INTRODUCTIONOtoacoustic Emissions (OAE) are sounds which emerge from hearing canal when (paradoxically) tympanic membrane receives vibrations from cochlea transmitted by middle ear (Kemp, 2002). These vibrations occur as a by-product of a specific and vulnerable cochlear mechanism known as "cochlear amplifier" and highly contribute to hearing sensitiveness and discrimination of frequencies (Kemp, 1978; Kemp, 2002). This exam can be done in any clinical circumstances in which the target of the evaluation is to observe cochlea job (Kemp, 1997; Kemp, 2002) (10,12).
In clinical practice, emissions can be recorded either in spontaneous and evoked manner by acoustic stimulation. The latter is divided in two types: Transient Evoked Otoacoustic Emissions (TEOAE), expelled by short term acoustic signals (clicks) and Otoacoustic Emission by Distortion Product (OAEDP), evoked by 2 pure tones of different frequencies simultaneously (Gattaz e Cerruti, 1994) (5).
In most of healthy ears, OAE are present, and they can be registered when thresholds are better than 25dBNA in frequencies of 250Hz to 8KHz in TEOAE and in OAEDP, better than 45dBNA in the same frequencies (Kemp and col., 1986; Harris et al., 1991, Harris and Probst, 1997; Lopes Fo. and Carlos, 2005). When cochlear is involved by noise exposure, acoustic trauma, drug administration, surgery, age and contralateral stimulation, TEOAE can suffer alterations, in both composition of frequencies and in amplitude (Harris et al., 1991), for this reason it is a sensitive technique to identify changes on cochlear job (Kemp, 2002) (7,8,10,11,15).
By the fact that ototoxicity associated with cisplatin administration often is presented with hearing loss and tinnitus, some authors examined the use of OAE in experimental studies (Sie e Norton, 1997; Sockalingam et al., 2000) while others recommended the use of TEOAE as a method of hearing monitoring in therapy involving Cisplatin (CDDP) (Zorowka et al., 1993; Allen et al., 1998). Nevertheless, most of them do not provide a clear or precise criterion of loss of amplitude of the TEOAE, which identifies or determines the beginning of cochlea suffering. Therefore, there is the need of studies to obtain variation of TEOAE in normal individuals and then later comparison and monitoring of hearing system in patients with cancer (1,17,18,19).
This study intends to analyze variations of relative amplitude of TEOAE found in normal individuals among three different sessions.
MATERIAL AND METHODThis study was presented and approved by Ethics Committee under protocol number 00-11054-4.
Normal individuals, both men and women, were invited to take part in this study. They were selected by the following criteria:
- absence of hearing complaint;
- absence of middle ear alteration or otologic background;
- absence of occupational noise exposure; and
- absence of ototoxic drug therapy.
To take part in this study, all individuals should present normal tonal threshold in all frequencies tested from 0.25 to 8 kHz and integrity of middle ear, with presence of tympanometric curve type A in both ears. The evaluation of tympanum-ossicular system was performed using Mini Timp Interacoustics MT10 and it was repeated in all sessions of records of EOAT.
There were 35 individuals, 28 were female, aging from 21 and 40 years. Each of them was submitted to 3 records of TEOAE within one-week interval at least between them. Those were performed in acoustically designed room, using ILO 292 (Otodynamics Ltda. Versão 92), connected to a portable computer Toshiba.
It was used a non-linear stimulus with spectrum covering frequencies from 0.8 to 4kHz, with record of 260 clicks, adjusting the gain of the equipment in a way to keep intensity of stimulus between 79 and 82 dB. The stimulus spectrum was observed in a way to keep it in homogeneous form, so all frequency bands could receive energy in regular way. Therefore, this homogeneity was not necessary achieved.
The spectrum of responses (from EOAT) corresponded to frequencies from the used stimulus (Lopes Fo. and Carlos, 2005) and was considered in bands of half-eighth centralized in 1.0k, 2.0k, 3.0k and 4.0kHz (15).
The criteria for the presence of responses was a correlation of at least 50% of global reproductivity in each of tested frequency band, and global amplitude and by bands of at least 3dB (S/R and 3dB), yet noise could not exceed 40dB.
Variations of relative amplitude (S/R) were analyzed in each evaluation of each ear tested in all frequency bands, considering in a separate way the positive variations (increase of amplitude), negative ones (reduction of amplitude), and null ones (maintenance of amplitude).
Data were submitted to statistical analysis using tools of descriptive statistics, of distribution of central frequencies, of changeability and of measures of tendencies to describe frequencies and Paired Wilcoxon signed-test (level of significance of 5%).
RESULTSResponses to researches of otoacoustic emissions could be recorded in all tested ears, although, to some individuals, in some sessions, some frequency bands did not achieve a definite criteria of presence of responses (SNR = 3dB), and were excluded individually.
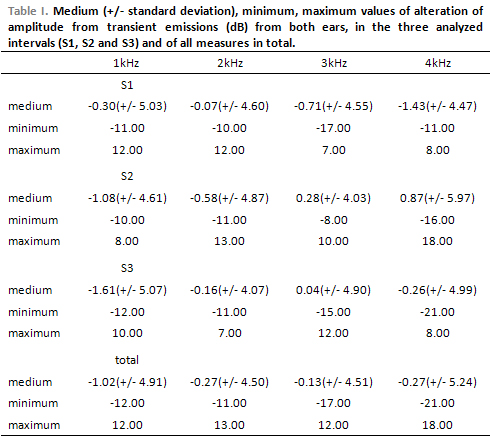
Table 1 shows the averages of standard deviation of amplitude variation from the responses from the first to the second evaluation (S1), from the second to the third evaluation (S2), from the first to the third evaluation (S3), obtained from examined individuals with normal hearing.
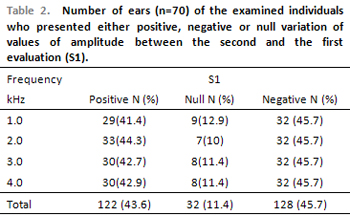
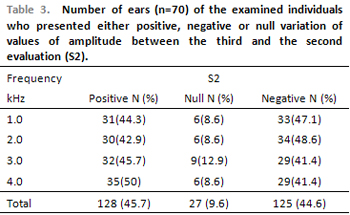
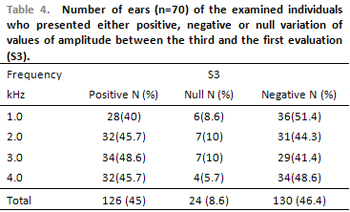
Tables 2, 3 and 4 show that null variation of amplitude of responses of the OAE is less frequent in all tested frequencies in different intervals of tests.
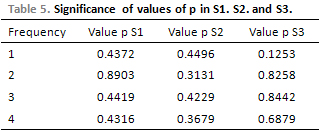
Table 5 shows that there was no significant difference of variation values of amplitude from different sessions of evaluation.
DISCUSSIONOtoacustic emissions reveal the action of active biological mechanisms in each cochlea, responsible for a unique sensitiveness, for an accurate selection of frequency and for great dynamic band of the normal hearing system (Norton et al., 1999) (16).
If emissions change before hearing suffers any alterations, it is possible an intervention before definite hearing loss occurs. Indeed, Lapsley Miller et al. (2004) suggest that there is a redundancy in the number of external ciliated cells, so lesion of considerable number of cells do not result in reduction of hearing threshold, but in the amplitude of otoacoustic emissions (13).
Hearing monitoring can result in early detection of ototoxic-drug-induced hearing loss and occupational noise, what it can cause important prophylaxis action.
Although Harris et al. (1991), Littman et al. (1998), and others, have observed the contribution of the research of distortion product emissions to identify ototoxic effects, Guedes et al. (2002) observed greater variety of responses from EOAPD, especially in frequencies above 4 kHz, rather then from EOAT. We chose to perform EOAT in this study because of the quickness of record, because of available spectrum information in the software ILO 292 and because we searched minimum variations of amplitude. On the other hand, it is not proved that the presence of ototoxic effect in acute frequencies extend to conventional ones, even after cumulative doses. In most of cases, interruption or change of therapy is not studied, unless hearing loss interferes in speech perception, in communication or in language development. So, early identification of ototoxic effects in frequencies up to 4 kHz is totally relevant (6, 8, 14).
Results show the same variation in all frequencies, in all sessions of evaluation. In the same way, Tables 2 and 4 show that variations can be for both increase and reduction of amplitude in subsequent test, so there is a shorter occurrence of null variations.
To a proper record of the EOA, besides verification of probe placement, of patient's noise (breathing and swallowing) and of the environment, there was a concern with the integrity of tympanum-ossicular system, though in pathological conditions, the effects of mass and rigidity present a function unbalance, changing the standard of transmission of sound wave that intends to achieve inner ear and also interferes in the transmission of cochlear emissions, which intend to achieve tympanic membrane (Lopes Fo. and Carlos, 2005) (15).
Understanding how external factor interferes on TEOAE is important to obtain valid results and to determine situations in which changes can be especially assigned to cochlear factor. External factors such as situation of external hearing canal and middle ear, environment noise and intensity of stimulus were controlled, whenever possible, during the study in order to consider variations found as they arose from cochlear events. All individuals presented normal tympanometric curves and presence of estapedial reflex in all frequencies tested in bilateral manner, in all session of evaluation. In order to make evaluations similar, there was control of variable of external noise and the equipment (limited to 40 dB), of the stimulus intensity, which was adjusted manually at about 80 dB, number of presentations, although Kemp (1997) suggested that 50 responses obtained in quiet places (above level of rejection) would be enough to consider an acceptable and reliable response. The record remained in 260 stimulus (8,9).
It is expected that any changes on the responses from individuals submitted to conditions of risk regarding hearing should be greater than the detected test-retest normal intra-individuals variation (Lapsley Miller et al., 2004). At the same time, the decision if variation was due to cochlea suffering requires the knowledge of the greateness of the difference from the professional (Beattie et al., 2003). Therefore, we could observe in our samples that the same individuals with normal hearing are subject to variations that exceed even the criteria of presence and absence of it (SNR > 3dB) (2,13).
Although amplitudes of OAE can differ between normal ears, they are often similar between both, right and left (Kemp, 2002) and in spite of the great variety of amplitude found in both our results and in the literature, Zorowka et al. (1993) said that variations are constant in the same individual. Indeed, in spite of the variety identified in our study, there was no significant difference between averages from the three recorded sessions (10,19).
Among the studies which presented the reproductivity of emissions, Franklin et al. (1992) found variation about 2dB in amplitude of the TEOAE in 12 normal individuals. The same variation was found in 10 normal individuals in a study done in 3 sessions within 3-day intervals between them (Harris et al., 1991). In Guedes et al. (2002) global amplitude variation of transient evoked emissions was 3.69dB (DP +/- 2dB) (4,6,8).
Lapsley Miller et al. (2004) studied 472 individuals aging from 14 to 49 years with different grades of noise exposure during 4 years, though in the fourth year only 42 individuals could be followed. The target of it was to evaluate the changes of amplitude of the emissions and the correlation with tonal threshold every year. They also examined 106 ears of non-noise-exposed individuals. They observed that the greatness of variation of transient emissions with non-linear stimulus at 74 dB was similar to the group with and without exposure, so it cannot be assigned to noise. The variation of amplitude in the group without exposure was between -0.46 dB and -0.48 dB. Authors tested non-linear emissions at 74 dB by the fact that the transient emissions at the level provide high test-retest confidence and shorter product in all types of emissions (13).
Harris et al. (1991) outlined that the responses of shorter amplitude varied in a similar way to the great amplitude. According to the results, the greater variation found was in the frequency of 0.7 kHz (2 dB, SD = 1.5 dB) and the shorter difference was in 2.4 kHz (0.8 dB, SD = 0.57 dB) (8).
Chan and Mc Pherson (2000) have lately studied the reproductivity of transient emissions and with tone-burst from 30 young Chinese with normal hearing in three sessions of evaluation. They found that differences of test-retest had never varied more than 6dB in global response and no more than 11 dB in response by band. The variation average was 0.81 in frequency of 1 kHz.3.
Although, in our study, it was not possible to quantify variation of amplitude found due to high standard deviation, it was not observed statistically significant change among tests. This enables the possibility to use emissions as a reliable test of cochlear function and disfunction, though the intrasubject change should be explained in a careful and individual manner.
REFERENCES1. Allen GC, Tiu C, Koike K, Ritchey AK, Jurs-Lasky M, Wax MK. Transient evoked otoacoustic emissions in children after cisplatin chemotherapy. Otolaryngol Head Neck Surg 1998;118:584-588.
2. Beattie RC, Kenworthy OT, Luna CA. Immediate and shortterm reliability of distortion-produtct otoacoustic emissions. Int J Audiol 2003;42:348-354.
3. Chan RH, Mc Pherson B. Test-retest reliability of toneburst- evoked otoacoustic emissions. Acta Otolaryngol 2000;120:825-834.
4. Franklin DJ, McCoy MJ, Matin GK, Lonsbury-Martin BL. Test-retest reliability of distortion-protuct and transiently evoked otoacoustic emissios. Ear and Hearing 1992;13(6):417-29.
5. Gattaz G, Cerruti VQ. O uso do Registro de Emissões Otoacústicas Evocadas para Triagem Auditiva em Neonatos de Risco para Deficiência Auditiva. Revista Paulista de Pediatria 1994 Set; 12(3):291-4.
6. Guedes MC, Passos SN, Goffi-Gomez MVS, Bento RF. Estudo da reprodutibilidade das emissões otoacusticas em indivíduos normais. Rev. Bras. Otorrinolaringol. 2002 jan/fev;68(1):34-38.
7. Harris FP, Probst R. Otoacoustic emissions and Audiometric Outcomes IN: Robinette MS, e Glattke TJ. Otoacoustic Emission. Clinical Applications. Thiemi. New York. 1997. cap.8.
8. Harris FP, Probst R, Wenger R. Repeatability of transiently evoked otoacoustic emissions in normally hearing humans. Audiology 1991;30:135-41.
9. Kemp DT. Otoacoustic Emissions in Perspective. In: Robinette MS, Glattke TJ. Otoacoustic Emissions. Clinical Applications. Thieme. New York. 1997.
10. Kemp DT. Otoacoustic emissions, their origini in cochlear function, and use. British Medical Bulletin 2002, 63:223-241.
11. Kemp DT, Bray P, Alexander L, Brown AM. Acoustic Emission Cochleography; Pratical aspects. Scand. Audiol. Suppl. 1986;25:71-85.
12. Kemp DT. Stimulates acoustic emissons fron within the human auditory system. J Acoust Soc Am 1978;64:1386-91.
13. Lapsley Miller JA, Marshall L, Heller LM. A longitudinal study of changes in evoked otoacoustic emissions and puretone thresholds as measured in a hearing conservation program. Int J Audiol 2004;43:307-322.
14. Littman TA, Magruder A, Strother DR. Monitoring and predicting ototoxic damage using distortion product otoacoustic emissions: pediatric case study. J Am Acad Audiol 1998;9:257-262.
15. Lopes Fo O, Carlos RC. Emissões Otoacústicas. In: Lopes Fo. O. (ed.) Tratado de Fonoaudiologia. São Paulo. Tecmedd. 2a ed. 2005. Cap.10.
16. Norton SJ & Stover LJ. Emissões Otoacústicas: um novo instrumento clínico.In: Katz J. Tratado de Audiologia Clínica. São Paulo: Manole cap.29 pp.44-458
17. Sie KC, Norton SJ. Changes in otocoustic emissions and auditory brain stem respose after cis-platinum exposure in gerbils. Otolaryngol Head Neck Surg 1997;116(6):585-592.
18. Sockalingam R, Freeman S, Chery L, Sohmer H. Effect of high-dose cisplatin on auditory brainstem responses and otoacoustic emissions in laboratory animals. Am J Otol 2000;21:521-527.
19. Zorowka PG, Schimitt HJ, Gutiahr P. Evoked otoacoustic emissions and pure tone threshold audiometry in patients receiving cisplatinum therapy. Int J Pediatric Otorhinolaryngol 1993;25:73-80.
1. Speech Doctor (Volunteer in the Audiology department at Hospital do Câncer from 2002 to 2005)
2. PhD (PhD in Science of Communication Disorder by UNIFESP. Speech Doctor in the Audiology Department at Hospital do Câncer)
3. Speech Doctor (Speech Doctor in the Audiology Department at Hospital do Câncer).
4. Speech Doctor (Master Student in Science at Fundação Antonio Prudente. (Speech Doctor in the Audiology Department at Hospital do Câncer).
Study done at Audiology Department at Centro de Tratamento e Pesquisa Hospital do Câncer. A.C. Camargo.
Mail address: Setor de Audiologia do Centro de Tratamento e Pesquisa Hospital do Câncer. A.C. Camargo - Rua Professor Antonio Prudente, 211 - Liberdade - São Paulo / SP - CEP 01509-010 - Phone: (5511) 2189-5123 - E-mail: mel_boni@yahoo.com.br
This article was submitted to SGP - Sistema de Gestão de Publicações (Publication Management System) from RAIO on March 28, 2006 and was approved on June 9, 2006 18:22:08.