INTRODUCTIONThe study imunnomediate disease from inner ear is basically new. It started around four decades ago, firstly in German by Lehnhart, in 1958, and then in Japan by Kikuchi, in 1959 (1,2).
In 1961, Beickert, found antibodies in histological areas of cochlea in guinea pigs (1,2).
Systemic lupus erythematosus (SLE) is an inflammatory disease, autoimmune, which shows its main alterations at the level of the smallest vascular structures and of the subjacent conjunctive tissues. It is classified by the production of antibodies against cell components. Among diseases of conjunctive tissues systemic lupus erythematosus is the greatest, for its clinical aspect and for its great amount of laboratory abnormalities, affecting multiple organs in simultaneous or consecutive manner, and this causes curiosity by different medical specialties. (3-6)
Polymorphic clinical manifestations can be observed affecting different systems: osteoarticular, muscular, subcutaneous, vascular, renal, nervous, pulmonary, gastrointestinal, dermatological (skin eruption in malar and nasal areas in butterfly-wing shape), hematological, ocular and hearing (3,4-8).
This disease affects people aging from second to fourth decades of life, especially women at reproductive age. Its etiology is still unknown and it is believed that disfunctions on T cell and polyclonal activation of cells B result in autoantibody production (3,6,9-11).
The involvement of hearing and vestibular systems is a rare complication, though well defined when observed on multisystemic autoimmune diseases such as rheumatoid arthritis, Wegener´s granulomatosis, LES and others (1).
Vascular lesions in internal hearing artery can cause isolated or associated vestibulocochlear symptoms. In about 1/3 of the cases they are not associated with vestibular symptoms, though gradual involvement of the system forwards labyrinth compensation (1,8,12).
MacCabe in 1979 (13) was the pioneer to describe the diagnosis for autoimmune sensorineural hearing loss, and also noticed the presence of altered responses at the lymphocyte migration test, supposing participation of immunological mechanisms in 17 cases of sensorineural hearing loss which present hearing improvement under corticosteroid therapy.
The target of this study was to evaluate vestibulocochlear behavior in patients with LES.
MATERIAL AND METHODS10 female patients with LES aging from 16 to 66 years were examined and sent from Ambulatório de Reumatologia do Hospital das Clínicas - Curitiba/Pr (Rheumatology Ambulatory) to Laboratório de Otoneurologia da Universidade Tuiuti - Paraná (Otoneurology LAboratory).
The research was approved by Institucional Ethics Committee, protocol number 023/2005 and authorized by a signed Free and Clear Agreement Term. Patients were submitted to the following procedures:
AnamnesisA questionnaire focusing on otoneurological symptoms and sings and, family and personal antecedents was applied.
Otorhinolaryngological EvaluationThis evaluation was done with the target of eliminating any alteration that might interfere on the exam.
Conventional threshold tonal audiometry was performed with audiometer Interacoustics AC 40, headphones TDH 39P and threshold in dB NA. After that, it was researched the determination of speech threshold (SRT- Speech Reception Threshold) and the Speech Recognition Percent Index (SRPI) in acoustically designed booth to prevent any foreign noise which might interfere in the test.
Classifications by Davis and Silvermann (14) and Silman and Silvermann (15) were applied to establish grade and type of hearing loss.
Acoustic Impedance MeasureThis procedure was performed in order to evaluate integrity of tympano-ossicular system through tympanometric curve and also through acoustic reflex research. It was used Interacoustics AZ-7 and heaphnes TDH 39P, and to result interpretation, it was applied Jerger´s criteria (16).
Vestibular EvaluationPatients were submitted to the following tests, which compose vestibular exam:
Without RecordIt was researched:
- Nystagmus and positional vertigo through Brandt and Daroff´s maneuver (17);
- Spontaneous and semi-spontaneous nystagmus with open eyes, frontal look and 30º of look deviation to right, to left, up and down.
With RecordTo perform vectoelectronistagmography (VENG), it was used a thermosensitive device, Berger, VN316 model, with three record channels. After cleaning skin of periorbitary areas using alcohol, an active electrode is attached with electrolytic paste to the lateral angle of each eye and frontal medium line, forming an isosceles triangle, which made the identification of oblique, vertical and horizontal eye movements possible. This type of VENG has enabled in obtaining more accurate measurement of slow component speed (vestibular correction) of nystagmus.
Ferrante adjustable height pendular swivel chair, a Neurograff visual stimulator, EV VEC model, and a Neurograff air otothermometer, NGR 05 model.
The following eye and labyrinth tests were performed according to PADOVAN AND PANSINI (18) and MANGABEIRA-ALBERNAZ et al. (19) criteria.
- Eye movement calibration. In this step of the exam, the evaluated clinical aspect was regularity of the line, what could make researches comparable.
- Spontaneous nystagmus (eyes open and closed) and semi-spontaneous nystagmus (eyes open) research. Occurrence, direction, inhibiting effect of eye fixation, and the value of angular speed of the maximum slow component of the nystagmus were evaluated in this record.
- Pendular tracking research to evaluate occurrence and type of curve.
- Optokinetic nystagmus research at a speed of 60º per second, at clockwise and anti clockwise rotation in horizontal direction. It was evaluated: occurrence, direction, value of angular speed of the maximum slow component at clockwise and anticlockwise rotation of the nystagmus.
- Pre and post-rotatory nystagmus research at descending pendular rotatory test, stimulating lateral, anterior and posterior semicircular ducts. In order to stimulate lateral semicircular ducts (horizontal), head was bent 30o to front direction. Next, head was bent 60o back and 45o to right, and then 60o back 45o to left, respectively to soothe anterior and posterior semicircular (vertical) ducts. It was observed: occurrence, direction, frequencies to clockwise and anti-clockwise rotation of the nystagmus.
- Research of pre and post-caloric nystagmus, performed on patients positioned with head and trunk leaned backwards at 60º, in order to properly stimulate of lateral semicircular ducts. The time spent on each ear for air irrigation at 42°C, 20°C and 10°C 80s for each of the temperatures and the responses were recorded with eyes closed and then opened in order to observe EIFO (inhibiting effect of eye fixation). In this evaluation, it was observed: direction, accurate values of VACL (value of angular speed of the maximum slow component) and the calculation of relations from directional preponderancy and labyrinth predominance of post-caloric nystagmus.
Statistical AnalysisProportional Difference Test was applied with the purpose of comparing results from caloric test (analyzing absolute and relative values) and results from vestibular exam. The level of rejection on voided hypothesis was established at 0.05% or 5%.
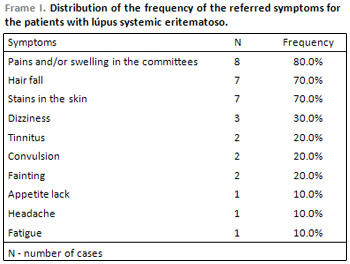
RESULTSThe main symptoms reported by patients are displayed on Frame 1. Audiological evaluation which comprehends research of tonal thresholds in frequencies from 250 to 8000 Hz, research of Speech Reception Threshold and Speech Recognition Percent Index, presented normal results in all patients.
Regarding acoustic impedance measures, we have found tympanometric curve Type A in normal condition and presence of acoustic reflex in all cases.
Results from research of positional, spontaneous and semi-spontaneous nystagmi without record, eye movement calibration, spontaneous and semi-spontaneous nystagmi with record, pendular tracking, optokinetic, pre and post rotatory nystagmi were normal.
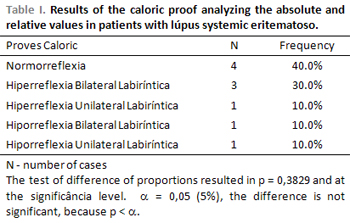
Regarding caloric test, four cases (40.0%) presented normorreflexia and six (60.0%) presented alterations. From those, three (30.0%) presented bilateral labyrinth hyperreflexia, one case (10.0%) presented unilateral labyrinth hyperreflexia, one case (10.0%) presented bilateral labyrinth hyporreflexia and one case (10.0%) unilateral labyrinth hyporreflexia, accoriding to Table 1.
According to Proportional Test, there was no expressive difference when analyzing caloric test.
We would like to point that all alterations seen in vestibular exam occurred on peripheral vestibular system.
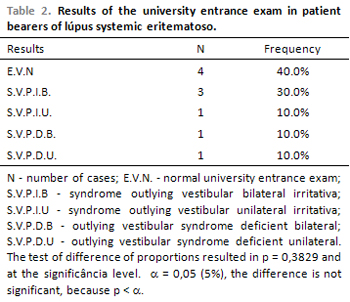
In four cases (40.0%) vestibular exam was normal, six cases (60.0%) presented peripheral vestibular syndrome; from these, three (30.0%) presented bilateral irritative peripheral vestibular syndrome, one (10.0%) presented unilateral irritative peripheral vestibular syndrom, one (10.0%) presented bilateral dificient peripheral vestibular syndrome and one (10.0%) presented unilateral dificient peripheral vestibular syndrome, accoriding Table 2.
According to Proportional Test, there was no expressive difference when analyzing results from vestibular exam.
DISCUSSIONThe most common symptoms reported by patients were: pain and/or joint swelling in eight cases (80.0%); falling of hair and skin spots in seven cases (70.0%) in each. We observed that otoneurological symptoms were hardly mentioned, such as dizziness in only three cases (30.0%) and tinnitus in two (20.0%), (chart 1). Ribeiro et al (2) examined 13 patients with LES and observed tinnitus and vertigo in five ones and aura completeness in nine ones. Sperling et al. (20) examined 84 patients and saw prevalence of aura symptom in 26 cases followed by tinnitus in 14 ones. According to authors, little reference to vestibular symptoms is due to gradual involvement of vestibular symptom causes labyrinth compensation.
In relation to prevalence of the disease in women, authors (21,22) report that more than 80.0% of the cases of LES affect them in the reproductive age. Physiological and supraphysiological concentrations of estrogen make humoral immune response easy leading to a multiplication of cells B and production of antibodies. The idea of that estrogen hormone is part of etiopathogeny of LES has its support on experimental studies with mice in which females develop condition similar to the disease, more severe and with higher auto-antibodies than in males.
We did not observe, in our study, hearing alterations in relation to audiological evaluation. We also report that hearing loss was not mentioned in the anamnesis by patients. In accordance with our findings, Atra et al. (23) researched hearing in 30 patients with LES and did not find any hearing alterations either. Authors also report that medical treatment did not change hearing. In Decoster Ferreira and Marques´ viewpoint (1), the involvement of hearing and vestibular systems is a rare complication, though it is well defined when present in multisystemic autoimmune diseases. To them, autoimmune disease of inner ear, is recognized as one the reversible causes of responsive sensorineural hearing loss when treated with immunosuppressant drug. The course of hearing loss can be bilateral, oscillating and be followed by vestibular symptoms, what it is rare, suggesting Ménière´s disease as a diagnosis. MacCabe (13) was the first to present diagnosis of sensorineural hearing loss in autoimmune disease. To authors (2,24) when hearing loss is already settled, it can develop from moderate to severe grade in few months. Audiometric curves can be descending or ascending, symmetric or asymmetric. Speech Recognition Percent Index can be unexpected, i.e. it can be altered or not. It is usually good or bad in relation to the pure tone threshold. Ribeiro et al. (2) examined 13 patients and noticed that only two of them present alteration on hearing exam. Sperling et al (20) noticed bilateral and unilateral sensorineural hearing loss in 27 patients out of the 84 who were examined.
Impedanciometry evaluation, in our study, did not present any alterations. To several authors (2,24) such evaluation can present normal tympanometric curve and presence of acoustic reflex.
In relation to labyrinth test through VENG, we could see alterations in 60.0% of patients at caloric test. We noticed that alterations on the exam occurred on peripheral vestibular system with a predominance of bilateral and unilateral irritative peripheral vestibular syndrome (40.0%) (Tables 1 and 2).
We have not found in the literature any correlation of the studied disease with vestibular exam in order to compare with our findings.
CONCLUSIONS1)Otoneurological symptoms were hardly mentioned; dizzines in 30.0% and tinnitus in 20.0% of the cases;
2)Audiological and impedanciometry exams did not present any alterations in all patients;
3)Alterations on vestibular exam occurred in 60.0% of patients, and it was found in caloric test;
4)There was a predominance of alteration of the peripheral vestibular system;
5)There was predominance of irritative peripheral vestibular syndromes. We noticed a shortage of publications in Brazil regarding the studied disease with otoneurological findings, what made the need of a more deep study on the topic. This might contribute for the recognition of the importance of the otoneurological evaluation on the immune-mediated disease of the internal ear, especially LES, as it is a topic of great interest.
REFERENCES1. Decoster DMH, Ferreira NGM, Marques MPC. Doenças auto-imune da orelha interna: uma revisão bibliográfica. Acta Awho, 2001, 20:113-6.
2. Ribeiro S, Moraes CLO, Neto GR, Silveira JAM, Gonçales F, Quintero SM. Avaliação Auditiva (audiometria tonal e emissões otoacústica evocadas - produtos de distorção) em pacientes portadores de lúpus eritematoso sistêmico e artrite reumatóide. Rev Bras Otorrinolaringol., 2002, 68:239-43.
3. Verztman L, De Paola D. Doenças difusas do tecido conjuntivo. Rio de Janeiro: Gernasa: 1972. p.201-61.
4. Verztman L, Leite N, Lederman R. Lúpus eritematoso sistêmico. In: Cruz Filho. A Clínica reumatológica. Rio de Janeiro: Guanabara Koogan: 1980. p.344-62.
5. Bomtempo CAS, Vasconcelos FPJ, Kakehasi AM, Básalo S, Brito FA, Ferreira GA, et al. Lúpus eritematoso sistêmico e mielite transversa: relato de um caso com necropsia. Rev Bras Reumatol., 2001, 41:296.
6. Verli FD, Cherubini K, Souza MAL. Lúpus eritematoso: uma abordagem estomatológica. Rev Bras Patol Oral., 2004, 3:26-31.
7. Tabosa TP, Souza BDB, Russo FFS. Lúpus eritematoso sistêmico associado a miastenia gravis: relato de caso. Rev Bras Reumatol., 2001, 41:298.
8. Cecatto SB, Garcia RID, Costa KS, Anti SMA, Longone E, Rapoport PB. Perda auditiva sensorioneural no lúpus eritematoso sistêmico: relato de três casos. Rev Bras Otorrinolaringol., 2004, 70:398-403.
9. Norris DA. Pathomechanisms of photosensitive lupus erythematosus. J Invest Dermatol., 1993, 100:585-685.
10. Petri M, Robinson C. Oral contraceptive and systemic lupus erythematosus. Arthritis Rheum., 1997, 40:797-803.
11. Yung RL. Mechanisms of lupus: the role of estrogens. Clin Exp Rheumatol., 1999, 17:271-5.
12. Andronopoulos AP, Naxakis S, Lygatsikas C. Sensorineural hearing disorders in systemic lupus erythematosus: a controlled study. Clin Exp Rheumatol., 1995, 13:137-41.
13. McCabe BF. Autoimmune sensorioneural hearing loss. Ann Otol Rhinol Laryngol., 1979, 88:585-9.
14. Davis H, Silverman RS. Hearing and deafness. 3ª ed. New York: Holt, Rinehart & Wilson: 1970. p.253-79.
15. Silman S, Silverman CA. Auditory diagnosis, principles and applications. London: Singular Publishing Group: 1991. p.215-32.
16. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol., 1970, 92:311-24.
17. Brandt T, Daroff RB. Physical therapy for benign paroxysmal positioning vertigo. Arch Otolaryngol., 1980, 106:484-5.
18. Padovan I, Pansini M. New possibilities of analysis in electronystagmography. Acta Otolaryngol., 1972, 73:121-5.
19. Mangabeira-Albernaz PL, Ganança MM, Pontes PAL. Modelo operacional do aparelho vestibular. In: Mangabeira- Albernaz PL, Ganança MM. Vertigem. 2.ed. São Paulo: Moderna: 1976. p.29-36.
20. Sperling NM, Tehrani K, Liebling A, Ginzler E. Aural symptoms and hearing loss in patients with lupus. Otolaryngol Head Neck Surg., 1998, 118:762-5.
21. Mills JA. Systemic lupus erythematosus. New Engl J Med., 1994, 330:1871-79.
22. McMurray RW, May W. Sex hormones and systemic lupus erythematosus: rewiew and meta-analysis. Arthritis Rheum., 2003, 48:2100-110.
23. Atra E, Pontes PAL, Goldenberg J, Nóbrega JL, Sato EI, Pollar DF. Estudo da audição no lúpus eritematoso disseminado. Rev Bras Reumatol., 1983, 23:203-7.
24. Cruz OLM, Costa SS, Alvarenga EL. Disacusia neurossensorial imunomediada. In: Cruz OLM, Costa SS. Otologia clínica e cirúrgica. Rio de Janeiro: Revinter: 2000. p.307-13.
1. Doctor (Coordinator of the Program for Master of Communication Disorders at the University Tuiuti of Parana).
2. Doctor (Adjunct Professor of the Program for Master of Communication Disorders at the University Tuiuti of Parana).
3. Student of the Graduate Course in Speech at the University Tuiuti do Paraná (None).
4. Specialist (Associate Professor of Clinical Medicine, Federal University of Parana).
5. Specialist (Resident of the Office of Rheumatology, Hospital de Clinicas of Curitiba / PR).
Labotatório Otoneurology of the University Tuiuti do Paraná (UTP).
Address to correspondêmcia: Bianca Simone Zeigelboim - Street Gutemberg, 99 to 9 floor - CEP 80420-030 - Curitiba / PR - Phone / Fax: (41) 3331-7807 -- E-mail: @ bianca.zeigelboim utp.br
This article was submitted in SGP - Sistema de Gestão de Publicações (Publication Management System) in the RAIO 10/4/2006 and approved on 30/5/2006 23:01:06.