INTRODUCTIONBefore the beginning of the antibiotic therapy age a large number of adenoids (pharyngeal tonsils) and tonsils (palatine tonsils), mainly affecting in children, were removed through surgery, with the purpose of controlling recurrent infections. Nowadays most cases of recurrent infections can be treated by making use of drugs. However, there are still some circumstances in which surgery is necessary.
The cases which are surgery-prescribed are: recurrent amygdalitis, which often affects children from five to seven times a year, in two consecutive years at least (1); peritonsillar abscess (2); halitosis due to coat in the tongue, a social factor for surgery prescription; large or hypertrophy tonsils; sleeping apnea (3); otitis media is almost always secondary to a infection of the upper aerodigestive tract (nose or pharynx) (4).
Adenoidectomy, Tonsillectomy or Adenotonsillectomy procedures have been performed for long and also have been under changes in order to reduce their complications. Bleeding the most common one (5).
Paulo de Aegina (625-690 a.C.) reported cases of tonsillectomy in his Epitome of Medicine (seven books) (6,7).
Surgery procedures and surgical tool have been constantly changing in order to reduce complications (incomplete removal of the tonsils; postoperative pain; nauseas and vomiting; respiration and deglutition difficulties). Fetid bleeding is nowadays the most common complication, and it requires postoperative revision (5,7,8).
This work has the purpose to study the profile of patients who were assisted by the Otorinolaryngology discipline at UNISA and to compare results with the literature data.
MATERIAL AND METHODSThis study was previously registered at SISNEP and later approved by the Research Ethics Committee by Universidade de Santo Amaro (nº 183/7).
It was performed an analysis of the medical reports of the patients who were submitted to surgery in the Otorhinolaryngology discipline of the Faculdade de Medicina da Universidade de Santo Amaro (UNISA), in the city of São Paulo from January/2002 to January/2003 and from January to August/2006.
Data was collected in a standardized protocol and codified into Epi-Info 6.0 program in order to have its statistical analysis.
All medical reports were analyzed during the period above mentioned. All patients who were submitted to the following surgical procedures were selected: Adenoidectomy, Tonsillectomy or Adenotonsillectomy. Patients who had simultaneous operations (with the exception of postectomy, umbilical hernia or inguinal hernia) were not included in the study.
The following data was collected: sex; age; diagnosis; surgery prescription; type of anesthesia; surgery procedure; period of hospitalization; causes of occasional postoperative revision and postoperative complications.
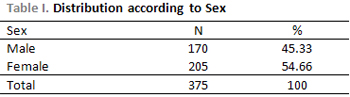
RESULTSData showed prevalence on males (54.66%) over females (45.33%).
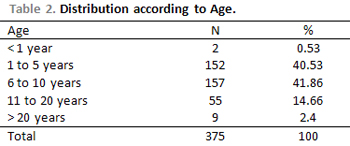
Patients aging from 6 to 10 years prevailed (41.86%) followed by patients aging from 1 to 5 years (40.53%).
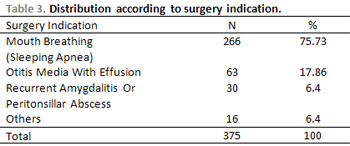
The main surgery indications referred to cases of mouth breathing (70.93%), otitis media with effusion (16.8%) and recurrent amygdalitis or peritonsillar abscess (8.0%).
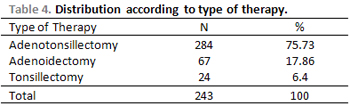
Adenotonsillectomy was performed in 75.73% of the cases; Adenoidectomy in 17.86% and Tonsillectomy in 6.4%.
The occurrence of bleeding was the only complication observed in 0.8% among all cases.
All patients were submitted to balanced general anesthesia (Propofol from 2 to 4mg/Kg in children and 2 to 3mg/Kg in adults) and airway anesthesia (Isoflurane). Midazolam (0.1mg/Kg EV) was applied as pre anesthesia drug.
All patients were submitted to mechanical dissection of the tonsillar tissue for the tonsillectomy procedures and curettage of the adenoid tissue in the cavum with Beckman curette. The Hemostasis procedure was performed with compression by making use of gaze soaked in Bismuth Subgalate. In case of bleeding during surgery, stitches were done separately with simple catgut 2.0 suture and with 2,0-cm needle. The period of hospitalization agreed with the Hospital rules, and the maximum mandatory period was six hours after surgery. Only three patients remained for more than 24 hours in hospital because they developed hemorrhage after surgery.
DISCUSSIONThe tonsils (also known as palatine tonsils) and the adenoids (known as pharyngeal tonsil) are parts of a structure called lymphatic ring of Waldeyer. This ring is found at the entrance of the upper respiratory tract, and that is why it is highly affected by a large number of infections. In addition to palatine and pharyngeal tonsils, the tubal and lingual tonsils and the lymphatic tissue also are found in the pharynx (9). They are ring-shaped and formed by a large amount of cells responsible for the production of antibodies (lymph tissue), which are the proteins involved in the organism defense against different infections (10). The function of these cells is the most important during childhood and youth, when their sizes are reduced.
The removal of the pharyngeal and/or palatine tonsils was a common procedure not long ago. This fact is easily seen among Brazilians aging between fifty and sixty, most of them were submitted to such surgery.
The surgery procedure has been highly prescribed after the studies that showed the importance of the conservation of the lymph tissue of the tonsils to a better development of children and adolescent together with the pharmacology advances in the treatment of infectious and inflammatory diseases on the nose and throat.
The target of this research was to trace the profile of patients who are assisted in a University hospital and to compare it with worldwide literature revision with the purpose of verifying occasional disagreement in our population.
According to sex, the research showed that 54.66% of the patients were male and 45.33% were female. This shows that there is no clear frequency in both sexes regarding the distribution of the researched diseases, which is confirmed by other study, performed in Brazil, reporting 52.6% in males and 47.4% in females in a year period. A similar study in the United States showed 70% in female and 30% in males (10,11).
The distribution according sex is suggested by the influence of the environment. However, it is not the aim of this study to clear its possible causes; still it is a possible topic for future researches.
The age group of the selected patients ranged between six and ten years, accounting for 41.86%. However, there was prevalence of patients aging five years (40.53%). According to the literature, the average age of patients are around eleven and twenty two (10).
The fact can be referred to the type of the population from the assisted area, where there is a lack of basic sanitation and medical care. These aspects are associated to malnutrition, which increases the number of respiratory infections, by then increasing the number of operations with the purpose of preventing future problems, such as morphological alterations.
The analysis of the results showed that most of the prescriptions (75.73%) were assigned to patients with sleeping apnea. This is a late complication of the infections on tonsils because they develop a chronic process of recurrence that leads to upper airway obstruction. Patients who are not properly treated are the main carriers of mouth breathing syndrome.
As previously mentioned, the assisted population lacks health care and this might explain the achieved percentage. The otitis media with effusion was the second prescription (16.8%). It results from the progress of the microorganisms in the auditory tube deriving from infections of the pharyngeal tonsils.
The recurrent amygdalitis or peritonsillar abscess was the third most frequent cause, disagreeing with the literature that reports them as the most frequent cause, as a result of a long treatment of patients with some immunological disorder or carriers of microorganisms resistant to antibiotic therapy. These can lead to recurrent sinusitis, recurrent otitis media, snoring and apnea (12,13).
The Adenotonsillectomy was most performed procedure (75.73%), which showed that the lymph tissue involvement is generalized around the Waldeyer's ring. This information agrees with another national study that reported 72.14% of the cases (3,13). The isolated Adenoitectomy was the second procedure (17.86%), which showed that the adenoid involvement is larger than the tonsil involvement, in an isolate manner, and that leads to more severe symptoms as oral respiration, the most operative indication. The Tonsillectomy, in an isolate manner, was performed in 6.4% of the cases, differing from the national literature that reports 0.24% of occurrences (3). The matter might be due to the fact that the University Hospital is a reference center and has a larger number of samples.
Surgical procedures were characterized for being of short duration. Most of the procedures (60.6%) ranged between sixteen and thirsty minutes. This agrees with the literature that reports an average of thirsty minutes.
Patients remained hospitalized for six hours in the University Hospital (called Hospital/Day), where the study was done. Those six hours were suitable for the end of the general anesthesia action, and if there were no complications, they could be released(14).
The bleeding process, during and after surgery, can be minimized by the investigation on personal and family bleeding background; by interruption with early use of drugs that alter either the blood coagulation or the platelet agglomeration and by previous blood coagulogram. All patients who were operated presented negative personal and family background to blood dyscrasia and normal blood coagulogram (14).
Bleeding refers to the first and most common intercurrence, ranging from 2 to 3.99% (15,16,17). The cases that need a second intervention range from 0.7% to 0.8% (15,18,19).
Cases of bleeding are more common in children under 2 years old (17,20). That is the reason why surgeries are not recommended to children aging from zero to two year (16). The three types of surgeries referred in this study presented 0.8% of postoperative bleeding, which agrees with the literature.
CONCLUSIONThe evaluation of the profile of patients who were assisted in the Othorinolaryngolofy Discipline of the Faculdade de Medicina da Universidade de Santo Amaro (UNISA) regarding Adenoidectomy, Tonsillectomy and Adenotonsillectomy follows the standards of national and international literature.
REFERENCES1. Albernaz PLM. Amidalectomia e adenoidectomia: indicações e contra-indicações. Disponível em www.brasilmedicina.com.br, acessado em 30/08/07.2. Equipe autores ABC da Saúde. Abscesso periamigdaliano. Disponível em http://abcdasaude.com.br, acessado em 30/08/04.
3. Vieira FMJ, Diniz FL, Figueiredo CRW, Luc LM - Hemorragia na adenoidectomia e/ou amigdalectomia: estudo de 359 casos. Rev Bras de Otorrinolaringol. 2003, 69(3):338- 341.
4. Equipe médica da Medgraf - S.Paulo. Tratamento da Síndrome de Apnéia do Sono tipo obstrutivo. Disponível em www.respiremelhor.com.br/medicina, acessado em 30/08/07.
5. Molina FD, Maniglia JV, Magalhães FP, Dafico SR, Rezende, RS. A eficácia do subgalato de bismuto em tonsilectomias como agente hemostático. Rev Bras de Otorrinolaringol. 2000, 66(3 pt. 1): 194-7.
6. Liu JH, Anderson KE, Willging JP, Myer CM, Shott SR, Bratcher GO, Cotton RT. Posttonsillectomy hemorrhage: what is it and what should be recorded? Arch Otolaryngol Head Neck Surg. 2001, Out, 127 (10): 1271-5.
7. Walner DL, Parker, Noah PBA, Miller, PR. MD Past and present instrument use in pediatric adenotonsillectomy Otolaryngol Head Neck Surg. 2007, 137(1):49-53.
8. Gurunluoglu R, Gurunluoglu A . Paul of Aegina: landmark in surgical progress. World J Surg. 2003, 27(1):18-25.
9. Santos RP. Amígdalas e adenoides. Disponível em http://www.unifesp.br/dotorrino/orl/info/a2.htm, acessado em 09/08/07.
10. Zakirullah. Post-tonsillectomy and adenotonsillectomy morbility & complications at District Headquarter Hospital Daggar. J Ayub Med Cool Abbottabad. 2001, 13(3):4-6.
11. Paredes P, Paul P. Evaluación de amigdalectomias y adenoidectomias realizadas em el Hospital Regional Honorio Delgado de Arequipa entre 1975 a 1994. [Tese] Arequipa, San Agustin. UNSA; 1995.
12. Otacilio e Campos. Tratado de Otorrinolaringologia. Editora Roca; 1994.
13. Diniz FMJ, Figueiredo FL, Weckx LR, Luc LM. Hemorragia na adenoidectomia e/ou amigdalectomia: estudo de 359 casos. Rev Bras de Otorrinolaringol. 2003, 69(3): 338-341.
14. Windfuhr JP MD, Chen YS MD, Remmert S MD. Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients. Otolaryngol Head Neck Surg. 2005, 132(2):281-286.
15. Kendrick D, Gibbin K. An audit of the complications of paediatric tonsillectomy, adenoidectomy and adenotonsillectomy. Clin Otolaryngol. 1993, 18 (2):115-7.
16. Crysdale WS, Russel D. Complications of tonsillectomy and adenoidectomy in 9409 children observed overnight. CMAJ. 1986, 135(10):1139-42.
17. Walker P, MBBS, FRACS, and Gillies BN. Posttonsillectomy hemorrhage rates: Are they techniquedependent? Otolaryngology-Head and Neck Surgery. 2007, 136(3):27-31.
18. Hungria H. Tratado de Otorrinolaringologia. Rio de Janeiro, RJ. 6ª ed. Guanabara Koogan; 1991.
19. Prim MP, Diego D, Jimenez JL,Yuste V, Sastre N, Rabanae I, Gavilan J. Analysis of the cause of imediate unanticipated bleeding after pediatric adenotonsillectomy. Int. J Pediatric Otoaryngol. 2003, 67(4):341-4.
20. Slovicky TA, Shapira Y, Tarasiuk A, Leiberman A. Complications of adenotonsillectomy in children with OSAS younger than 2 years of age. Int. J Pediatric Otoaryngol. 2003, 67(8):847-51.
1. Resident doctor in Otorhinolaryngology.
2. Specialist in Otorhinolaryngology (Chief of the medical residence at UNISA)
3. PhD in Otorhinolaryngology - Titled Professor (Head of the Otorhinolaryngology Department at UNISA.
4. PhD in Otorhinolaryngology (Head of the Otology of the Discipline of Otorhinolaryngology at UNISA.
5. Medicine student.
Faculdade de Medicina de Santo Amaro - UNISA
Roberto Gaia Coelho Júnior
Mail address: Al. Franca, nº 1436, Apto 13 , Cerqueira Cesar
CEP-01422-001, São Paulo, SP
Phone/Fax:3082-5301 - Email: betogaia@bol.com.br
This article was submitted to SGP (Sistema de Gestão de Publicações) of R@IO on December 18th, 2007 and approved on July 24th, 2008 at 22:59:51.