INTRODUCTIONThe contamination by lead affects all the systems in human body, especially the nervous system. The clinical manifestations depend on the intensity of time of exposure and individual sentivity (1).
The tolerated level in human organism, according to the American Disease Control Center (2) is of up to 10 g/dL, however some studies (3-9) revealed harmful effects to the health in concentrations inferior to 10 g/dL.
The lead effects in the auditory system, there is no consensus in the literature. In January of 2002, at Bauru city, there was prohibition of a factory due to emission of particles of lead to the environment, superior to the allowed. This event enabled the study of the effects of lead alone. The studies (10,11) performed did not show changes in the functioning of outer hair cells, auditory nerve and brainstem.
It is known that the contamination by lead may affect the development of central nervous system, may cause attention deficit, concentration, memory, intelligence, learning, perceptive processes, psychomotor development and interpersonal (12-14), among others.
The Auditory Processing is a set o processes and mechanisms which occur in the hearing system in response to acoustic stimulus and that are responsible for localization and lateralization of sound, discrimination and recognizing the hearing patterns, temporal aspects of hearing, hearing performance with competing acoustic signals and with degradation of acoustic signal (15). For these skills develop properly, it must have functional and structural integrity of peripheral and central auditory system.
Considering that the contamination by lead may affect some functions of central nervous system, it was judged necessary to perform a prospective study of the level of blood lead in children exposed to lead and their performance of behavior tests, chosen to triage the hearing processing, in order to help the investigation of relating between the lead and hearing processing changes.
Thus, this work has as objective to check the performance of the children exposed to lead in hearing processing tests.
METHODThis study was approved by the Ethics and Research Committee of University of Sao Paulo, College of Odontology of Bauru, protocol number 73/2010.
90 children participated of this study of masculine and feminine genders, at age between 7 to 15 years-old.
The inclusion criteria were: reside at Bauru city in the area where there was emission of particles of lead above the permissible; parents consent to evaluation and publishing of the results; lead level equal or superior to 10 g/dL; audiometry with results within the normal range in the frequencies tested; tympanometry curve type A.
The children were submitted to Pure Tone Audiometry in the frequencies from 500 to 4 KHz and to tympanometry. In order to get the hearing processing it was used Auditory Fusion Test-Revised (AFT-R) subtest 1(16) and the dichotic listening test (binaural integration stage) (17).
The AFT-R evaluates the temporal resolution, determining the duration in milliseconds (ms), in which the listener is able to distinguish a brief interval of silence between two pure tones. It was considered as good performance to the perception of sound in an interval equal or inferior to 60ms and as poor performance, the perception of sound in an interval superior to 60 ms.
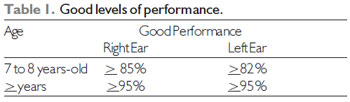
The Dichotic Listening Test consists in four presentations of a list of two digits of two-syllable in Brazilian Portuguese, in which four different digits are presented simultaneously, two in each ear, characterizing a dichotic task. The results were classified as good performance according to the Table 1, being considered poor performance values inferior to the described in the Table (17).
All of the children evaluated had samples of blood collected in order to determine the levels of blood lead. These examinations were conducted by Municipal Health and performed at Adolfo Lutz Institute (IAL/SES-SP).
It was performed statistical analysis of the results, being used instruments for descriptive analysis and the Spearman test to check the correlation between the data.
RESULTSFrom 90 children evaluated, 14 were excluded from the sample because they had changes in audiometry or tympanometry. Others 3 (3, 3%) were excluded for presenting lower lead levels to 10 g/dL. Therefore it was analyzed the results of hearing processing results in 73 children, which corresponds to 81, 1% of initial established number. Thus, total number was fixed as 73, so it would be possible to perform statistical analysis.
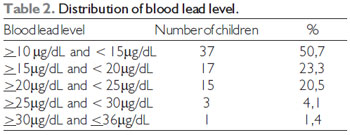
From these children, 32 (43,8%) were from feminine gender and 41 (56,2%) of masculine, with average age of 9,5 years-old. The blood lead level varied from 10 to 30,2 g/dL, according to described on Table 2, and the corresponding average of 15,8 g/dL (standard deviation of 4,8).
Related to the hearing processing tests, the AFT-R presented minimum result of 10ms and maximum of 200ms, being the average 90ms and the standard deviation, 62. According classification proposed in the methodology, 44 (60,3%) children evaluated presented poor performance in this test, in other words, superior results to 60ms.
For analysis of the dichotic listening test separation was made between the right ear and left ear. The minimum value found was 40% (OD) and 23,7% (OE), and the maximum was 100% in both ears. This test was performed in only 52 children. Thus, following the classification criteria proposed in methodology, 13 (25%) presented good performance in both ears; 20 (38, 5%) presented poor performance in both ears; 4 (7, 7%) presented poor performance only on the right ear; 15 (28, 8%) presented poor performance in the left ear.
According to the result of Spearman correlation test, there was no statistical significance between the lead level and the hearing processing results.
DISCUSSIONIn order to a listener realize the silence interval between two sounds; this interval should be increased till 17ms. The judgment of the temporal order seems to be independent of the nature of acoustic sounds (18). In this way, any with threshold detection range greater than 20ms probably has deficit in the ability of temporal resolution, which interferes on the perception of normal speech and in recognizing phonemes. So, when the greater is the interval detection threshold, in milliseconds, great is the probability of a deficit in temporal processing.
It was consulted several data basis, thus it was not found study with subjects in similar conditions to this present study. The results found were compared to other literature finding and with normal range of the tests.
In school-age children (6 to 10 years-old) without hearing change, a study showed the mean thresholds of AFT-R were 10 ms inferior and to the children with risks of changes in the language development (sensory deprivation and hearing, learning difficulties) the thresholds were greater than the interval of confidence interval established (15ms) (19).
Other work presented threshold of auditory fusion ranging between 56,25ms and 59,75ms in children with cleft lip and palate from 11,44ms to 14,42ms in children without cleft (20).
In this study it was found mean threshold of 91 ms to the children evaluated contaminated by lead, obtained in the subtest 1 of AFT-R. The minimum threshold found war of 10 ms and the maximum was of 200 ms. Despite of not being possible to compare with the studies cited above, it is possible to affirm that these results are below to the expected at age of the children evaluated.
As regards proof of digits dichotic, the presented performance by young adults was a higher percentage of correct answers than 90% in threes steps (binaural integration, directed attention to the right and directed attention to the left), coinciding with international findings (17).
In a study (21) which investigated the simultaneous exposure to lead and to noise about hearing nervous system in 43 workers from a factory of batteries in Brazil, it was used the following procedures: measure of the level of lead in blood (Pb-S), Tone Audiometry, Tests such as the dichotic listening, Sentences Identification Competitive (SSI), Dichotic listening digits, Dichotic Dissyllable Listening (SSW), and Filtered Speech. From these 43 research participants, 17 was exposed to the noise levels of 96 dBA, and 26 were exposed to noise (84 dBA) and lead. For the dichotic digit test (binaural integration) it was not observed changes in exposed subjects only in noise, however, 50% of the group of subjects exposed to lead and to noise presented change.
In this study, evaluated children were exposed to lead (differently to the subjects from the study aforementioned, in which the subject were exposed to other agents, like noise), which allowed a possible analysis of interference of isolated lead contamination in the abilities of hearing processing. However, in the dichotic listening test, it was found an average of 89% for the right ear, and 84% for left ear, being these values lower than described in literature as normal range.
In order to identify possible changes in peripheral and central hearings in workers who was exposed to metallic mercury, researchers (22) performed the tests of tone audiometry (air and bone), and impedance audiometry (tympanometry and stapedial reflex), and that workers had mean exposure of six years. As conclusion, it was identified both peripheral and central auditory disorders in these subjects.
Other authors (23) studied the cognitive function using a mode of late evoked potential (P300) in 22 workers, whose lead concentration in blood was between 12 to 59 µg/dl. The P300 latency was significantly longer compared to the control group, showing correlation with lead level in blood. The authors evaluated, this same sample, the speed of peripheral nervous conduction. The results showed that the speed is slower in the workers exposed, Bing this correlated to the same way of presence of lead level in blood. No significant correlation was found and between the speed of nervous conduction and the P300, This led the authors to conclude that the mechanism of the effects of lead in the Central Nervous System it seems to be different from the effect of the mechanisms in peripheral nervous system. Moreover, these researchers claimed that the results of this study suggest that lead affect the cognitive function, as well as the functions of central auditory nervous system
Although the analysis did not show statistical significance between the performed tests, when comparing to the other results it is visible that these children present some kind of change in hearing processing, that may lead to problems in development in hearing skills, in communication and reading and writing development.
CONCLUSIONThe performance of the children exposed to lead was inferior to the described by literature, however there were no statistical correlation between intoxication by lead and the development of hearing processing abilities.
BIBLIOGRAPHIC REFERENCES1. Minozzo R, Minozzo EL, Deimling LI, Minozzo RSM. Plumbemia em trabalhadores da indústria de reciclagem de baterias automotivas da Grande Porto Alegre, RS. J Bras Patol Med Lab. 2008, 44(6):407-12.
2. Centers for Disease Control (CDC). Agency for Toxic Substances and Disease Register. Case studies in environmental medicine: lead toxicity [Internet]. [citado 2009 novembro 30]. Available from: http://wonder.cdc.gov/wonder/prevguid/p0000017/p0000017.asp#Table_1
3. Balbus-Kornfeld JM, Stewart W, Bolla KI, Schwartz BS. Cumulative exposure to inorganic lead and neurobehavioural test performance in adults: an epidemiological review. Occup Environ Med. 1995, 52(1):2-12.
4. Lindgren KN, Masten VL, Ford DP, Bleecker ML. Relation of cumulative exposure to inorganic lead and neuropsychological test performance. Occup Environ Med. 1996, 53(7):472-7.
5. Hänninen H, Aitio A, Kovala T, Luukkonen R, Matikainen E, Mannelin T, et al. Occupational exposure to lead and neuropsychological dysfunction. Occup Environ Med. 1998, 55(3):202-9.
6. Rodrigues OMPR, Almeida SH, Ribeiro T. Avaliação do desenvolvimento de crianças de 1 a 3 anos de idade contaminadas por chumbo. In: Neme CMB, Rodrigues OMPR, organizadores. Psicologia da saúde: perspectivas interdisciplinares. São Carlos: RIMA Editora; c2003. p.73-94.
7. Campbell TF, Needleman HL, Riess JA, Tobin MJ. Bone lead levels and language processing performance. Dev Neuropsychol. 2000, 18(2):171-86.
8. McGeehin MA. El envenenamiento infantil por plomo: un problema de años que demanda soluciones nuevas salud pública de México. Salud pública Méx. 2003, 45(2):179-180.
9. Lanphear BP, Dietrich K, Auinger P, Cox C. Cognitive deficits associated with blood lead concentrations <10 microg/dL in US children and adolescents. Public Health Rep. 2000, 115(6):521-9.
10. Alvarenga KF, Jacob LCB, Martins CHF, Costa AO, Coube CZV, Marques JM. Emissões otoacústicas - produto de distorção em sujeitos expostos ao chumbo e ao ruído. Rev Bras Otorrinolaringol. 2003, 69(5):681-9.
11. Alvarenga KF. Avaliação do sistema auditivo periférico e central em crianças com histórico de contaminação por chumbo. Tese de Livre Docência da Faculdade de Odontologia de Bauru-USP; 2006.
12. Schnaas L, Rothenberg SJ, Perroni E, Hernández RM, Hernández C, Martinez S. Relación entre la exposición prenatal y posnatal al plomo y el desarrollo intelectual del niño a los 42 meses de edad. Perinatol Reprod Hum. 1999, 13(3):214-20.
13. Meyer PA, Brown MJ, Falk H. Global approach to reducing lead exposure and poisoning, mutation research. Mutation Research/Reviews in Mutation Research. 2008, 659(1-2):166-175.
14. Feldman RG. Effect of toxins and physical agents on the nervous system. En: Bradley WG, Daroff RB, Fenichel GM, Marsden CD (eds). Neurology in Clinical Practice. Boston: Butterworth-Heinemenn; 1991.
15. American Speech-Language-Hearing Association. Central Auditory Processing: Current Status of Research and implications for Clinical Practice. A Report from ASHA Task Force on Central Auditory Processing. Rockville, USA, 1995.
16. McCroskey RL, Keith RW. Auditory Fusion Test-Revised (AFT-T), Auditec of St. Louis; 1996.
17. Santos MFC, Pereira LD. Escuta com dígitos. In: Pereira LD, Schochat TE. Processamento Auditivo Central-manual de avaliação. São Paulo, Lovise, 1997.
18. Bellis T. Assessment and management of central auditory processing disorders in the educational setting from science to practice. 2. ed. New York: Delmar Thompson; 2002.
19. Costa LP, Pereira LD, Santos MFC. Auditory fusion test in scholars. Pro Fono. 2004,16(2):187-96.
20. Cassab TV, Zorzetto NL. Teste da fusão auditiva-revisado (AFT-R) em crianças com fissura labiopalatina. ACTA ORL/Técnicas em Otorrinolaringologia. 2006, 24(4): 272-276.
21. Jacob LCB. Efeitos da exposição simultânea ao chumbo e ao ruído sobre o sistema nervoso central em trabalhadores de uma fábrica de baterias [Tese de doutorado]. Universidade de São Paulo, Bauru, 2000.
22. Lima ERZ, Colon JC, Souza MT. Alterações auditivas em trabalhadores expostos a mercúrio. Rev CEFAC. 2009, 11(supl.1):0.
23. Araki S, Murata K, Yokoyama K, Uchida E. Auditory event-related potential (P300) in relation to peripheral nerve conduction in workers exposed to lead, zinc, and copper: effects of lead on cognitive function and central nervous system. Am J Ind Med. 1992, 21:539-47.
1) Speech Therapist. Master´s student of Post-Graduation program of College of Odontology of Bauru - University of São Paulo, Speech Therapist area.
4) PhD. Professor Doctor of Speech Therapist Department of College of Odontology of Bauru - University of São Paulo
5) Associate Professor. Teacher Associated to Department of Speech Therapist Department of College of Odontology of Bauru - University of Sao Paulo
6) Professor. Professor of Speech Therapist Department of College of Odontology of Bauru - University of São Paulo
Institution: University of Sao Paulo, College of Odontology of Bauru, Speech Therapist Department, Speech Therapist Clinic. Bauru / SP - Brazil. Mailing address: Mariza Ribeiro Feniman - 9-75 Dr Octávio Pinheiro Brizolla, alameda - Vila Universitária - Bauru / SP - Brazil - Zip-code 17012-901 - Telephone: (+55 14) 3235-8332 - E-mail: feniman@usp.br
Article received in 2011 May 18th. Article approved in 2011 June 25th.