INTRODUCTION In the industrial environment we will find a preoccupying factor if we think of the serious implications to the physical and psychic health of workers, that occur with the indiscriminate and non-planned increase of industrialization. The state of São Paulo stands out as a pole of small and medium-sized enterprises. It is common to find small-sized companies installed with a reduced investment and a low number of employees, generally with low level of qualification. This set of characteristics is followed by lack of information of workers and entrepreneurs concerning the occupational risks of the adopted activity field.
We find several agents that under certain conditions may commit the quality of the work environment and consequently the worker's health and quality of life. Out of the main occupational risks in cabinetworks, we may mention noise, dust, vibration and chemicals, such as glue.
Studies on work environments report that in industries we may identify up to nine harmful agents simultaneously. Although they are complex, the studies about the combined effects at work are an important challenge in the area of worker's health (1). However, an increase of publications on the combined effects was verified, and appointed a growing interest in a less restrictive approach for explanation of associative connections, specially about the chemicals and noise exposure (2). In addition to noise in the work environments, other agents combined to it represent a potential risk to hearing, even under relatively low noise exposure conditions. Such agents comprise the organic solvents, chemical asphyxiants, metals and ototoxic drugs (3).
Decree 3048 of the Social Security of May 06 1999 acknowledges some chemicals as ototoxic agents and indicates that this type of exposure must be taken into account when we examine the causal connection between an auditory loss and the work environment conditions (4). In a study with two groups of individuals exposed to the same intensity of industrial noise, in which one of these groups is exposed to cadmium and not the other, verified a hearing loss concentrated mainly in the frequencies of 4000 and 6000 Hz, more stressed in the group exposed to noise and cadmium, and then concluded the probable ototoxic action of the cadmium metal when associated to noise exposure (5). Another comparative study, carried out by means of audiometric exams, compared two groups of 155 metallurgical workers(18 to 50 years) exposed to noise (GI) and to noise and chemicals (GII) for a period that ranged from 3 to 20 years. The results confirmed a significant difference in the proportion of occupational hearing loss at the OD between groups I (3.6%) and group II (15.5%); a significantly higher occupational hearing loss proportion in GII (18.3%) compared to GI (6%). They concluded that GII presented a proportionally higher prevalence of hearing loss when compared to GI, even having been exposed to the harmful agents for a shorter mean time (6).
Environmental stressors such as noise, heat, vibrations, pressures, radiations and chemicals like tobacco, dust, gases, steams are some of the agents found in several work places (7). In addition to these, there are also organizational stressors, that are those related to the work organization, like shifts, rhythm and ergonomy, that is, the relationship of the workers with their tasks. When combined, they may have a number of effects on the workers' health and welfare and thus increase the risk of work accidents.
The Noise-Induced Hearing Loss (NIHL) has been object of studies in the collective health field due to the auditory alterations that affect communication and the workers' quality of life. Noise is considered to be the most frequent physical agent in the work environment, and is characterized as a factor of the highest prevalence in the occupational diseases origin (8). In Brazil, the NIHL is amongst the workers' main health problems (7) and is ranked in the second place amongst the most frequent diseases of the auditory system (10).
NIHL was described as a cumulative and insidious pathology that progresses along the years of noise exposure associated to the work environment. Its initial signs show the affection of the auditory thresholds in one or more frequencies between the range of 3000 to 6000 Hz (11). It is also defined as a gradual reduction of the auditory accuracy resulting from continuous exposure to high levels of sound pressure, which provokes lesion in the internal and external hair cells of the Corti's organ. Characterized by a neurosensorial, irreversible, almost always bilateral and symmetric loss, it does not exceed 40 dB (NA) in the grave frequencies and 75 dB (NA) in the acute frequencies; it primarily manifests in 6000 Hz, 4000 Hz and/or 3000 Hz and expands to frequencies of 8000 Hz, 2000 Hz, 1000Hz, 500 Hz and 250 Hz. It has an irreversible nature and progressive evolution, susceptible to prevention (12).
NIHL may interfere with the worker's quality of life and produce hearing handicaps and disabilities such as the reduction of the speech perception in noisy environments, of television, radio, movies, theater, alert sound signals, music and environmental sounds. Handicaps that represent non-auditory consequences, influenced by psychosocial and environmental factors such as stress, anxiety, isolation and poor self-imaging, which commit the individuals' relationships in the family, at work and in the society and damage the development of their activities in the day by day life (13).
Out of the factors that influence the risk of installation of NIHL, the physical characteristics of the noise stand out (type, spectrum and level of sound pressure), the time of exposure and the individual susceptibility (14).
The diagnosis of NIHL depends on the typical representation in the audiograms and the evidence of the existence of noise exposure in the work environment, always taking into account the intensity and the nature of such agent, as well as the mode of exposure (15).
By analyzing the literature researched, we may observe that most studies carried out with workers confirmed that the noise may cause auditory symptoms such as hearing loss, tinnitus and difficulty to understand the speech; extra-auditory symptoms, such as vestibular alterations, in the excretion of cortisol, sleep alterations and communication disorder, as well as behavioral symptoms, excitability and stress (5.13, 14, 16, 17, 18 e 19).
It is estimated that the risk of undergoing work accident is twice higher among workers exposed to noise. The occupational exposure to noise not only deteriorates the auditory health of the worker, but also corresponds to a risk factor for work accident (17).
Vibration is also an occupational risk agent associated to the noise (18). The exposure action combined with the risks, noise and vibration may cause a synergic effect to the workers' health; the damages in the inner ear may cause the worsening of hearing, mainly in medium and low frequencies (20).
A systematic increase of stress and other deleterious effects in workers exposed to this combination is higher compared to workers exposed to one or other separately (721). This study also concluded that the complaints included by workers exposed to the entire body vibration were: headache, dizziness, column problems, sleep problems, hypertension, anxiety, nervousness, inattention, tingling sensation and whitening of the fingers, tinnitus and vision problems. As for the altered audiograms, the higher group was exposed to a vibration transmitted by means of hands-arms.
In the national literature, several studies with workers exposed to occupational noise appoint to a prevalence of hearing loss induced by high sound pressure levels - NIHL (22). In a study carried out with 187 metallurgical workers, the author quantified the occurrence of auditory alterations suggestive of NIHL and its main symptoms. The results were 21% suggesting NIHL, 72% suggesting other diseases. The most remarkable symptoms were difficulty of speech understanding (12%), hypacusis (7%), tinnitus (13%); sensation of auricular plenitude (4%); otorrhea (6%) and dizziness (12%) (14).
The prevalence of hearing losses was studied in workers of the marble production sector. 152 workers were evaluated with a mean age of 30 years and 8.3 years of occupational exposure to noise. The results revealed that 48% of the sample presented auditory damage, with a higher level of hearing loss in the frequency of 6000 Hz. Out of the altered audiometry results, 50% presented noise-induced hearing loss (NIHL) and 41% with beginning of NIHL. Amongst the workers with NIHL, 57.1% had bilateral alteration, 17.1% in the right ear and 25.7% in the left ear. Out of those with beginning of NIHL, 13.9% were bilateral, 19.4% in the right ear and 66.7% in the left ear (12).
The audiologic profile of a group of soldiers was studied and the authors concluded that out of the 97% of the thresholds included in the study, 38.1% presented with a NIHL-suggestive otologic picture. The complaints of 25.8% of the individuals were of hearing loss and from those who had no complaints, 30.5% had characteristic audiometric alterations. The hearing loss found was the more intense the older the patient and the longer the time of work. Their main complaints were: irritation with intense sounds (54.6%) and temporary hearing loss (40.2%), 13.4% complained of tinnitus. It was also concluded that 64.59% of the soldiers examined did not use suitable protection in the shooting exercises (18).
The noise as a stress factor in the life of workers in the field of cabinetmaking and locksmith workshop was researched in 21 workers aged between 31 and 67 years, by means of audiometry and questionnaire on stress. The results confirmed 48% of the participants with auditory alterations and there was no correlation between the hearing loss and stress (23).
By means of a transversal study, the clinical and occupational data was analyzed from 182 workers in a metallurgic company. The results confirmed that 15.9% of the NIHL-suggestive cases, according to the Costa's classification in 1998, and no significant association was identified between these cases and the variables of age and regular use of IPE (15).
By means of a cross study with 184 workers of the textile industry, the authors researched on the prevalence of NIHL. The results indicated 28.3% of PAIR, with prevalence of level I hearing losses, according to Merluzzi's classification. The most frequent symptoms were difficult understanding of speech (25%), tinnitus (9.6%), auricular plenitude (5.8%), dizziness (3.8%) and otalgia (3.8%). The authors concluded there was an increase of cases of NIHL with age and time of exposure (24).
Aiming to verify the prevalence of NIHL in the industrial district, researchers (25) investigated the hearing loss prevention program (HLPP) of 89 companies of different segments of economic activity. They analyzed the last audiometry of 5372 workers. It was confirmed that out of 1019 workers with hearing loss, which correspond to 19% of such alterations, 90.6% are of sensorioneural type.
In another national study, aiming to analyze the noise control programs in four metallurgic companies, the authors analyzed 741 workers, 41% had auditory alterations (mean age of 42.3 years; mean time of service of 16.7 years). In workers with more than one audiometry, 104 presented with auditory threshold displacement. Out of whom, 38 (36.5%) NIHL bearers had their auditory thresholds aggravated. 69.5% of the workers were exposed to the noise higher than 84 dB(A). The study concluded that the Hearing Preservation Programs have not been managed suitably; the noise exposure is still excessive, and the risk of development of NIHL remains (17).
The prevalence of hearing loss in aircrafts maintenance workers was researched in 74 workers, including 11 pilots, 35 mechanics and 28 of the management area, aged from 31 to 50 years old. Its results appointed a high prevalence of DA, reaching 32.4%, higher among the mechanics, followed by support workers and lower among the pilots (26).
The reference and final auditory thresholds variation for each frequency was analyzed by means of a retrospective study from a database of 4837 workers who had at least 2 audiometry exams. The authors confirmed a higher alteration of the auditory thresholds in the right ear, and the older workers and those with a longer period of service were mostly affected (27).
Considering the high number of health complaints and the possibility of auditory alterations resulting from occupational noise exposure, the need for audiologic evaluation is evident for the early diagnosis of NIHL and preventive and collective action, aiming to preserve the hearing and the workers' health. Therefore, the objective of this study was to research the auditory health of employees in a funeral urns factory, exposed to several chemicals and physical agents, such as the noise, electric saw vibration, glue and dust.
METHOD It is a study with transversal design, with the participation of 90 workers of a funeral urns company of the countryside of the state of São Paulo. The study was approved by the Ethics Committee in Research, according to process no. 159/2008 and all participants signed the Free and Clarified Authorization Term.
90 workers of a funeral urns factory, aged between 16 and 52 years, took part in this study, exposed to sound pressure levels equal or higher than 85 dBNPS, vibration and/or chemicals in the work environment. The criteria established for inclusion of the participants in this sample were the minimum period of 1 year in this factory. As exclusion criteria, we determined the presence of neurological, psychiatric problems, use of ototoxic medication or hearing loss with determined etiology. The criteria used for inclusion or exclusion were obtained by means of the specific interview.
The CAE visual inspection was carried out with an otoscope of Missouri trademark, model TK007; specific interview and Threshold Tonal Audiometry were performed by means of audiometer of the ACÚSTICA ORLANDI trademark, model LO-250/TIPO3, with auricular plugs TDH-39, calibrated according to the audiometer gauging norms according to INMETRO. The exams were carried out in acoustic cabin of Virbrasom trademark, with 14 hours of auditory resting, by following the recommendation of administrative rule no. 19.
The audiometry results were classified in 3 groups, Group I, audiogram suggesting normal hearing; Group II, audiogram suggesting NIHL, and Group III, audiogram results with other classifications (28).
Statistical method The values observed in the variables studied were filed in the Microsoft Excel program. We used descriptive statistics by means of averages, minimum and maximum values. To analyze the difference between the averages, we used the paired t-test. We used the Spearman's rank correlation coefficient to verify the correlation between the occupational noise exposure time variables and the auditory thresholds. In all statistical tests we adopted the level of significance of 5% (p < 0.05).
RESULTS With the statistical analysis it was possible to draw the audiological profile of the population studied. We will primarily describe the data obtained as for the characteristics of the population studied. Out of the 90 participants, the minimum age was of 16 years, the maximum age was of 52 years. Out of whom, 17 were between 16 and 17 years old and had the function of young apprentice. The age range was divided in groups, 88.66% of the participants were from 16 to 35 years old, 8.88% between 35 to 45 years old and 4.44% from 46 to 52 years old. As for sex, 78 were male (86.6%) and 12 were female (13.3%). To comprehend the population studied, the service time ranged from 1 to 10 years of work, and the function time ranged from 3 months to 10 years.. As for the occupational function, we opted to analyze all the company's employees, so that the group was composed by assembler, assistant, cutter, sander, polisher, carpenter and cabinet maker.
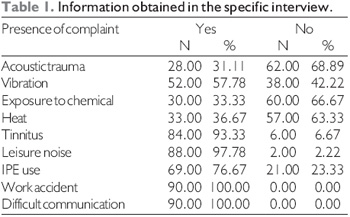
No participant was prevented from performing audiometry in the CAE visual inspection (Table 1).
Graphic 1 presents the auditory thresholds average of all frequencies studied, as well as the tritonal average of the medium frequencies (500Hz, 1kHz and 2kHz) and high frequencies (3kHz, 4kHz and 6kHz) in both ears by means of the paired t-test, no frequency studied presented statistically significant result.
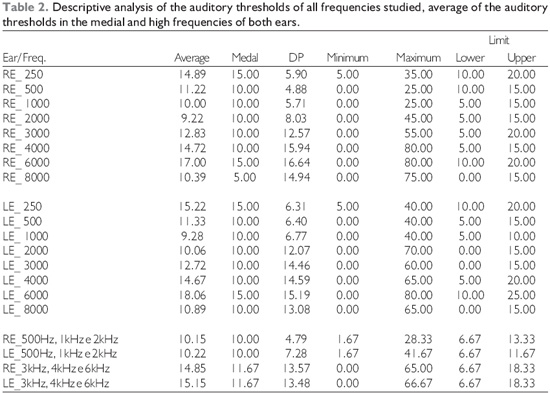
Table 2 describes the average of the auditory thresholds of all frequencies studied, as well the tritonal average of the medium frequencies (500Hz, 1kHz and 2kHz ) and high frequencies (3kHz, 4kHz and 6kHz) of both ears, in addition to the medial, standard deviation, maximum, minimum, upper and lower limits.
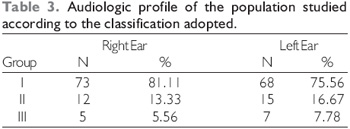
Table 3 describes the audiological profile of the population studied according to the Classification adopted (28), where Group I has suggestive audiogram results of normal hearing; Group II, audiogram results suggesting NIHL, and Group III, audiograms with other classifications.
To verify whether the age of the individuals studied influenced the auditory thresholds of both ears, we carried out the Pearson's Rank Correlation CoefficientTest(p<0.05), which indicated that the thresholds in the frequencies of 2, 3, 4, 6 and 8kHz in the right and left ears and also the frequency of 500 Hz in the left ear were statistically significant.
With the results of the Tukey's Test to compare the age range, we may confirm that in the frequencies of 2kHz, 3kHz, 4kHz, 6kHz and 8kHz of the right ear; 2kHz, 3kHz, 4kHz, 6kHz and 8kHz of the left ear and the average of the bilaterally medial and high frequencies had significant differences between the age range until 35 and >45 years, that is, the group of age range until 35 years presented a better auditory threshold than the group aged over 45 years. In the frequencies of 250 Hz, 2kHz, 4kHz, 6kHz and 8kHz of the right ear; 2kHz and 6kHz of the left ear and the average of the medial and high frequencies of the right ear presented statistically significant differences when compared to the group of age range between 36 to 45 years and over 45 years old, that is, the group aged between 36 to 45 years old presented statistically better auditory thresholds compared to those of the group with age range >45 year. In the comparison between the group aged until 35 years and the group aged from 36 to 45 years, the first presented statistically better thresholds in the frequencies of 1 kHz and 6kHz of the left ear.
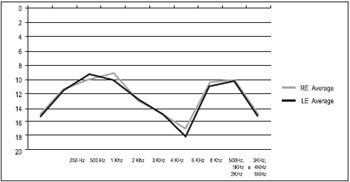
Graphic 1. Describes the comparison between the auditory thresholds averages of the right and left ears carried out of all frequencies studied and the comparison of the averages of the auditory thresholds of the medial frequencies (500 Hz, 1kHz and 2kHz) and high frequencies (3kHz, 4kHz and 6kHz) of a basis in kHz.
Amongst the agents that may result in occupational risk, the noise certainly appears as the most frequent; however, there are other agents that cause risk, such as ototoxic chemicals or vibration, which may produce occupational hearing losses in the absence of noise or potentialize the effects of auditory loss. Based on scientific researches, we may state that the simultaneous exposure to noise and ototoxic chemicals produces a synergic effect, and the exposure effect of combined exposure is higher than the simple addition of the effects of each agent separately (3). This study allowed us to analyze the auditory health in workers of funeral urns, the results confirmed, in the tritonal average, the auditory decrease in the higher frequencies, as described in table II, that is, for the tritonal average (500, 1000 and 2000Hz) of the RE it was of 10.15dB, of the LE it was of 10.22dB, the tritonal average of high frequencies (3000, 4000 and 6000Hz) was of 14.85 dB for RE and 15.15 for LE, and these results confirmed the findings of prior studies. (5,11,12,22). As for the laterality, the fact there was a higher commitment of the RE, as also observed in Table 2, both for averages of 500, 1000 and 2000 Hz, and for 2000, 4000 and 6000 Hz it is controversial and needs to be researched in the future because some studies reveal that the LE would be more susceptible to noise lesion (12) or a higher commitment in the RE (6-27). It is a matter that needs to be discussed, since there are different citations in several studies because there are factors that interfere with the laterality, including the individual susceptibility (29).
The literature points out a large occurrence of the incision in frequencies of 4000Hz or 6000Hz (2,10,12,14,15); also in Table 2, we may observe the prevalence of the incision in the frequency of 6000 Hz, results that are opposed to other studies (12), while other studies report the incision in the frequency of 4000Hz (14, 19).
In Table 1 we observe the data obtained in anamnesis, as for the IPE, 76.67% reported its the, once it may be ascribed for the adoption of protection measures adopted by the industry not much spread or a lack of knowledge of the forms of prevention of hearing loss, with focus on collective protection measures and the use of IPE. When industrial workers are exposed to noise higher than 85dBNPS, we know they may develop hearing losses and the use of IPE is determined (9, 10,14,19,22,28), but it is still not clear whether such norms are applicable for leisure noise, and there is a variety of opinions as for the implementation of measures to prevent hearing loss for leisure noise. In this study, a concerning information is observed in Table 1 as for the exposure to leisure noise, which is mentioned in 97.78% of the interviewees.
The prevalence of complaints concerning the presence of tinnitus is described in the literature as a common complaint of workers who work in noisy environments, in previous studies, the complaint of tinnitus ranged from 2.76% (19) to 68.7% (13). In this study the prevalence of tinnitus was of 93.33%. No other prior work has presented such a high prevalence.
A concerning data, once the occupational hearing loss is susceptible to prevention, was the prevalence of auditory alterations obtained in this study, presents suggestive audiograms of NIHL according to the classification adopted, that is, 13.3% in the RE and 16.67% in the LE, similar results were mentioned in other studies (5, 14, 19), in other works the prevalence was higher than that found in this work (12, 17, 18), which may be justified by the different occupational risk other than noise to which this population was exposed. These results are relevant for the periodical follow up aiming to avoid the hearing loss progression and point out the need to research aspects regarding vibration and chemicals, since there was no comparison of groups exposed only to noise or vibration and chemicals. We must also take into account the psychosocial effects, difficult to be measured.
In this study, the age and time of service were associated to the alterations on the auditory thresholds, we verified an increase in the auditory thresholds as an increase of age and time of exposure occurred, and these results agree with prior studies (18, 19, 22, 27), the average time of service of the workers ranged from 3 months to 10 years of work as well as the age ranged from 16 to 52 years, the audiometric findings of these workers may indicate that the working time in the company does not necessarily confirms the time of exposure to noise.
At last, considering that the occupational hearing loss can be prevented, there is the need for a stronger scientific investment to enable the prevention strategies. An educational work may modify the behavior in this population of young workers, as well as the entrepreneurs. Both, workers and company, are responsible for the compliance with the law in force. Therefore, the workers would benefit with a better quality of life and the entrepreneurs would be playing their role with responsibility.
CONCLUSION This study enable the confirmation of:
altered audiometry results in the right ear in 13.33% and 16.67% in the left ear;
the age range influenced the auditory thresholds.
BIBLIOGRAPHIC REFERENCES 1. Lacaz, FAC. Saúde dos trabalhadores: cenários e desafios. Cad. Saúde Públ. 1997, 13(2):7-19.
2. Morata TC, Lemasters GK. Considerações epidemiológicas para o estudo de perdas auditivas ocupacionais. In: Nudelmann, AA (org). PAIR. Rio de Janeiro; Ed. Revinter; 2001. v.2, p.1-16.
3. Lacerda A, Leroux T, Morata TC. Efeitos ototóxicos da exposição ao monoxico de carbono: uma revisão. Pró-Fono. Revista de Atualização Científica. 2005, 17(3):403-12.
4. Ministério da Previdência e Assistência Social. Decreto no. 3048, de 06/05/1999. Aprova o regulamento da previdência social e dá outras providências. Brasília. Ministério da Previdência e Assistência Social. 1999 [DOU de 12/05/ 1999].
5. Abreu MT, Suzuki FA. Avaliação audiométrica de trabalhadores ocupacionalmente expostos a ruído e cádmio. Rev Bras Otorrinolaringol. 2002, 68(4):488-94.
6. Botelho CT, Paz APML, Gonçalves AM, Frota S. Estudo comparativo de exames audiométricos de metalúrgicos expostos a ruído e ruído associado a produtos químicos. Rev Bras Otorrinolaringol. 2009, 75(1):51-7.
7. Fernandes M, Morata TC. Estudo dos efeitos auditivos e extra-auditivos da exposição ocupacional a ruído e vibração. Rev Bras Otorrinolaringol. 2002, 68(5):705-13.
8. Padovani C, Nova CV, Queirós F, Silva LPA. Percepção das condiçöes auditivas pelos servidores públicos da Universidade do Estado da Bahia: consideraçöes sobre o projeto saúde auditiva. Rev. Baiana Saúde Pública. 2004, 28(2):203-11.
9. Gabas G. Escute bem e proteja-se. Rev Proteção. 2007, 181:54-61.
10. Atti JL, Correa AG, Stefani F, Vaccaro S. Perda Auditiva Induzida por Ruído. Rev. Cient. AMECS. 2000, 9(2):40-4.
11. Gatto C, Lerman RA, Teixeira TM, Magni C, Morata TC. A análise da conduta de médicos diante de trabalhadores com perda auditiva. Rev Distúrbios da Comunicação. 2005, 17(1):101-14.
12. Hanger MRHC, Barbosa-Branco, A. Efeitos auditivos decorrentes da exposição ocupacional ao ruído em trabalhadores de marmorarias no Distrito Federal. Revista Assoc. Méd. Brasileira. 2004, 50(4):396-9.
13. Guida HL. Efeitos psicossociais da perda auditiva induzida por ruido em ex-funcionários da industria. Acta ORL/Técnicas em otorrinolaringologia. 2006, 25(1):78-83.
14. Araújo SA. Perda auditiva induzida pelo ruído em trabalhadores de metalúrgica. Rev. Bras. Otorrinolaringol. 2002, 68(1):47-52.
15. Guerra MR, Lourenço PMC, Bustamante-Teixeira MT, Alves MJM. Prevalência de perda auditiva induzida por ruído em empresa metalúrgica. Rev Saúde Pública. 2005, 30(2):238-44.
16. Dias A, Cordeiro R, Corrente JE, Gonçalves CGO. Associação entre perda auditiva induzida pelo ruído e zumbidos. Cad. Saúde Pública. 2006, 22(1):63-8.
17. Gonçalves, CGO, Iguti MA. Análise de programas de preservação da audição em quatro indústrias metalúrgicas de Piracicaba, São Paulo, Brasil. Cad. Saúde Pública. 2006, 22(3):609-18.
18. Silva AP e col. Avaliação do perfil auditivo de militares de um quartel do Exército Brasileiro. Rev Bras Otorrinolaringol. 2004, 70(3):344-50.
19. Lopes AC, Nelli MP, Lauris JRP, Amorim RB, Melo ADP. Condições de saúde auditiva no trabalho: investigação dos efeitos auditivos em trabalhadores expostos ao ruído ocupacional. [periódico online]. Arq Int Otorrinolaringol. 2009, 13(1):49-54.
20. Bochina M, Morgenroth K, Dziewiszek W, Kassner J. Experimental vibratory damage of the inner ear. Eur Arch otorhinolaryngol. 2005, 262(4):307-13.
21. Izumi R, Mitre EI, Duarte MLM. Efeitos das vibrações de corpo inteiro na audição. Rev CEFAC. 2006, 8(3):386-92.
22. Porto MAA, Gavya DLC, Lauris JRP, Lopes AC. Avaliação da audição em frequências ultra-altas em indivíduos expostos ao ruído ocupacional. Pró-Fono. 2004, 16(3):237-50.
23. Kasper KCF, Gomes MVG, Zaher VL. O ruído como fator estressante na vida de trabalhadores dos setores de serralheria e marcenaria. Arq. Int. Otorrinolaringol. 2005, 9(1).
24. Caldart AU, Adriano CF, Terruel I, Martins RF, Caldart AU, Mocellin M. Prevalência da perda auditiva induzida pelo ruído em trabalhadores de industria têxtil. Arq Int Otorrinolaringol. 2006; 10(3):192-6.
25. Teles RM, Medeiros MPH. Perfil audiométrico de trabalhadores do distrito industrial de Maracanaú - CE. Rev Soc Bras Fonoaudiol. 2007, 12(3):233-9.
26.Ribeiro AMD, Câmara VM. Perda auditiva neurossensorial por exposição continuada a níveis elevados de pressão sonora em trabalhadores de manutenção de aeronaves de asas rotativas. Cad Saúde Publ. 2006, 22(6):1217-24.
27. Santos JD, Ferreira MIDC. Variação dos limiares audiométricos em trabalhadores sumetidos a ruído ocupacional. Arq Int Otorrinolaringol. 2008, 12(2):201-209.
28. Fiorini AC. Conservação auditiva: estudo sobre o monitoramento audiométrico em trabalhadores de uma indústria metalúrgica[dissertação mestrado em Distúrbios da Comunicação]. Pontifica Universidade Católica de São Paulo. São Paulo; 1994.
29. Silva GLL, Gomes MVSG, Zaher VL. Perfil audiológico de motoristas de ambulância de dois hospitais na cidade de São Paulo-Brasil. [periódico online]. Arq Int Otorrinolaringol. 2006, 10(2):132-40.
30. Lopes AC, Santos CC, Alvarenga KF, Feniman MR, Caldana ML, Oliveira AN, Jorge TM, Bastos JRM. Alterações auditivas em trabalhadores de industrias madeireiras do interior de Rondônia. Rev Bras. Saúde Ocupacional. 2009, 34(119):88
1. Doctoral Degree. Doctor Professor.
2. Specialist in Audiology. Clinical Phonoaudiologist.
3. Master's Degree in Phonoaudiolgist. Fapesp Grant Holder.
4. In Graduation Course of Phonoaudiology.
5. Doctoral Degree. Associate Professor of the Odontopediatrics, Orthodontics and Collective Health of FOB-USP.
6. Phonoaudiologist. In course for Master's Degree in Phonoaudiology at FOB/USP.
Institution: Departamento de Fonoaudiologia - Faculdade de Odontologia de Bauru/USP. Bauru / SP - Brazil. Mail Address: Andréa Cintra Lopes - Alameda Dr. Octavio Pinheiro Brisolla, 9-75 - Vl. Universitária - Bauru / SP - Brazil - Zip-code: 17043-101 - Caixa Postal: 73 Telephone: (+55 14) 3235-8000 extension: 8557 - E-mail: aclopes@usp.br
Article received on June 24, 2009. Article accepted on August 16, 2009.