INTRODUCTION Teachers at all levels of education need for an effective functioning of the phonatory system for the exercise of their profession. The phonatory dysfunctions that develop or exacerbate in the course of their activity, manifested initially by signs and symptoms whose cause is attributed to professional voice use with or without other factors.
Due to the diversity of multiple causation and symptomatology in disorders of the voice we propose to designate the set of factors related to the loss of vocal health through the use of professional occupational dysphonia Syndrome (ODS).
Based on the classic concept of health, we can affirm that the health status of the voice represents the balance between form (phonatory system) and function (phonation), on the one hand, and the action of the forces that tend to disturb them, on the other side. This interrelationship is not passive, is an active response of the organism in order to adapt to the demands. Between adaptation and no adaptation to the professional use of voice there is a degree of euphony that extends to those who are in excellent condition, through different degrees of voice disorders ranging from that are reasonably well to those who are below normal until the who really are disabled.
According to LEAVELL & CLARK (1), the natural history of any disease process in humans has two periods in which there is the development and deployment of disease: pre-pathogenic and pathogenic.
In the pre-pathogenic for the performance of environmental risk factors in individual predisposition to the aggressors.
The period includes pathogenic phases: early pathogenesis, preceding the early discernible, followed by phases of the pathogenesis of advanced and convalescence.
Syndrome occupational dysphonia has its conceptual application in the early stages of disease pathogenesis vocal functional or organic.
Applying this concept to the SDO, in the pre-pathogenic three factors are interrelated, ie the individual such as gender, age and inadaptações phonic, environmental, noise, acoustics, microphones, work organization, ergonomics and stress activity and the pre-existing and hormonal disorders, inflammatory airway syndrome pharyngo-laryngeal reflux, self-medication, smoking, alcohol and caffeine intake.
The period begins in early pathogenic when the trigger action, and the host (the professional voice) does not adapt and respond to changes in functional or tissues in the phonatory system. These changes are not apparent by current diagnostic methods and criteria require clinical knowledge to consider the history of the disease since its inception, i.e. the pre-pathogenic and pathogenic early.
In these phases, there is the possibility of reversing the disease.
In the evolutionary process of the disorder begin to emerge that the symptoms are reversible when removing agent, which configures the pathogenesis discernible early and still not prevent the full development of the activity. When it evolves toward preventing partial activity starts advanced stage of the pathogenesis and treatment needs; we can add another milestone to set the advanced stage is the appearance of lesions in the larynx, which inserted into designated SDO laryngopathies Occupational (LO) (2).
In case of maintenance of changes (chronic) or their extreme consequences in convalescence can achieve the degree of dysphonia permanent disability.
Aiming to avoid the disability, we have to interfere with the harmful factors of detectable pre-pathogenic to pathogenic early discernible.
The techniques of primary prevention should then be applied to avoid expulsion from the professional activities and, reversing the disease's development. With preventive measures, we aim to maintain health by protecting specific vocal teacher and for establishing barriers against agents the environment.
In the pre-pathogenic and pathogenesis during the early difficult to identify the professional voice that will potentially move into the next phase through conventional diagnostic means, because everyone is focused on the presence of organic injury or functional installed. Pathogenesis of advanced-stage forward, the disability professional, professionals themselves identifies the need of diagnosis and care. Targeting the prevention of disability is essential to find those who are in early phase of pathogenesis discernible, as in the pre-patogêncio. This group, by having conditions to keep in activity, there appears spontaneously, but can be identified by the search for symptoms and removal of working conditions. In the advanced stage of pathogenesis will require professional care, secondary prevention with targeted and customized technical and essentially habilitatórias, there is usually temporary removal of their activities, but with full possibility of return. In convalescence act with tertiary prevention with emphasis on rehabilitation with the possibility of return doubtful.
Considering these aspects conducted by the Program for Prevention of Occupational Dysphonia University Teachers in the Northern Zone of São Paulo, a study aimed at determining the prevalence of occupational dysphonia Syndrome and checking the progress of this index after the introduction of prevention techniques primary.
METHOD We conducted a cross-sectional epidemiological study on the voluntary participation of teachers from a Higher Education Institution in the northern region of Sao Paulo. This study was performed at two different times: 2001 (phase 1) and 2004 (phase 2). Was approved by the Medical Ethics Committee and had the signature on the Informed Consent Term for teachers and responsible institution. It was conducted by medical staff accompanied by representatives of the union workers.
To meet the objective of determining the prevalence of discernible stage of pathogenesis of SDO, we use the self-assessment questionnaire prepared by the Tripartite Commission (3) according to Decree 253 which was published in the Official Gazette on July 31, 2002. This pulled the questionnaire data on symptoms that can be found in dysphonia as pain or irritation of the throat (S1), foreign body sensation (S2), need for throat clearing (S3), neck pain (S4) and hoarseness (S5) divided into constant, constant fluctuations and intermittent.
The symptoms were comparatively analyzed individually and in combination (when two or more present), this characterizes the SDO.
Questionnaires were given to teachers who were in the staff room during the periods that preceded the classes in the early school years 2001 and 2004, with voluntary participation and without the personal identification responses. In the period 2001 to 2004 were presented to the institution and teachers in general preventive measures including: stimulating the hydration, protection against inhalation of irritant substances such as tobacco mucosa and dust contraindication to self-medication and caffeine consumption , correction of postural deviations, the concepts of misuse and abuse of the voice and guidance in a vocal rest.
Were analyzed by percentage prevalence for symptoms and isolated on the associated symptoms, ie, two or more, to characterize the SDO.
We obtained data on age and gender in order to establish the equivalence of the constitution of the groups in phases 1 and 2.
Statistical analysis was performed to verify the association between dependent variables with independent variables (phase 1 and phase 2) by applying non-parametric tests of association Chi-square or Fisher exact test. Stood the significance level of 5% (p <0.05). The database was created in Excel and the analysis used the software SAS / SAT version 9.12.
RESULTS The average age was 40.86 years with standard deviation of 8.9 years, minimum of 29 years and maximum 86 years in phase 1, with participation of 101 teachers.
In phase 2, the mean age was 38.23 years with standard deviation of 8:32 years, minimum of 34 years and a maximum of 64 years, with participation of 148 teachers.
In Graphics 1 and 2 are presented as percentage prevalence rates for symptoms and isolated on the associated symptoms (SDO).
In Graphic 3 we have three types of symptom hoarseness.
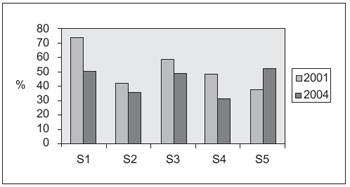
Graphic 1. Evolution of the percentage prevalence of symptoms of Syndrome occupational dysphonia phase 1 to phase 2. - S1 = pain or irritation p = 0.001 S2 = foreign body sensation, p = 0.2 = S3 need to hem = 0.05 p = S4 neck pain p = 0.008 hoarseness S5 = p = 0.20.
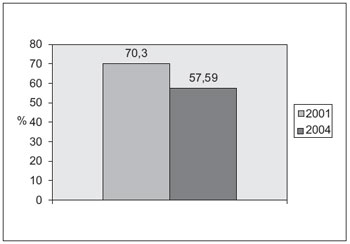
Graphic 2. Evolution of prevalence in percentage Syndrome occupational dysphonia phase 1 to phase 2. - P = 0.
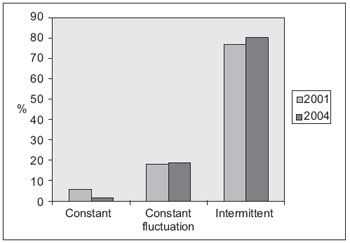
Graphic 3. Prevalence of modalities of hoarseness, in percentage, the syndrome of occupational dysphonia phase 1 to phase 2.
The influence of variables not considered in the questionnaire response was controlled by the method used in their application, because it was distributed and collected in the same act of contact with teachers, making the responses had a spontaneous character and reducing the immediate withdrawal participation. The spontaneity factor as well as ensuring the preservation of information without the need to identify the participant in the collection of responses was emphasized throughout the work.
The processes of health or disease of the vocal tract depends on the preservation of its cellular structure. At this point we find a confluence between the morpho-histological and epidemiological control of occupational dysphonia Syndrome, for sub-optimal use of state or substrate tissue responds by triggering of symptoms until the evolution to occupational laryngopathy.
Complaints of pain or irritation in the throat was the most common symptom reported in the first phase of the study, followed by the symptom of the need for throat clearing, with 74.2% and 58.5% respectively. With the introduction of preventive measures had significantly reduced to 50.5% and 49.0%. The hoarseness, referred to here as any changes in the quality of vocal emission, were reported mainly as intermittent, ie there are periods of greater demand vocal performance and / or the factors that act negatively to exacerbate. Of all the symptoms had the lowest prevalence in phase 1, ie 37.2%. In phase two, unlike the other symptoms, the prevalence increased significantly to 52.3%. This result, which seems paradoxical, can be explained by the fact of being obtained through the self-assessment questionnaire, the teachers, to be guided and advised to increase the risk of acquired vocal auditory perceptual capacity in addition to acquiring a more Careful forward their own voices.
The neck pain prevalence in Phase 1 of 47.4% and foreign body sensation with 41.8% are more related to muscle tension and stress, as well as postural disorders. Of the two, the neck pain was significantly reduced in phase 2 with 30.9%. We can explain this fall by the intervention in the workplace with ergonomic analysis and planning that acted adjusting the posture to the task to be performed, the institution was counseled about the use of chairs and furniture for home. As for foreign body sensation, no significant reduction expresses the influence of other causes beyond the use of voice in occupational dysphonia Syndrome, as the syndrome pharyngo-laryngeal reflux, emotional tension, etc..
The prevalence of occupational dysphonia Syndrome considering the early stage pathogenic discernible was 70.3%, which corresponds to literature data when it is searched under the generic name of occupational dysphonia. With the primary preventive treatment was significantly reduced to 57, 5%.
We do not know how this prevention in those who were served during the early pathogenesis and who benefited, this number was probably higher than the phase discernible because they were less affected and theoretically more vulnerable to security measures.
Analysis of our results it is evident that the primary preventative action in schools can significantly reduce the early stage of pathogenesis discernible above the pathogenesis of advanced in all inconvenience of sick leave that harm the teacher, the Corps Dicentia and Institution.
CONCLUSION The prevalence of pathogenic phase syndrome discernible occupational dysphonia occurred in most college professors and was significantly decreased in control and preventive medical work organization.
Syndrome occupational dysphonia is a new nosological entity which clinically important diagnostic interfere in the natural history of laryngopathies organic.
BIBLIOGRAPHICAL REFERENCES1. Leavell H, Clark EG. Medicina Preventiva. 1 Ed. São Paulo: McGrawHill do Brasil; 1976.
2. 3º Consenso Nacional Sobre Voz Profissional. Rio de Janeiro. 2004.
3. Comissão Tripartite de Normatização para a Voz Profissional. Ministério do Trabalho e Emprego. Questionário de auto-avaliação para professores. São Paulo: Imprensa Oficial do Estado; 2002.
1 Doctor of Medicine and Coordinator of the Committee on Phoniatrics of ABORLCCF. Head of the Labour Relations MTE - Management North / SP.
2 Professor, Department of Otolaryngology and Human Communication Disorders, UNIFESP.
Institution: Ministry of Labour and Employment. São Paulo / SP - Brazil. Mail Address: Sandra Irene Cubas de Almeida - Avenida General Ataliba Leonel, 2764 - Parada Inglesa - São Paulo / SP - Brazil - Zip code: 02242-000 - Telephone: (+55 11) 2973-8927 - E-mail: sandra.almeida@mte.gov.br
Article received on June 11, 2010. Article accepted on June 28, 2010.

