INTRODUCTION The perforation of the nasal septum are occasional findings in ENT examination. Most patients are asymptomatic (1 to 3.4), and estimated that approximately two thirds of people infected show no nasal complaints (1.4). The absence of symptoms is directly related to the size and location of the perforation of the nasal septum (5).
Often, patients come to the ENT complaining of wheezing and nasal crusting and discover they possess a septal perforation. The more subtle symptoms, such as discrete whistles caused by air turbulence, are related to small perforations. The perforations of larger sizes are related to the appearance of scabs, bleeding, runny nose, sensation of nasal obstruction, olfaction, nasal pain, headache and cacosmia (6,7,8,9). If moisture is preserved nasal, septal perforation is usually asymptomatic. The more anterior, more frequent presence of symptoms (3,10,11).
There are several causes of septal perforation (SP). The most common cause is iatrogenic laceration of mucoperichondrium bilaterally during a septoplasty or hematoma formation post-surgical nutrition compromises the quadrangular septal cartilage. Also among the various causes of granulomatous diseases (leishmaniasis, leprosy, Wegener, rhinoscleroma, syphilis, among others), trauma, for example, chemical cauterization for epistaxis, use of narcotics, mainly cocaine, a potent vasoconstrictor as well as drugs used for the treatment of conditions such as nasal corticosteroids and nasal vasoconstrictors.
In this article, we highlight the main causes of nasal septum perforation and review the diagnostic methods currently used. Importantly, recent articles deal mainly with the surgical management of the closure of septal perforations, and less common in the literature a broader approach on the etiology and diagnosis.
Etiology
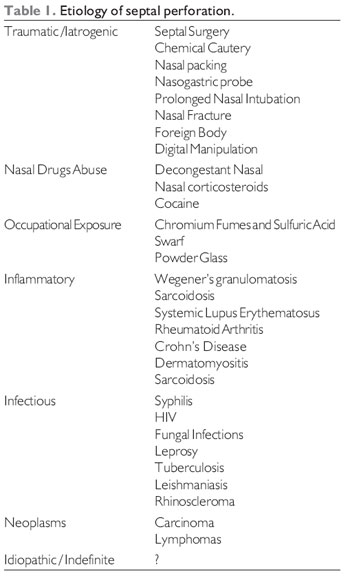
Perforations occur in the septal cartilage injury caused by the loss of integrity of the coating mucoperichondrium, with interruption of blood supply and consequent necrosis. Such injuries can be iatrogenic, traumatic, inflammatory, neoplastic, infectious or inhaling irritants (5). The following table shows the main causes of septal perforation (Table 1).
Iatrogenic and traumatic causes are the most prevalent and occur after surgery septoplasty, septal cauterization, radiotherapy and prolonged nasal tamponade (1,3,5,10,12,13). Prolonged use of nasogastric tube is also described as possible causes of septal perforation (5). The presence of perforation in the postoperative results from the opposing mucoperichondrium lacerations, injury and loss of cauterizing the blood supply by raising the flap mucopericondral (14). Of the patients undergoing nasal surgery, men are the most affected. It explains that higher prevalence in males the greatest number of septoplasty in men (13,15).
The septal perforation after septoplasty are found between 1% and 8% of patients in research. Some authors cite that the number of holes increases when it adopts the technique of Killian, characterized by submucosal resection without addressing the caudal septum. Already in Cottle's technique, which covers the caudal septum, the most common complications are further displacement and postoperative instability (16-19).
The most common traumatic causes are nasal fractures, rhinoliths, foreign bodies, septal hematomas and digital manipulation repeated (1,5,7).
Chronic use of inhalants as irritating nasal decongestants and cocaine can lead to cartilage necrosis by local vasoconstriction, with resultant ischemia, and also by the caustic component present in some of his compositions (10). The use of nasal corticosteroids for the long term is also described as a causative agent of perforations (5.20), particularly in females (21). And the combination of corticosteroids and nasal decongestant seems to increase the occurrence of perforations (22).
Besides the aforementioned irritants, are described in the literature several substances related to PS: chemical and industrial dusts (vapors of chromium, copper, salt, sulfuric acid and hydrochloric acid, cement dust, iron filings, tar, glass powder, soda sodium, calcium oxide, calcium cyanide, arsenic, mercury, phosphorus and benzene) and aerosols used in agriculture.
The bacterial and fungal rhinosinusitis are infectious causes of this disease. They also come within this group, syphilis, HIV, tuberculosis, rhinoscleroma, rinoesporidiose, paracoccidioidomycosis and septal abscesses. Still among the infectious causes are cutaneous leishmaniasis and leprosy, which still show high prevalence in Brazil, with an increasing number of cases reported in all regions (7,23,24).
Wegener's granulomatosis and sarcoidosis are inflammatory diseases most commonly associated with septal perforation (25). Other vascular changes and collagen, the case of systemic lupus erythematosus, also cause degeneration of the nasal septum.
Neoplasms should never be forgotten in the differential diagnosis of septal perforation. The most commonly associated are squamous cell carcinoma, cryoglobulinemia and T-cell lymphomas (5,26).
Diagnosis
The presence of septal perforation is easily diagnosed by the otolaryngologist during his medical history and physical examination and its etiology is rarely defined. Greater diagnostic clarification is due to follow the following steps: questions about nasal symptoms, history of prior use of medication and social habits, rhinoscopy, nasal endoscopy, detection of septal perforation as the appearance, size and location.
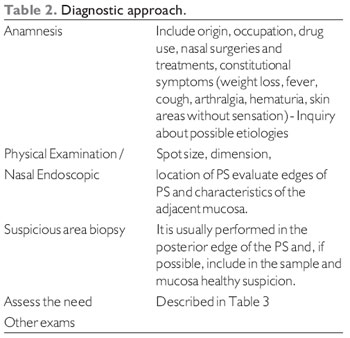
First, the diagnosis depends on obtaining a thorough history, noting the surgery, nasal previous treatments and previous use of inhaled irritants, such as cocaine (10) Table 2.
When symptomatic, the patient presented with typical complaints of wheezing, crusting, nasal obstruction, rhinorrhea, nasal dryness, nasal pain and epistaxis. These complaints are mainly explained by the turbulent nasal airflow. The loss of laminar flow leads to nasal crusting at the edges of perforation, which in turn results in the other signs and symptoms mentioned. The dry nose leads to crusting, epistaxis responsible for the subsequent odor and nasal obstruction. Wheezing is a direct consequence of air flow by drilling (10).
On physical examination, it is important to assess the presence of whitish spots on the skin with loss of sensation and nerve thickening, indicating a diagnosis of leprosy.
On ENT examination, most often during rhinoscopy can be viewed septal perforation.
The septal perforations can be classified by size into small (up to1 cm), medium (1 to 2cm) and large (greater than 2cm). The measurement of size is important not only for legal issue, but mainly for choosing the best therapeutic option (10). This measurement can be done in several ways, all very simple realization. The first is that literature deals with the measurement rule by side which is taking place rhinoscopy. Another technique involves placement of suture to posterior margin of the perforation and with a hemostat, mark the point on the anterior margin, after performing measure with a ruler. Finally, it can be used barium paste at the edges of perforation and, through a lateral view, define the size of perforation.
The size of the drilling, survey Pedroza evaluating 68 patients, we observed that 12% had small perforations, 57% medium and 31% were large (13).
After easy to diagnose structural biggest problem is after, when seeking the causes of perforation.
Rhinoscopy showed a hyperemic mucosa and abundant purulent discharge assumes an infectious cause for perforation, bacterial or fungal. A fungal infection primarily affects immunocompromised individuals. It is confirmed fungal infection by a compatible history and biopsy of infected tissue. It is recommended that the fresh tissue is sent to the laboratory and without previous contact with gauze, measures that facilitate the characterization of fungal infection (10).
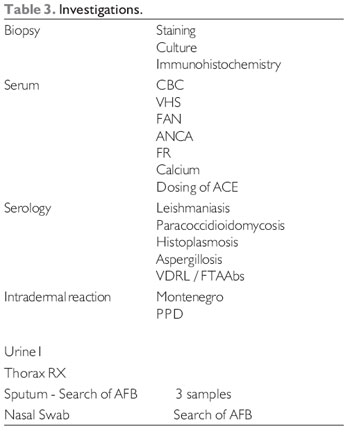
Complementary examinations in the investigation of the etiology of septal perforation are shown in Table 3.
As seen, due to several possible causes of septal perforation laboratory evaluations may be very broad. It is for the otolaryngologist by clinical history and physical examination to discern which tests are most appropriate for each case.
The biopsy is of utmost importance for the etiology of septal perforation and should be done in the initial investigation. In addition to rule out or confirm the presence of cancers such as squamous cell carcinoma (27), makes the differential diagnosis of various diseases. In the case of inflammatory diseases, for example, the presence of vasculitis complements the diagnosis of Wegener's granulomatosis, while the finding of noncaseating granulomas indicate a picture of sarcoidosis (10). If the suspicion of malignancy persists, biopsy should be repeated until diagnosis.
FINAL COMMENTS The etiology of septal perforation should be sought in all patients. A complete history was followed by anterior rhinoscopy, nasofibrocospia exams and appropriate for each case, especially for biopsy of the lesion, are the main means to correct the diagnosis and subsequent therapeutic management.
BIBLIOGRAPHIC REFERENCES1. Brain DJ. Septo-rhinoplasty: The closure of septal perforations. J Laryngol Otol. 1980, 94(5):495-505.
2. Olieveira RCB, Mateus AR, Augusto AG. Perfuração septal. Escolha da técnica cirúrgica. Acta ORL. 2006, 24(3):134-138.
3. Tasca I, Compadretti, GC. Closure of nasal septal perforation via endonasal approach. Otolaryngology-Head and Neck Surgery. 2006, 135(6):922-927.
4. Eng SP, Nilssen EL, Ranta M, et al. Surgical Management of septal perforation: an alternative to closure of perforation. J Laryngol Otol. 2001, 115(3):194-197.
5. Metzinger SE, Guerra AB. Diagnosing and treating nasal septal perforations. Aesthetic Surg J. 2005, 25(5):524-9.
6. Vicenti AB, Lourenço EA, Morgado PF. Cirurgia da perfuração do septo nasal. Em: Campos CAH, Costa HOO, editors. Tratado de otorrinolaringologia. 1ª. ed. São Paulo: Roca; 2003, 5:248-59.
7. RE M, Paolucci L, Romeu R, Mallardi V. Surgical treatment of nasal septal perforations: our experience. Acta Otorhinolaryngol Ital. 2006, 26(2):102-109.
8. Shikowitz, MJ. Vascularized Mucoperiosteal Pull Through Flap for Closure of Large Septal Perforation: A new technique. Laryngoscope. 2007, 117(4):750-755.
9. Kridel RWH. Septal perforation repair. Otolaryngol Clin North Am. 1999, 32(4):695-724.
10. Coleman Jr JR, Strong EB. Management of nasal septal perforation. Current Opinion in Otolaryngology & Head and Neck Surgery. 2000, 8(1):58-62.
11. Foda HMT, Magdy EA. Combining Rhinoplasty with Septal Perforation repair. Facial Plastic Surgery. 2006, 22(4):281-288.
12. Belmont JR. An aproach to large nasosseptal perforations and attendant deformity. Arch Otolaryngol. 1985, 111(7):450-455.
13. Pedroza F, Patrocínio LG, Arevaldo . A review of 25-year experience of nasal perforation repair. Arch Facial Plast Surg. 2007, 9:12-18.
14. Bent JP, Wood BP. Complications resulting from treatment of severe posterior epistaxis. J Laryngol Otol. 1999, 103:66-75.
15. Schulz-Coulon, H-J. Experiences with the bridge flap technique for the repair of large nasal septal perforations. Rhinology. 1994, 32(1):25-33.
16. Gubisch W. Extracorporeal septoplasty for the markdley deviated septum. Arch Facial Plast Surg. 2005, 7(4):218-226.
17. Baterman ND, Woolford TJ. Informed consentt for septal surgery: the evidence-base. J Laryngol Otol. 2003, 117:186-189.
18. Bewarder F, Pirsig W. Long-term results of submucous septal ressection. Laryngol Rhinol Otol (Stuttg). 1978, 57(10):922-931.
19. Rettinger G, Kirsche H. Complications in septoplasty. Facial Plast Surgery. 2006, 22(4):289-297.
20. Kridel RWH. Considerations in the etiology, treatment, and repair of septal perforations. Facial Plast Surg Clin N Am. 2004, 12(4):435-450.
21. Cervin A, Andersson M. Intranasal steroids and septum perforation - an overlooked complication? A description of the course of events and a discussion of the causes. Rhinology. 1998, 36(3):128-32.
22. Døsen LK, Haye R. Nasal septal perforation 1981-2005. Changes in etiology, gender and size. BMC Ear, Nose and Throat Disorders. 2007, 7:1.
23.Martins ACC, Castro JC, Moreira JS. Estudo retrospectivo de dez anos em endoscopia das cavidades nasais de pacientes com hanseníase. Rev Bras Otorrinolaringol. 2005, 71(5):609-16.
24. Falqueto A, Sessa PA. Leishmaniose Tegumentar Americana. Em: Veronesi R, Focaccia R, editores. Tratado de Infectologia. 3ª ed. Rio de Janeiro: Atheneu; 2005, p.1545-59.
25. Baum ED, Boudousquie AC, Li S, Mirza N. Sarcoidosis with nasal obstruction and septal perforation. ENT J. 1998, 77(11):896-902.
26. Knudsen SJ, Bailey BJ. Midline Nasal Masses. Em: Head & Neck Surgery - Otolaryngology. 3rd edition. Lippincott Willians & Wilkins Publishers; 2003. chapter 27.
27. Goulart IMB, Patrocínio LG, Nishioka SA, Patrocínio JA, Ferreira MS, Fleury RN. Concurrent Leprosy and leishmaniasis with mucosal involvment. Lepr Rev. 2002, 73(3):283-284.
1 ENT.
2 Fellowship in Endonasal Endoscopic Surgery and Facial Plastic Surgery. ENT.
3 Endonasal Endoscopic Surgery Fellowship in the Division of Clinical Otorhinolaryngology, HC / FMUSP. Otolaryngologists.
4 Associate Professor, Division of Clinical Otorhinolaryngology, Hospital of the Faculty of Medicine, University of São Paulo.
Institution: Faculty of Medicine, University of São Paulo. São Paulo / SP - Brazil. Mail Address: Department of Otolaryngology, School of Medicine, USP - Avenida Dr. Eneas de Carvalho Aguiar, 255 - 6th Floor - Room 6167 - São Paulo / SP - Brazil - Zip code: 05403-000 - Telephone / Fax: (+55 11) 3088-0299 - E-mail: otorrino.ichc@hcnet.usp.br
Article received on May 13, 2009. Approved on August 10, 2009.