INTRODUCTION Dermoid cysts are often present at birth. They are asymptomatic affecting mainly males(1). They grow in a slowly way, are unilocular, and the cyst masses can cause only few symptoms, that originate from the dimensions by its growth. They are often found in the ovary and testicles, and 7% can affect the head and neck area(2). Although the origin of those cysts is uncertain, it is believed that is associated to the remaining pluripotent embryo tissues during the first and second bronchial arches fusion in the third and fourth weeks of intrauterus life(3). Disorganized and difference growth of those "kidnapped" cells start from dermoid cyst.
Dermoid cysts can be classified into three histological types: epidermoid cyst (with no dermal annexes in its covering epithelium); dermoid (presence of skin annexes such as sweat gland cells and hair follicle) and teratoid ones (covering containing structures from the three generative layers).
When occurring in the head and neck, dermoid cysts are more common to be found in the fronto-orbital area, in the external superior forth of the orbit(4). Other sites can be the midline of the nose or neck and sublingual area.
The differential diagnosis of a retroauricular cyst should be done with the following: Epidermal inclusion cyst, Trichilemmal cyst, lipoma and hamangioma.
This study reports a case of epidermoid cyst in the retroauricular area. It is evaluated the secondary symptoms (conductive hearing loss) regarding its extension towards the interior of the external auditory meatus. Surgical removal was suggested aiming the recovery of patient's hearing ability as there was no other alteration that justified hearing loss.
CASE REPORT A 41-year-old-femaleL Caucasian patient searched for assistance complaining of hearing loss to the left side, with no otorrhea or ear pain. Symptoms arouse around 5 years ago with small retroauricular node, but no phlogistic signs, which receded gradually in two months and so did the signs and symptoms. In the following months, she noticed a progressive hypoacusis recurrence and after searching for ENT assistance was diagnosed of Cerumen impaction, which blocked the external ear meatus. She was also submitted to two warm water irrigations with no improvement of symptoms, and developed intense itching and pain. Then, she was examined (by the authors) through clinical ENT exam with an otoscope, and presented left EAC stenosis (external ear canal), which prevented the observation of the ipsilateral tympanic membrane. Tonal audiometry presented hearing threshold within normal limits to the right and mild conductive hearing loss to the let (Picture 1); immitanciometria showed curve A and bilateral stapedial reflexes. CT scan of mastoid bone with no contrast presented oval structure (Picture 2A), presence of fat, its larger axis measuring about 1.5 x 1.2cm (Picture 2B), between the soft tissues which cover the superior wall of the EAC inside, presenting a lipoma aspect. According to the diagnosis, surgical resection with complete removal of the lesion through retroauricular access and then anatomopathological exam of the surgical specimen were recommended. During surgery, it was found a 2cm diameter mass with citrine liquid (Picture 2C). This mass had uneven surface; it was soft and redish, and was placed in the posterior EAC area, extending into the mastoid bone (Picture 2D). Histopathological result was a suppurated epidermal cyst with giant-cell reaction.
Picture 1. Tonal audiometry presenting mild conductive hearing loss to the left.
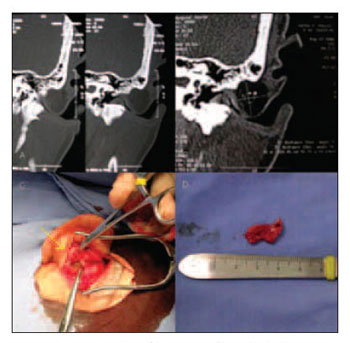
Picture 2. A, B. CT scan of the mastoid - coronal. Oval aspect with 1.5 x 1.2cm fat density between the soft tissues. CC. Retroauricular incision with auricular pinna which has been previously forced back (yellow arrow), intraoperative aspect of the citrine content. D. macroscopic content of the surgical specimen.
Patient presented clinical and audiometric improvement after surgery, and did not present recurrence up to the current date (3-month follow-up).
DISCUSSION A nodule in the ear is quite notable and should be seen by an ENT or skin doctor. It is a close, prominent, touchable, profound lesion sited on the dermis or cartilage, what can perforate by secondary cutaneous ulcer. Clinical context, precise localization, dermal and histological aspects help on diagnosing it.
Dermoid cysts on the outer ear are rare. There are three cases of retroauricular dermoid cysts(4,5) described in the literature and five ones in the Japanese literature. All of them occurring in the superior part of the ear(2).
Trichilemmal or sebaceous cysts are similar to the epidermoid one. The histopathological exam assures the diagnosis by a capsule formed by all epidermis layers and its content is composed by horny material (keratin). Lipomas are benign tumor composed by fatty tissue and can present the same aspect of the dermoid cysts. Hemangiomas are often present at birth; they are benign tumors of the vascular endothelial which can develop in spontaneous manner.
In the current report, anamnesis and physical exam showed progressive hearing loss complaint in the past 5 years and a nodule on the posterior wall of the EAC. Therefore, among all possibilities of diagnosing, excisional biopsy was chosen in order to be confirmed by the histopathological exam of the specimen. Tonal audiometry to measure hearing loss degree and CT scan to better evaluate the anatomy of the lesion and possible involvement of adjacent structures were chosen as preoperative exams. Surgical removal is the therapy for epidermoid cysts, and its localization determines surgical approach and also it should be a healing type.
For being a lesion sited on the posterior wall of the EAC by the mastoid and in order to completely ease symptoms, the current authors chose the retroauricular access for being a better accessible surgery and for providing easy identification and resection of the pathological process. It was necessary EAC packing by using Gelfoamâ and antibiotic cream in order to re-establish the skin canal, which was previously displaced by the cyst.
FINAL COMMENTS Epidermoid cyst in the retroauricular area is rare. They are not neoplasms, but actually developmental lesions. They are rare ectodermal tumors arising from benign, capsuled and slow growth fetal epiblast cells. Its growth happens due to normal esquamation cells inside a cyst cavity, causing secondary symptoms to its localization and involvement of neighbor structures. When treating it, complete removal of lesion should be carried out in order to avoid recurrences.
REFERENCES 1. De Souza BA, Dey C, Carver N: A rare case of dermoid cyst behind the ear. Plast. Reconstr. Surg. 2003; 112: 1972.
2. Ikeda M, Muto J, Omachi S: Dermoid cyst of the auricle: report of two cases. Auris Nasus Larynx 1990;16:193.
3. Freitas CEOLP, Siqueira BMS, Silva Junior AF, Botelho TL, Pereira CM: Cisto epidermóide em região submentoniana: relato de caso clínico. Rev. Bras. de Patologia Oral 2005; 4(2):90-93.
4. Samper A: Dermoid cyst on the auriculotemporal area. Plast. Reconstr. Surg. 2000; 106: 947.
5. Bauer DJ, Diwan R, Honig BK, Yokel B: Large asymptomatic mass on the ear: Dermoid cyst of the auricle. Arch. Dermathol. 1994; 130: 913.
1. 3rd year Resident doctor at Hospital dos Servidores do Estado do Rio de Janeiro.
2. Doctor at Serviço de Otorrinolaringologia do Hospital dos Servidores do Estado do Rio de Janeiro.
3. Master degree in ENT by Universidade Federal do Rio de Janeiro - PhD student at Santa Casa de São Paulo. Doctor at Serviço de Otorrinolaringologia do Hospital dos Servidores do Estado do Rio de Janeiro.
Serviço de Otorrinolaringologia do Hospital dos Servidores do Estado do Rio de Janeiro - ENT Service of Hospital dos Servidores - Rio de Janeiro - Brazil)
This article was submitted to SGP (Sistema de Gestão de Publicações - Publication Management system) of R@IO on December 27th, 2007 and approved on February 11th, 2007 at 11:48:18.

