INTRODUCTION The noise is a physical agent original from the superposition of several aperiodic sound vibration movements, with different frequencies. It is present in a large part of the social and occupational activities, and provokes an unpleasant sensation to the listeners (1). It separately presents a danger to the health when the sound level is higher than 80 dB, depending on its duration and systematic exposure. Therefore, from such sound intensity, audiometry is periodically made in industries (2).
The noise induced hearing loss (NIHL) has the following characteristics: it is always neurosensorial, as a result from the lesions that affect the cochlear hair cells; is irreversible and almost always of bilateral origin; it rarely reaches the deep degree of auditory loss. We also emphasized that, initially, NIHL affects the regions of frequencies of 6, 4 or 3 kHz, and with the loss progression it may reach regions of 8, 2, 1 kHz and 250 Hz. In addition to this, the individual may have tinnitus and discomfort to intense sounds and once ceased the exposure to noise, there is no noise progression. The individual time exposure and susceptibility are also factors that may influence in the appearing of the disease (3).
In a research carried out with workers of the industry in the metropolitan region of Salvador a prevalence of 35.7% of NIHL was observed, and there was a high prevalence of unilateral NIHL, 18% of the workers evaluated (4). Other research evaluated the hearing of 826 metallurgic workers and observed unilateral NIHL in 40% of the cases (5).
A study carried out to analyze the auditory and extra-auditory complaints in individuals exposed to noise showed that the most common hearing complaint was tinnitus and the extra-auditory complaint was arterial hypertension (6).
In the evaluation of patients exposed to noise, several methods may be used, such as threshold tonal audiometry (7) and high frequency audiometry, but the latter is not the most feasible and there is no consensus regarding interpretation criteria (8) and both present the factor of subjectivity in their results.
Another tests that present a large clinical potential are the otoacoustic emissions (OAE). It is a quick, objective and easy application exam. The cochlear alterations resulting from the exposure of high levels of sound pressure and chemicals may provoke early changes in their amplitude, that are original from the Corti's organ, by the external hair cells.
A study carried out recently with distortion product otoacoustic emissions (DPOAE) and workers exposed to pulsatile noise, concluded that a reduction occurred in the amplitude of reduction of responses in all frequencies researches (9).
Another study analyzed 338 volunteers before and after the exposure to noise. It showed that while the average of otoacoustic emissions amplitudes diminished significantly, the average of audiometric thresholds did not change, the authors concluded that the otoacoustic emissions may, therefore, be a causal variable for the noise induced auditory loss diagnosis (10).
In this same research line, other authors evaluated 74 workers, divided into exposed and not exposed to noise, the results suggest that occupational noise exposure may provoke alterations in the DPOAE's registers, even in individuals with tonal audiometry exam within acceptable limits, which indicates that this exam may be important as an early diagnosis method of the occupational noise induced hearing loss (11).
Today other harmful agents are being studied concomitantly to the noise, such as for instance the chemicals. The chemical act slowly, insidiously and by accumulating in the organism (12). The high frequency commitment seems to be one of the first signs detected as for the exposure effects relation combined with the noise in the workers' health (13).
Within this research line, studies have been carried out with professionals who control vectors by means of chemical, mechanical products or any other means of removal of agents harmful to the population. These workers are more exposed to insecticides of pyrethroid and organophosphorus type (14).
An important study verified that the distortion product otoacoustic emission amplitude was lower than in the group of individuals exposed to noise and to noise and lead at the same time, when compared to individuals without exposure to such agents and that the research of otoacoustic emissions may be altered in individuals exposed to noise and to noise and lead at the same time, even with auditory threshold in 25 dB, proposed as a normal standard for industries workers (15).
In another study, the authors did not confirm any statistically significant alterations between individuals exposed to both elements and individuals only exposed to noise; however, they concluded that the data suggests a neurotoxic and not cochlear effect of such product (16).
Some works suggest that exposure of both agents is actually harmful to health, since they have a synergic effect. However, these researches are scarce and present the need for a special attention to the subject because there is a large number of Brazilians exposed to this type of danger.
The objective of this work is to research the audiologic and DPOAE findings in workers exposed to occupational noise and plaguecides, with normal hearing and with hearing losses, and compare them with individuals without history of exposure to noises and plaguecides, in order to analyze the efficacy of the DPOAE test in the NIHL diagnosis.
METHOD This study was carried out in the Clinical Audiology Sector of the Center of Education and Health Studies (CEES), of the Philosophy and Sciences College of UNESP, Campus Marília - SP and was approved by the Ethics Committee in Research of the Institution (protocol no. 2606/2007).
The study was accomplished with 51 individuals (102 ears), divided into three groups. Group I was composed by 17 workers with a history of exposure to noise and plaguecides, all of whom with neurosensorial auditory loss, group II was formed by 17 workers with history of exposure to noise and plaguecides with audiometric thresholds within normality standards and group III was composed by 17 individuals without history of auditory complaint nor exposure to noise and plaguecides and was thus considered as the control group.
For individuals of groups I and II, all of the male sex, the general mean age was of 37.5 ± 3.48 years, ranging from 24 to 57 years and the exposure average time was of 12.5 years, ranging from 1 to 22 years. The individuals of group III, 6 men and 11 women were from 20 to 40 years old, with an average age of 35.2 ± 4,41 years.
The individuals of groups I and II were exposed to malation chemical. For the product's inhalation they used a pressurized costal spray that emits an equivalent level of noise of 98.5 dB (A) (14). The exposure time was of 3 to 4 hours per day. The employees were duly equipped with Individual Protection Equipment (IPE), and for our study it was important to stand out the use of suitable auricular protection. Some workers used ear protection of insertion/ splint type (CA 9275) theoretical attenuation level NRR of 21dB(A), other workers used ear protection of the shell type (CA 5322 with NRR of 23 dB(A).
Information regarding the following procedures were researched:
- audiologic anamnesis to survey the workers auditory health identification and history;
- imitanciometry, with the use of imitanciometer GSI 38 Grason - Stadler. In the acoustic immittance analysis of the individuals' middle ear, the tympanometry was considered (17). This procedure helped the evaluation of functional integrity of the tympano-ossicular set.
- threshold tonal audiometry, to evaluate the tonal thresholds (by air and bone ways) of the workers (18). The exam was made in an acoustic cabin, with the use of two-channels audiometer GS1 61 Grason - Stadler, with TDH-50 plugs.
- distortion product otoacoustic emissions to evaluate the cochlear functioning, more specifically the external hair cells. The equipment used was DPOAE-20 of Interacoustics connected to a computer. The test was carried out in acoustic cabin by means of a Dp-Gram that is obtained upon concomitant presentation of to pure tones f1 and f2. Such pure tones, called primary frequency, are expressed by the ratio of 1.22. In this study we used the response register equivalent to 2f1f2 and the intensity ratio L1 = 65 and L2 - 55 dBNPS. For analysis the frequencies of 1, 2, 4 and 6 kHz were considered. The ratio sign / noise was of 7 dB. The results analysis criteria were based on a relevant study about the clinical application of the DPOAEs in individuals with NIHL (19).
To test the significance between the groups a comparative analysis between the averages of the DPOAE test responses was made with the use of the Test ANOVA. Unique Factor, with significance level of 5% (p < 0.05) and tolerance level build up with 95% of statistical tolerance.
Whereas prior studies (20, 21) did not identify differences in the OAEs registers according to sex, the analyses were made irrespectively of the gender.
RESULTS The audiologic anamnesis results, concerning groups I and II, revealed that the main auditory symptoms and/or complaints presented by the workers were those of recruitment/discomfort to intense sounds (29.5%), tinnitus (26.5%) and arterial hypertension (12%). The individuals of group III did not present auditory complaints.
As for groups I and II, we consider that the time of exposure to noise and plaguecides ranged between 1 and 22 years (an average of 12.5 years), out of all, 26 individuals reported having always used individual protection equipment, 5 do not use ear protection and 3 use it asystematically.
In group I all workers presented with hearing loss of neurosensorial type, and they were 9 bilateral and 8 unilateral losses, summing up a total of 26 ears; in group II all workers presented audiometric thresholds within the normality standards (up to 25 dBNA), in addition to the normal ears, the unilateral cases of group I, totalizing 42 ears, and in group III all individuals presented audiometric thresholds within the normality standards, totalizing 34 ears.
In all cases studied type A (15) tympanometric curves were obtained, which revealed integrity of the tympano-ossicular system.
Graphic 1 presents the distribution of the 34 ears with exposure to noise and plaguecides (groups I and II); according to different degrees of affection, in seven audiometric frequencies, values within the normality, thresholds up to 25dB (NA) were considered and the hearing losses were characterized into values of 30 to 40 dB (NA) and 45 to 55 dB (NA).
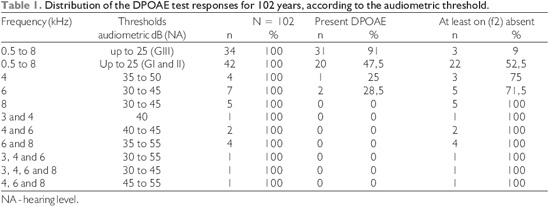
Then a clinical verification of the DPOAE test was carried out obtained according to the comparison with the tonal audiometry as presented in Table 1. This table confirmed the DPOAE responses were present in 91% of the cases, in group III (GIII), while in groups I and II (GI and GII), these were present in 47.5% of the cases.
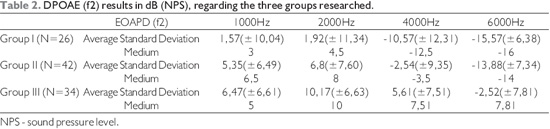
In a quantitative viewpoint (Tables 2 and 3), the DPOAE results allowed us to verify that there was a significant decrease in the responses amplitude, in the comparison between the groups.
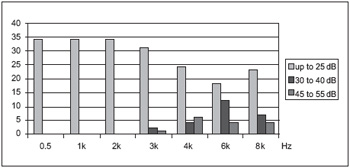
Graphic 1. Distribution of 34 ears according to the different audiometric thresholds (dBNA) in the frequencies between 0.5 to 8 kHz.
The audiometry results indicated the researched individuals did not present with hearing losses in the frequencies of 500 Hz, 1 and 2 kHz, and the losses occurred in the frequencies between 3 and 8 kHz. The data presented confirm the literature concerning noise induced hearing loss, which characterizes the audiogram with auditory loss in high frequencies, with descending neurosensorial curve, as well as the most frequent audiologic complaints were those of recruitment and tinnitus (3).
The results analysis revealed unilateral neurosensorial type hearing loss in 47% of the ears in group I. Unilateral NIHL was described by other authors (4, 5), who suggested to reconsider the statement that NIHL is almost always bilateral.
In addition to tinnitus, arterial hypertension is mentioned as an important extra-auditory finding (6), this symptom was also present in our results.
The fact we found compatible thresholds with hearing loss only at high frequencies may be due to two factors: the individuals are in process of unleashing of the NIHL; or do not present with aggravation of the hearing loss because the institution has a prevention program implemented for nine years. However, we must consider the commitment in high frequency, observed in the population with hearing loss, seems to be one of the first signs detected as for effects of the exposure to ototoxic agents, associated with noise, in the worker's health (13).
This study made evident that the exposure to occupational noise and plaguecide, whether in individuals with hearing loss or in individuals who did not present alterations in the tonal audiometry yet, was responsible for a decrease in the responses amplitude for the DPOAE test, when the results are compared with the control group, without exposure to noise and plaguecide. This relationship between noise exposure and decrease in the DPOAE's amplitude were also obtained by other authors (10, 11, 15).
CONCLUSION As far as the results obtained in this study, it was possible to observe an important contribution of the distortion product otoacoustic emission test for diagnosis of auditory alterations, since there was a decrease in the tests responses amplitude, even in individuals exposed to noise and plaguecides, with audiometric thresholds within the normality standards.
Therefore, we conclude the DPOAE test represents a useful tool not only for follow up but also for prevention of the NIHL.
BIBLIOGRAPHICAL REFERENCES 1. De Almeida SIC, Albernaz PLM, Zaia PA, Xavier OG, Karazawa EHI. História natural da perda auditiva ocupacional provocada por ruído. Rev Ass Med Brasil. 2000, 46:143-58.
2. Brasil. Ministério do Trabalho e Emprego. Portaria 3.214 de jul. 1978. Normas regulamentadoras de segurança e saúde no trabalho (NR-15): atividades e operações insalubres. Brasília; 1978.
3. Comitê Nacional de Ruído e Conservação Auditiva. Perda auditiva induzida pelo ruído relacionado ao trabalho. Acust Vibr. 1994, 13:123-25.
4. Miranda CR, Dias CR, Pena PGL, Nobre LCC, Aquino R. Perda auditiva induzida pelo ruído em trabalhadores industriais da região metropolitana de Salvador, Bahia. IESUS, 1998, 7:87-94.
5. Kwitko A, Pezzi RG. Crítica da norma regulamentadora no 7.1 Tabela de Fowler. 2. Perda auditiva bilateral. Revista Brasileira de Saúde Ocupacional, 1993, 21:93-99.
6. Blandino PC, Garcia AP. Estudos das Queixas Auditivas e Extra-auditivas em Trabalhadores do Serviço Social do Comércio. Acta ORL. 2006, 24:239-244.
7. Mulheran M, Degg C. Comparison of distortion product OAE generation betwen a patient growth requirent frequent gentamicin therapy and control subjects. Br J Audiol. 1997, 31:5-9.
8. Campbell KCM, Durrant J. Audiologic monitiring for ototoxicity. Otolaryngologic Clinics of North America (Ototoxicity). 1993, 26:903-10.
9. Konopka W, Olszewski J, Pietkiewicz P, Mielczarek M. Distortion product otoacoustic emissions before and after one year exposure to impulse noise. Otolarygol Pol. 2006, 60:243-7.
10. Lapsley MJA, Marshall L, Heller LM, Hughes LM. Low-level otoacoustic emissions may predict susceptibility to noise-induced hearing loss. J Acoust Soc Am. 2006, 120:280-96.
11. Marques FP, Costa AC. Exposição ao ruído ocupacional: alterações no exame de emissões otoacústicas. Rev Bras Otorrinonalaringol. 2006, 72:362-6.
12. Ribeiro HP, Lacaz FAC. De que adoecem e morrem os trabalhadores. Imprensa Oficial do Estado, São Paulo: DIESAT/IMESP; 1984.
13. Morioka I, Miyai N, Yamamoto H, Miyashita K. Evaluation of combined effect of organic solvents and noise by the upper limit of hearing. Industrial Health. 2000, 38:252-7.
14. Vilela RAG, Malagoli ME, Morrone LC. Trabalhadores da saúde sob risco: o uso de pulverizadores no controle de vetores. Revista Produção. 2005, 15:263-72.
15. Alvarenga KF, Jacob LCB, Martins CHF, Costa AO, Coube CZV, Marques JM. Emissões Otoacusticas - produdo de distorção em Indivíduos Expostos ao chumbo e ruído. Rev Bras Otorrinolaringol. 2003, 69:681-6.
16. Martins CHF, Vassoler TMF, Bergonse GFR, Alvarenga KF, Costa AO. Emissões otoacústicas e potencial evocado auditivo de tronco encefálico em trabalhadores expostos a ruído e ao chumbo. Acta ORL. 2007, 25:293-98.
17. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryng. 1970, 92:311-24.
18. Momensohn-Santos TM, Russo ICP. Prática da audiologia clínica. 5a ed. São Paulo: Cortez Editora; 2005.
19. Parrado Moran MES, Fiorini AC. Aplicações clínicas das emissões otoacústicas-produto de distorção em indivíduos com perda auditiva induzida por ruído ocupacional. Distúrbios da Comunicação. 2003, 14:237-61.
20. Hauser R, Probst R. The influence of systematic primary-tone level variation L2-L1 on the acoustic distortion product emission 2f1-f2 in normal human ears. J Acoust Soc Am. 1991, 89:280-6.
21. Coube CZV, Costa Filho OA. Emissões otoacústicas evocadas: produto de distorção em indivíduos com audição normal. Rev Bras Otorrinolaringol. 1998, 64:339-45.
1. Doctor (a). Professor Assistant Doctor.
2. Bachelor's Degree in Phonoaudiology. Phonoaudiologist.
Institution: Faculdade de Filosofia e Ciências - Departamento de Fonoaudiologia, UNESP - Campus de Marília - SP.
Mariília / SP - Brazil. Mail Address: Heraldo Lorena Guida - Avenida Hygino Muzzi Filho, 737 - Caixa Postal 181 - Marília / SP - Brazil - Zip code: 17525-900 - E-mail: hlguida@marilia.unesp.br Fund for Research of the Philosophy and Sciences College - UNESP, Campus of Marília.
Article received on June 15 2009. Approved on July 27 2009.