INTRODUCTIONThe mucoepidermoid carcinoma is the salivary glands most frequent malignant tumor and it affects the major and minor salivary glands (1,2). It's the most common malignant tumor in the parotid (60-70% cases) (1,2). Its origin is the epithelium of the glandular excreting duct, and it may also develop in the nasal cavity minor salivary glands, maxillary sinuses, nasopharynx, oropharynx, larynx, vocal cords, trachea, lungs and lacrimal glands (1, 3, 4).
Malignant tumor located in the nasal cavity and paranasal sinuses are extremely rare and correspond to about 3% of the head and neck neoplasms. In the United States, there is an estimate of less than one case per 100000 inhabitants (5,6). The literature mentions a few cases of nasal septum affection. Out of these cervical-facial tumors, only 10% come from the salivary glands located in the nasosinusal mucosa, and their main subtypes, in frequency order are cystic adenoid, adenocarcinoma and mucoepidermoid (5) (Table 1). In a study carried out by Calderon-Garcidueñas et al. (6), with 256 patients with nasosinusal malignant neoplasm, no case of mucoepidermoid was described in this location.
CASE REPORTA 32-year-old, female, melanodermic patient. Presented with a history of nasal obstruction, frequent fluid rhinorrhea and epistaxis in the right nasal cavity for about 2 years. She mentioned having eliminated a reddish mass from this nostril about 1 year ago during a sneezing crisis.
Upon otorhinolaryngologic exam: the right nasal cavity had a tumor mass with verrucous, rose-colored, soft aspect, bleeding upon manipulation, non-pulsating, implanted in the nasal septum, obstructing the respiratory passage.
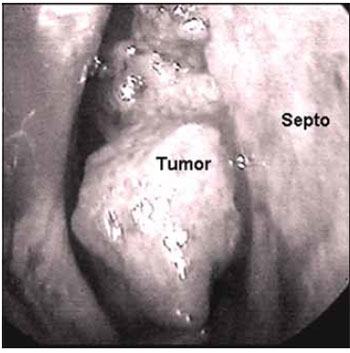
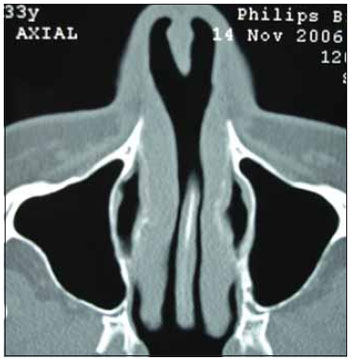
The nasofibroscopy (Picture 1) revealed a vegetating lesion originated in the nasal septum frontal region and the ground and lateral wall were preserved. Computerized Tomography of the face sinuses (Picture 2) showed affection in the right nasal septum at areas II, III and IV of Cottlè. The cervical CT revealed reactional lymph-node-megaly.

Picture 1. Mucoepidermoid Carcinoma of the Nasal Septum. Nasal Endoscopy CID: right lower infundibulum.

Picture 2. Imaging exam of the mucoepidermoid carcinoma of nasal septum. Axial tomography of the face sinuses. Pre-operative Right septum tumoration.
The tumoral biopsy revealed Mucoepidermoid Carcinoma. The tumor was classified with T1, N0, M0.
The right nasal cavity endoscopy during operation (Picture 3) revealed exiguous upper margin, that affected the septum above the retraction angle. She was submitted to surgery for the tumor exeresis, with endonasal access (Picture 4), associated with the nasal dorsum displacement. The tumor was removed in a single and wide block, including the septum cartilage and counter-lateral mucosa, which resulted in a wide perforation of the septum (Pictures 4,5) and the cartilaginous septum roof with about 0.5 mm. The safety margins were macroscopically normal, and were confirmed by freezing exam in the intraoperative.
Picture 3. Mucoepidermoid Carcinoma of the Right Nasal Septum. Endoscopic view during operation.
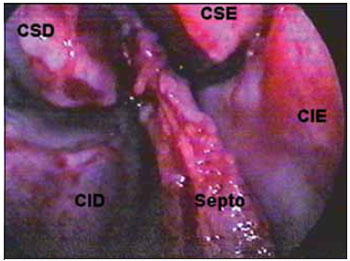
Picture 4. Septum carcinoma resection. Videoendoscopic surgical site. CID: right lower infundibulum. CIE: left lower infundibulum. CSD: right upper infundibulum. CSE: left upper infundibulum.
Picture 5. Septum carcinoma resection. Dried surgical part.
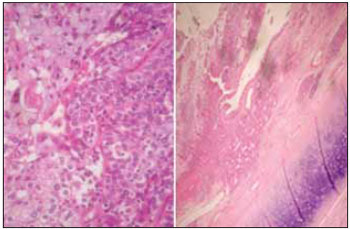
The anatomopathological exam (Picture 6) revealed high grade malignancy mucoepidermoid carcinoma (Table 2) with 1.6x1.5x0.3 cm, removed with free surgical margins. Septum cartilage without tumor infiltration.
Picture 6. Optical microscopy exam of the mucoepidermoid carcinoma of nasal septum. Microscopy (HE 200 x and 100 x).
She was forwarded to the Oncology Service for complementary radiotherapy.
Postoperative tomography shows the dry area (Pictures 7, 8). There is no sign of sealing in the nasal dorsum, even after radiotherapy.

Picture 7. Imaging exam after surgical resection. Postoperative axial tomography of the dried septum area.
Picture 8. Imaging exam after surgical resection. Postoperative sagital tomography of the dried septum area.
She is in the 3rd year of follow-up, without local, regional or remote recurrence signals.
DISCUSSIONThe mucoepidermoid carcinoma corresponds to 6 to 9% of all salivary glands tumors (3), and was found mainly in intraoral major and minor salivary glands. About 10% of the mucoepidermoid carcinoma cases occur out of the major salivary glands. The difficulty to study these unusual sites is the scarcity of studies and publications (1,3).
The nasal cavity and the paranasal sinuses are uncommon regions for malignant lesions. The main nasosinusal malignant tumor is the squamous cell carcinoma. Out of glandular tumors, the mucoepidermoid is the third in frequency, minor than the cystic adenoid and adenocarcinoma, respectively (5,6). Studies show that 0.6% of all salivary glands tumors are nasosinusal mucoepidermoid. When we consider all the mucoepidermoid tumors, 4.8% are nasosinusal (4).
The mucoepidermoid carcinoma is not frequent in the first decade of life, and has an incidence increase in young adults (3). As far as sex is concerned the studies are conflictive: some believe there is no predilection (1), others state preference for the feminine sex (60.2%) (3). As procatartic factors we include exposure to ionizing radiation, previous RT, nickel refinery, chemical solvents, leather, sawing, formaldehyde, pollution (6). The patient worked in a beauty salon with chemical stain and formol.
They appear as single mass, painlessly and of progressive and dragging growth (1,3). Generally, the tumors in the nasal cavity are found earlier than the paranasal ones, due to their symptoms (1,5). The hidden metastasis incidence is low.
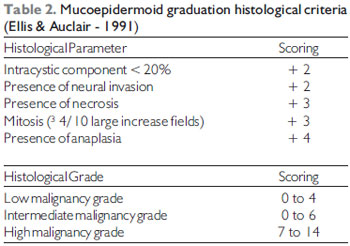
Histologically, the mucoepidermoid carcinoma is characterized by the presence of mucous, squamous and intermediate cells (with epidermoid metaplasia) (3,4). The pattern is cystic or cystic papillary (3). They may be classified into low, intermediate or high malignancy grade based on five parameters: proportion of cystic and solid elements, neural invasion presence, necrosis, anaplasia and mitotic rate (1,4) (Table 2). In spite of having been histologically classified with high malignancy grade, it clinically presented an indolent behavior.
The treatment is based on the tumor malignancy grade, tumor extension and the patient's general conditions. Wide surgical resection should be carried out, followed of post-operative radiotherapy for the intermediate and high grades, and only low grade tumors should be surgically operated (1,4). Cervical emptying should be performed in cases with regional metastases, advanced clinical staying or high histological grade (1,3). Chemotherapy has been suggested for high grade carcinomas for they have sensitivity similar to squamous cells carcinomas (3). In this case, we opted for not making excavation of the ganglions and maintained cervical CT.
The prognosis is influenced by the tumor grade, osseous invasion, absence of tumor in the surgical margins, age of 60 years or older, pain, cervical metastasis and facial paralysis. Low grade tumors allow 90% of survival within 10 years and the high grade tumors allow 42% (4).
CONCLUSIONThe nasal tumor masses must be studied with imaging exams and histopathology.
The computerized tomography reveals the limits, mass origin and exclude tumors too vascularized - nasoangiofibroma or in communication with the SNC - meningoceles, esthesioneuroblastoma. The nasal endoscopy complements the study in the identification of the tumor implantation.
The tumor biopsy may surprise with a malignant neoplasia diagnosis, and makes the surgical planning suitable to cure it.
BIBLIOGRAPHICAL REFERENCES1. Pires FR, Alves FA, Almeida OP, Kowalski LP. Carcinoma mucoepidermóide de cabeça e pescoço: estudo clínico-patológico de 173 casos. Rev Bras Otorrinolaringol. 2002, 68(5):679-84.
2. Devita VT, Hellman S, Rosenberg SA. Cancer of the Head and Neck. In: Cancer - Principles & Practice of Oncology, 5th ed. Philadelphia: Lippincott-Raven Publishers; 1997, p. 833.
3. Salazar CM, Saa J, Sánchez-Jara MR, García JL, González M. Carcinoma mucoepidermóide de vestíbulo nasal. Acta Otorrinolaring Esp. 2000, 51(7):729-32.
4. Thomas GR, Regalado JJ, McClinton M. A rare case of mucoepidermóide carcinoma of the nasal cavity. Ear Nose Throat J. 2002, 81(8):519-22.
5. Mendonça VF, Carvalho ACP, Freitas E, Boasquevisque EM. Tumores malignos da cavidade nasal: avaliação por tomografia computadorizada. Radiol Brás. 2005, 38(3):175-80.
6. Calderón-Garcidueñas L, Delgado R, Calderón-Garcidueñas A, Meneses A, Ruiz LM, Garza J, Acuna H, Villarreal-Calderón A, Raab-Traub N, Devlin R. Malignant neoplasms of the nasal cavity and paranasal sinuses: A series of 256 patients in México City and Monterrey. Is air pollution the missing link? Otolaryngol Head Neck Surg. Apr. 2000, 122:499-508.
1. Specialist in Otorhinolaryngology at ABORL-CCF Otorhinolaryngologist.
2. Specialist in ORL 3rd Year Specialization.
3. In Course for Specialization in ORL 3rd Year Specialization.
4. Specialist in Otorhinolaryngology at ABORL-CCF Preceptor of ORL Specialization in ORL of Hospital Socor - Belo Horizonte / MG.
5. Student of Medicine in the College of Barbacena - MG (4th year of graduation in medicine).
Institution: Serviço de Otorrinolaringologia e Cirurgia Cérvico-Facial do Hospital Socor Belo Horizonte - MG. BeloHorizonte / MG - Brazil.
Mail address:
Alano Nunes Barcellos
Rua Juiz de Fora, 115/1301 - Bairro: Barro Preto
Belo Horizonte / MG - Brazil - Zip code: 30180-060
Fax: (+55 31) 3832-1647
E-mail: dr_alano@yahoo.com.br
Presented as a poster in the 5th Triological Congress of Otorhinolaryngology, during the 6th through the 9th of June 2007, in Brasília / DF.
Article received on November 3, 2007.
Approved on August 23, 2008.