Although it's an uncommon finding, the pneumatized inferior turbinate must be part of the nasal obstruction differential diagnosis, so as to enable an adequate surgical program and prevent surprises during common operations, such as the inferior turbinectomy.
BIBLIOGRAPHICAL REFERENCES1. Egeli E, Demirci L, Yazýcý B, Harputluoglu U. Evaluation of the inferior turbinate in patients with deviated nasal septum by using computed tomography. Laryngoscope. 2004, 114:113-17.
2. Berger G, Balum-Azim M, Ophir D. The Normal Inferior Turbinate: Histomorphometric Analysis and Clinical Implications. Laryngoscope. 2003, 113:1192-98.
3. Akoglu E, Karazincir S, Balci A, Okuyucu S, Sumbas H, Dagli AS. Evaluation of the turbinate hypertrophy by computed tomography in patients with deviated nasal septum. Otolaryngol Head Neck Surg. 2007, 136(3):380-4.
4. Braun H, Stammberger H. Pneumatization of turbinates. Laryngoscope. 2003, 113:668-72.
5. Kiroglu AF, Cankaya H, Yuca K, Kara T, Kiris M. Isolated turbinitis and pneumatization of the concha inferior in a child. Am J Otolaryngol. 2007, 28(1):67-8.
1. Resident Doctor R3 of the Armed Forces Hospital.
2. Resident Doctor R2 of Otorhinolaryngology.
3. Resident Doctor R3 of Otorhinolaryngology.
4. Otorhinolaryngologist. Head of the Otorhinolaryngological Clinic of the Armed Forces Hospital.
Institution: Hospital das Forças Armadas. Brasília / DF - Brasil.
Mail address:
Caio Athayde Neves
Avenida Contorno do Bosque S/N - HFA (Otorrinolaringologia)
Cruzeiro Novo - Brasília - DF - Brasil - Zip Code: 70658-900
Article received on July 20 2008.
Approved on March 5 2009.

