INTRODUCTIONThe increase in age is directly proportional to the presence of several hearing symptoms, such as vertigo, presbycusis and tinnitus (1). Additionally, the prevalence of degeneration in the cervical joint and neck pain in individuals above 50 years of age s high, and severity tends to increase with age(2).
Tinnitus is defined as the perception of a sound in the ears or head without a sound produced by an external source. It impairs approximately 15% of the world population and this prevalence increases for 33% among the individuals above 60 years of age (3). Tinnitus s a symptom frequently accompanied by presbycusis and it is usually more disturbing than hearing loss itself (4).
Currently, it is known that tinnitus appears as the result of the dynamic interaction of several centers of the nervous and limbic systems and that the alterations and/or cochlear lesions are the predecessors of this process, causing a disequilibrium in the inferior paths of the auditory system, resulting in an abnormal neuronal activity, later stressed by the central nervous system and eventually felt as a tinnitus (3). Besides, the afferents from the cervical part with protrusions to the cochlear nucleus indicate an influence of the cervical column reflex to this hearing center (5).
Among the numberless etiologies of tinnitus, the otological, metabolic, cardiovascular diseases; cervical column, dental, neurological, psychiatric and other pathologies related to drug ingestion, alcohol and tobaccoism (6, 7). Not to mention the reduction in the auditory acuity, exposure to noises, head and cervical lesions, factors of life style and mental status (8).
The presence of pain neck and headache is common in tinnitus patients, and it is also verified that these patients can have the symptom influenced by the presence of myofascial trigger-points in the postural muscles of the cervical area, in the scapular waist and in the chewing muscles, where they provoke a spontaneous pain or when moving (9). In patients showing a chronic pain, especially myofascial pain in the cervical area or a degenerating disease of the cervical column, incidence of tinnitus and hearing loss is more elevated than it would be foreseeable in the general population (10).
The objective of this study was to investigate the prevalence of tinnitus and cervical alterations in elderly patients at the ALOS project (Aging and Longevity Study) and verify their probable associations.
METHODA transverse study was performed whose inclusion criteria were elderly people aged 60 or older, both sexes, independent life, classified in levels 3 and 4 of the Functional Status suggested by SPIRDUSO (11), who voluntarily accepted to participate in the study.
The first 147 individuals of the ALOS project (aging and longevity study) were allocated in the city of Londrina. The sampling was randomly and unchangeably defined at a random by taking into consideration the five areas of the city.
In this study, the active curvature movements, extension, lateral neutral extension to the right and to the left, neutral rotation to the right and to the left of the cervical column to evaluate whether there is a reduction of movement width in the studied population by goniometry by using a universal goniometer (Carci, Indústria e Comércio de Aparelhos Cirúrgicos e Ortopédicos Ltda, Brazil) with a two-by-two-degree measurement scale. To measure the cervical MW by goniometry, the measurement system develpoed by KAPANDJI (12) and MARQUES (13) was used: 0-65o, cervical curvature, 0-50o cervical extension, lateral 0-40o curvature to the right and to the left, and 0-55º cervical rotation. The presence of neck pain and tinnitus were verified by applying the standardized questionnaire used during the collections of the ALOS project.
This research was approved by UNOPAR's ethical committee in research under record nº 0070/09.
Chi Square and Relative Risk tests were performed to verify the probable associations between neck pain and the individuals showing and not showing tinnitus, as well as measure the cervical movement width so as to verify any restriction in the joint mobility and a probable association with tinnitus.
For univariate analysis, p<0.01 was considered, and for an inclusion in the final model for Chi Square and Relative Risk test p<0,05 was considered, both had a 95% confidence interval. The statistical software used was SAS 9.1.3
RESULTSThe sample was comprised of 147 individuals aged between 60-95, with an average age of 69.22; 61.90% was (91) and 38.10% was male (56). Out of these individuals, 42.85% (63) had a tinnitus; 36.50% male (23) and 63.50% female (40); among the individuals with tinnitus (63), 61.90% had tinnitus bilaterally, 26.99 on the right ear and 11.11% on the left ear. Also, 51% of the individuals mentioned cervical pain, 70% of whom were female. When performing Chi Square and Relative Risk tests, there was no evidence to believe that there is an association between tinnitus and cervical pain, since p = 0.1984 (p>0.05) (Table 1)
The elderly had a limitation in all the movement widths, as shown by Table 2. In comparison with the presence of tinnitus with the cervical movement width, there was no association between the limitation of cervical movements between people with and without tinnitus, p > 0.05. (Table 3)If the factor tinnitus is disregarded, there is a difference in the sample between the size of cervical rotation limitation according to the side. In this case, the movement width restriction is more limited to the right side than to the left side o p=0.0324 Table 4.
There was no association between the tinnitus-impaired side and the side of movement-restricting width in tinnitus patients either p >0.05.
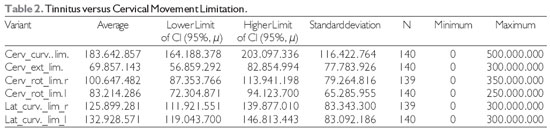
Legend: Cerv.curv.lim : cervical curvature limitation; Cerv. ext. lim.: cervical extension limitation; Cerv rot lim r: Cervical rotation limitation to the right; Cerv curv lim l: Cervical rotation limitation to the left; Lat curv lim r: lateral curvature limitation to the right; lateral curvature limitation to the left.
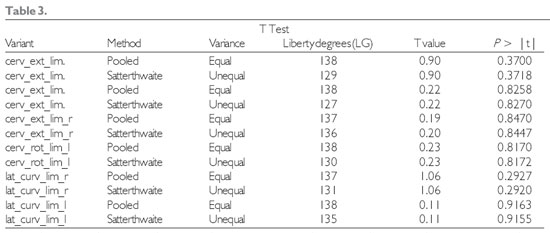
Legend: Cerv.curv.lim : cervical curvature limitation; Cerv. ext. lim.: cervical extension limitation; Cerv rot lim r: Cervical rotation limitation to the right; Cerv curv lim l: Cervical rotation limitation to the left; Lat curv lim r: lateral curvature limitation to the right; lateral curvature limitation to the left.
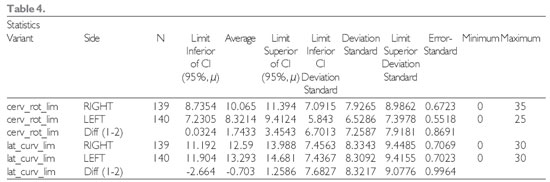
Legend: Cerv.curv.lim : cervical curvature limitation; Cerv. ext. lim.: cervical extension limitation; Cerv rot lim r: Cervical rotation limitation to the right; Cerv curv lim l: Cervical rotation limitation to the left; Lat curv lim r: lateral curvature limitation to the right; lateral curvature limitation to the left.
The tinnitus prevalence in this population was 40%. In a study performed in Japan, the tinnitus prevalence was 18.6% in individuals above 65 years of age; in Australia, it was prevalent in 32.7% above 60 years of age and in Nigeria 41.9% in individuals above 80 years of age (7, 8). Tinnitus can directly or indirectly impair the individual in their professional and leisure activities, interfere with their family and social relationships, and, in extreme cases, lead to suicide. Studies have demonstrated that tinnitus can reduce the elderly's quality of life and reduce their welfare sensation (14).
In a Brazilian study, 406 patients were evaluated within six months, 58% of whom had tinnitus disorder, out of whom 68% were female and 32% were male, compatible with these results, in which among the elderly with tinnitus, 63.50% were female (15).
The studies are controversial with regard to their sex influence when tinnitus is present. Although some show a discreet prevalence in the female gender, others suggest a higher prevalence in the male gender, but a statistical significance is rarely achieved. The possible reason for a higher prevalence in the male gender would be that men are more exposed to occupational noises. Conversely, women show a higher availability of time to search for a doctor, what would explain the findings of a higher prevalence in the female gender. In this study, there was a higher prevalence of female patients (3).
It was verified that 51% of the study population showed a neck pain, equivalent to studies in which the prevalence of neck pain the adult population can range from 6 to 50% (16). Such symptoms are derived from several degenerative processes, direct traumas or from cumulative microtraumas of the postural stress. The reduction in the muscular mass between 50 and 80 years of age is likely the result of the aging process of the neuromuscular system in association with the reduction of the level of physical activity (2).
Research developed by a tinnitus research group showed that this symptom also has a strong association with the presence of myofascial trigger points on the areas of head, neck and scapular waist (9). Besides, it was demonstrated that in tinnitus patients, 75% of the patients showed an influence in the tinnitus intensity according to the movements of head and neck (18). Although the high prevalence of neck pain and tinnitus in our study, there was no association between these two disorders.
The elderly in this show had a reduction in the movement width in all the degrees of movement, the highest of which was in the cervical curvature. However, there was no association between tinnitus and the reduction in the movement width. The width reduces with age in nearly all the studies and there is apparently no intrinsic influence that can reduce this progression. The width reduction of the cervical movements is multifactorial. The degenerating processes must be taken into consideration, whether they are discs, osseous and/or ligamentous, in addition to muscle shortenings and discontinuance (2).
There was no association between the side impaired by tinnitus and the side of the width restriction of movements in the individuals of this study; however, there was a tendency to make a possible association because o the existence, in cases of muscle tension, of a connection between proprioceptive and nociceptive afferents of the cervical area and the cochlear nucleus (9). Based on the literature and the data found in this study, it is believe that in researches with a bigger population, an association between the side of movement width restriction and the tinnitus side can be evident.
CONCLUSIONIt was concluded that tinnitus and neck pain are importantly prevalently in the elderly and that, with aging, there is a reduction in the width of cervical movements in every way - curvature, extension, cervical rotation and lateral curvature, and the highest limitation in the cervical rotation to the right.
There was no association between tinnitus and neck pain or between tinnitus and a reduction of cervical width in this population. There was no association between the tinnitus-impaired side and the side of movement-restricting width in tinnitus patients either. The results of this preliminary study demonstrated the need for more researches and the advanced number of this sample to actually come to a conclusion of these associations.
REFERENCES1. Ganança FF, Gazzola JM, Ganança CF, Caovilla HH, Ganança MM, Cruz OLM. Quedas em idosos com Vertigem Posicional Paroxística Benigna. Braz J Otorhinolaryngol. 2010, 76(1):113-20.
2. Carvalho CO, Magalhães DAS, Silva Junior JAA, Bicalho LFH, Costa APB, Costa LOP, Figueiredo VF. Estudo comparativo das amplitudes de movimento da coluna cervical em idosos com diferentes níveis de aptidão física. Acta Fisiatr. 2006, (13):347-51.
3. Pinto PCL, Sanchez TG, Tomita S. Avaliação da relação entre severidade do zumbido e perda auditiva, sexo e idade do paciente. Braz J Otorhinolaryngol. 2010, 76(1):18-24.
4. Ferreira LMBM, Ramos NA, Mendes EP. Caracterização do zumbido em idosos e de possíveis transtornos relacionados. Rev Bras Otorrinolaringol. 2009, 75(2):245-8.
5. Biensinge A, Reibhauer A, Mazurek B. Halswirbelsäule. The role of the cervical spine and the craniomandibular system in the pathogenesis of tinnitus. Somatosensory tinnitus. HNO. 2008, 56:673-677.
6. Okada DM, Onishi ET, Chami FL, Borin A, Cassola N, Guerreiro VM. O uso da acupuntura para alívio imediato do zumbido. Rev Bras Otorrinolaringol. 2006, 72(2):182-6.
7. Lasisi AO, Abiona T, Gureje O. Tinnitus in the elderly: Profile, correlates and impact in the Nigery study of ageing. Otolaryngol Head Neck Surg. 2010, 143:510-515.
8. Michikawa T, Nishiwaki Y, Kikuchi Y, Saito H, Mizutari K, Okamoto M, and Takebayashi T. Prevalence and Factors Associated with Tinnitus: A Community-Based Study of Japanese Elders. J Epidemiol. 2010, 20(4):271-6.
9. Rocha CACB, Sanchez TG, Siqueira JTT. Pontos-gatilho Miofasciais: Ocorrência e Capacidade de Modulação em Pacientes com Zumbido. Arq Int Otorrinolaringol. 2006, 10(3):210-7.
10. Hamill-Ruth RJ; Ruth RA; Cyd CD, Cook A. Management of Tinnitus and hiperacusis using a multidisciplinary pain model. APS Bulletin. 2000, 10(5):126-7.
11. Spidurso WW. Dimensões físicas do envelhecimento. Barueri: Manole; 2005
12. Kapandji IA. Fisiologia articular: esquemas comentados de mecânica vertebral: tronco e coluna vertebral. 5ª ed. São Paulo: Pan-Americana; 2000.
13. Marques AP. Manual de Goniometria. 2ª ed. São Paulo: Manole; 2003
14. Steinmetz LG, Zeigelboim BS, Lacerda AB, Morata TC, Marques JM. Características do zumbido em trabalhadores expostos a ruídos. Rev Bras Otorrinolaringol. 2009, 75(1):7-14.
15. Pinto PCL, Hoshino AC, Tomita S. Características dos pacientes com queixa de zumbido atendidos em ambulatório especializado - HUCFF. Cad Saúde Coletiva. 2008, 16(3):437-48.
16. Kettler A, Werner K, and Wilke HJ. Morphological changes of cervical facet joints in elderly individuals. Eur Spine J. 2007, 16(7):987-92.
17. Chaves TC, Nagamine HM, Belli JFC, de Hannai MCT, Bevilaqua-Grossi D, Oliveira AS. Confiabilidade da fleximetria e goniometria na avaliação da amplitude de movimento cervical em crianças. Rev Bras Fisioter. 2008, 12(4): 283-9.
18. Björne, A. Assessment of temporomandibular and cervical spine disorders in tinnitus patients. Prog Brain Res. 2007, 166:216-9.
1) Specialist, Taking Master Degreee in Rehabilitation Science at UNOPAR. Physiotherapist admitted after a public examination by the Family Health's Program.
2) Doctor in Medicine and Health Science. Master Degree's Professor of Rehabilitation Science at UNOPAR.
3) Doctor in Nursery, USP's Nursery School of Ribeirão Preto. Professor, North of Parana University, PR.
4) Bachelor in Statistics - University of Brasilia, 2008. Odds&Actions's Managing Partner and Counsellor at the Regional Council of Statistics - 1st Region.
5) Specialist in Audiology, taking Master Degree in Rehabilitation Science at UNOPAR. Cismepar's Phonoaudiologist.
Institutition: North of Parana University - UNOPAR. Londrina / PR - Brazil. Mailing address: Michelle Damasceno Moreira - Rua Augusto Guerino, 195 Apto 35 - Bairro: Portal de Versailhes 1 - Londrina / PR - Brazil - ZIP Code: 86057-240 - Telephone: (+55 43) 3178-0336 / 3371-7990 / 9161-5577 - Email: micmoreira@yahoo.com.br
Article received on April 6, 2011. Article approved on May 23, 2011.


