INTRODUCTIONThe relationship between allergy and the balance disorders has been target of several questionings and researches, specially the Ménière's Disease. In 1923, Duke was the first author to relate allergy with the Ménière's Disease, when he observed a clinical improvement of his patients with the use of epinephrine and reactivation of vestibular symptoms after tests of provocation with allergens to which they were sensitive (1). The idea was fortified in the 70's with the appearing of the autoimmunity concept in the cochleo-vestibular disorders (2). Still in the same decade, various authors described the clinical improvement of vertigo, tinnitus and hypacusis with specific therapies for inhalants and foods allergy (3, 4, 5, 6, 7). Since then, the endolymphatic sac has been recognized as a "place for immune reactions of the inner ear" (8, 9, 10), for its capacity to process antigens and produce its own immune response by antibodies. Its rich vascular fenestrated network presents selective permeability to circulation of certain substances in the inner ear, some of which considered to be antigens (11). The idea becomes attractive when high levels of circulating immunocomplexes are detected in patients with the Ménière's Disease (12, 13, 14).
Some clinical features of the Ménière's Disease are suggestive of autoimmune cause, such as the disease bilaterality, crises evolution, development of the disease in normal ear after traumatism or infection in the contralateral ear. The temporal relationship between crises of the disease and climate variations and/or contact with known inhalant allergens or food ingesta is observed (15). Recently, the prevalence of allergy in patients with Ménière's Disease was established in about 40% for inhalants and 26.6% for foods (16), a high percentage compared to the general population data, currently estimated between 25 to 30% (17) for inhalants and 5% for foods.
Although the main focus of the studies developed so far is the Ménière's Disease, the prevalence of allergy cases is not established in a population with balance disorder. Since there is a higher number of allergic patients in this population, would they carry a specific symptomatology relating to endolymphatic hydrops?
The objective of this study is to determine the prevalence of allergy in the Otoneurology service population of this hospital.
METHODThe study was approved by the Ethics Committee for Research Projects Analysis (protocol no.: 867/03) of this hospital. All patients invited to take part in the research received elucidation and signed a free and clarified authorization term.
Our sample represents a transversal cut of the Otoneurology Service, in the period from February 2004 through February 2007. The data described represent the result of a research of positive allergic tests in individuals with complaints of balance disorders. All patients with otoneurological disorders suggesting peripheral disease were included, and those with central origin balance disorder were excluded.
For the vestibular lesion topographic diagnosis, the patients were submitted to complete anamnesis, with characterization of the type of dizziness and its relationship with cochlear and/or systemic symptoms. The, we performed: full otorhinolaryngological exam, clinical research of affection of other cranial pairs and static and dynamic balance tests. As for the complementary exams, blood exams were requested (blood-count, fast blood sugar, lues sorology, lipid profile, thyroid hormones dosage, and, if necessary, blood sugar and insulinemic curve), tonal and vocal audiometry, with impedanciometry and otoneurological exam (electronistagmography). Other exams, such as electrocochleography and imaging exams, were requested according to specific clinical indication.
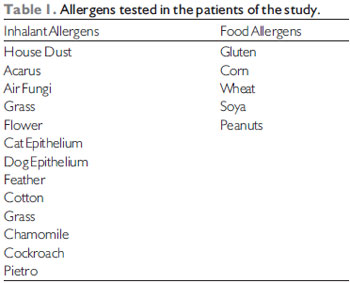
The patients were submitted to a clinical characterization questionnaire of their dizziness, tinnitus and allergy and a cutaneous test of immediate hypersensitivity (prick test) for 18 allergens as described in Table 1. As for the inhalants, the justification is that these are the most prevalent (18). The tests were carried out by the same person, and the positive response of cutaneous papule bigger or equal to three millimeters was considered.
The following variables were taken into account for the study: age, sex, clinical type of dizziness and tinnitus, in addition to the specificity of the allergen tested that produced a positive response. For statistical evaluation of the results the chi-square test and the t test for two independent samples were employed. The significance level adopted was of 5% as proposed for biological models.
RESULTS75 patients were part of the study with complaints of balance disorders of peripheral origin.
The sample presented 76% of individuals of the female sex
As for sex, there was no significance for prick test positive result (p=0.390). When the age of the patients was evaluated, we observed a significance that the prick test positive result patients tended to be younger than the non-allergic (p=0.029).
Prick TestSome patients mentioned allergic reaction or intolerance (urticaria, dysphonia, colic or diarrhea) to some foods that were not part of the battery used. Amongst which they mentioned milk, mayonnaise, cattle meat, pig meat, sausage, sardine, shrimp, oat, coffee, manioc, watercress, pineapple and mango fruit. Such foods were not tested on the prick test, and, therefore, they were not considered in the study.
In the sample studied, 25 individuals (33.3%) [IC (95%) = 22.9% to 45.2%] presented with a positive allergic test to at least one of the 13 inhalant allergens tested: house dust (88%) and mite (80%) were antigens that provoked the highest percentage of positive response, followed of cat epithelium (44%), dog epithelium (40%), cockroach (36%), feather (12%), cotton (12%), grass (12%). Then, pyrethrums, air fungi and chamomile were positive in 8% of the allergic individuals and the remaining antigens (grass and flower), in 4%
As for the food antigens tested, only 6 patients (8%) [IC (95%) = 3.0% to 16.6%] presented with a positive reaction for at least one allergen. The most frequent was corn (20%), followed of gluten (8%), soya (8%), nut (8%) and wheat (4%). All patients with positive results in food allergens also reacted to at leas one inhalant allergen.
The allergy prevalence to at least one of the antigens in our sample was of 33.3% in the total. All patients contained in this percentage reacted to at least one inhalant and 8% of whom also responded to at least one food antigen.
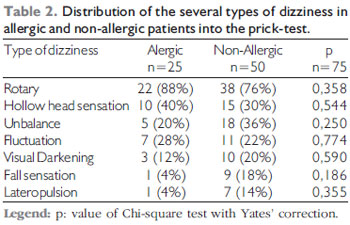
Symptoms characterizationSome of the evaluated patients had two or more types of dizziness. The 25 individuals with positive prick test were characterized clinically as for the types of dizziness they presented. Out of whom, 22 (88%) presented with rotary dizziness, 10 (40%) mentioned "hollow head", 5 (20%) unbalance, 7 (28%) floating, 3 (12%) visual darkening, 1 (4%) sensation of fall and 1 (4%) lateropulsion. In the 50 individuals with negative prick test, 38 (76%) presented with rotary dizziness, 15 (30%), "hollow head", 18 (36%) unbalance, 11 (22%) floating, 10 (20%) visual darkening, 9 (18%) falling sensation and 7 (14%) lateropulsion.
Upon comparison of both groups (allergic patients x non-allergic patients) there was no statistically significant difference as for the distribution of the different clinical picture of dizziness characterization (Table 2).
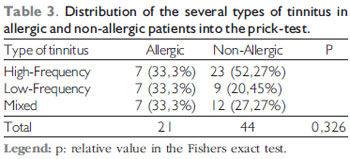
Tinnitus was present in 21 (84%) of the 25 patients with positive allergic test. Out of whom, 7 (33.3%) presented with high-frequency tinnitus, 7 (33.3%) low-frequency and 7 (33.3%) mixed tinnitus (of high and low frequencies). As for the 50 patients with negative allergic test, tinnitus was present in 44 (88%) cases, and was of high-frequency in 23 (52.27%), of low-frequency in 9 (20.45%) and mixed in 12 (27.27%). As for the presence of tinnitus, once again, there was no statistically significant difference between the allergic and non-allergic groups (p=0.326) (Table 3).
In 8 of the 21 allergic patients with tinnitus (38.1%) it appeared or was intensified during the dizziness, and the same happened with 15 out of 44 non-allergic patients with tinnitus (34.1%). Again, there was no statistically significant difference between the allergic and non-allergic groups (p=0.787).
DISCUSSIONIn this study we worked with convenience sample. The prevalence studies demand a sample size much larger than that obtained in this study, which ended up generating an wide trust interval both for food allergy prevalence and inhalants allergy.
In our sample, the prevalence of inhalants allergy (33.3%) does not seem to differ from the data of their current prevalence in the general Brazilian population, according to the last study by ISAAC, carried out in Brazil (17).
As for food allergy, the value found of 8% in our sample is much higher than that of 5% described in the general population, although both values are within IC 95% (3.0 to 16.6%), which is wide, as discussed above.
Special attention should be given to the fact the present study presents a restrict number food allergens for the prick test (only five). The patients feeding history data of our sample revealed possible allergic and/or food intolerance reactions to certain foods, whose antigenic extracts were not availed for the performance of the prick test. This could underestimate the food allergy prevalence in the population under analysis, since we considered only the patients with positive prick test for the calculation of food allergy prevalence in this study.
We must still recall that, until now, the question of precise methods for determining food allergy is largely discussed. Some authors defend the execution of a food ingesta journal for each individual, during two weeks, by instructing the patient to relate the frequency of foods swallowed with the appearing of a given symptom (inclusion / exclusion diet). In the literature, some tests in vitro are described for the determination of food allergy, such as Immunoglobulin E serum dosage specific for certain antigens, histamine liberation tests and the leukocytes cytotoxic test. However, it's important to recall that high levels of immunoglobulin or reactive leukocytes don't ensure necessarily that the disease is clinically present. Positive results must be correlated with the individual food allergy clinical history. In vivo, we mention oral provocation tests, but they are not safe for the risk of development of anaphylactic reaction (19).
Once again, it's crucial to remark that in this study only patients who presented with food allergens positive results tested with the prick test were considered to be allergic. However, a negative result at the prick test for food antigens may not exclude allergy, because the percutaneous antigenic stimulation way is different from oral stimulation, which may generate false-negative results. The golden standard to test food allergy is the oral provocation test, which, due to the risks it may cause, was not made in this study. This could change the result obtained, specially considering that some patients mentioned food reaction to some other foods that were not tested.
However, the allergy prevalence results found in the sample are far lower than those achieved by Derebery, who reports 40% of inhalants allergy and 26.6% of food allergy in patients with the Ménière's Disease (16).
Vertigo was the most common dizziness complaint in both groups; it didn't differ regarding the presence or not of allergy, and this is another information that may suggest there is no etiological relationship between allergy and peripheral vestibulopathy.
The fact the presence of tinnitus coincident with dizziness is not statistically different in the allergic and non-allergic groups is another information that may disagree with the allergy etiological association with peripheral vestibulopathy, specially when Ménière is mentioned.
CONCLUSIONIn our study, the prevalence found of inhalants allergy in the individuals with complaints of peripheral dizziness is close to the allergy prevalence in the general population. However, the food allergy prevalence values were a little higher than those found in the general population, although both values are within the IC of 95% calculated for the sample of 75 patients.
BIBLIOGRAPHICAL REFERENCES1. Duke WW. Ménière's syndrome caused by allergy. JAMA. 1923, 81(26):2179-81.
2. McCabe BF. Autoimmune Sensorineural Hearing Loss. Ann Otol Rhinol Laryngol. 1979, 88:585-89.
3. Powers WH. Allergic factors in Ménière's disease. Trans Am Acad Ophthalmol Otolaryngol. 1973, 77:22-9.
4. Pulec L, House WF. Ménière's disease study. Three years progress report. Int J Equilib Res. 1973, 3:156-65.
5. Wilson WW. Antigenic excitation in Ménière's disease. Laryngoscope. 1972, 82:1726-35.
6. Shaver Jr EF. Allergic management of Ménière's disease. Arch Otolaryngol. 1975, 101(2):96-9.
7. Endicott JN, Stucker FJ. Allergy in Ménière's disease related fluctuating hearing loss preliminary findings in a double-blind crossover clinical study. Laryngoscope. 1977, 87:1650-57.
8. Rask-Andersen H, Stahle J. Immunodefense of the inner ear? Lymphocyte-macrophage interaction in the endolymphatic sac. Acta Otolaryngol (Stockh). 1980, 89:283-94.
9. Harris JP. Immunology of the inner ear: evidence of local antibody production. Ann Otol Rhinol Laryngol. 1984, 93:157-62.
10. Tomiyama S, Harris JP. The role of the endolymphatic sac in inner ear immunity. Acta Otolaryngol. 1987, 103:182-8.
11. Altermatt HJ, Gebbers JO, Muller C, Arnold W, Laissue JA. Human endolymphatic sac: evidence for a role in inner ear immune defense. ORL J Otorhinolaryngol Relat Spec. 1990, 52:143-8.
12. Brookes GB. Circulating immune complexes in Ménière's disease. Arch Otolaryngol Head Neck Surg. 1986, 112:536-40.
13. Zhu XN, Hsu L, Zhao YS. Immunoglobulin E and circulating immune complexes in endolymphatic hydrops. Ann Otol Rhinol Laryngol. 1990, 99:535-38.
14. Derebery MJ, Srinavasa RV, Siglock TJ, Linthicum FH, Nelson RA. Ménière's disease: an immune complex-mediated illness? Laryngoscope. 1991, 101:225-9.
15. Derebery MJ. The role of allergy in Ménière's disease. Otolaryngologic Clinics of North America. 1997, 30(6):1007-17.
16. Derebery, MJ, Berliner KI. Prevalence of allergy in Ménière's disease. Otolaryngology-Head and Neck Surgery. 2000, 123(1):69-75.
17. ISAAC - The International Study of Asthma and Allergies in Childhood Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema. Lancet. 1998, 351:1223-32.
18. Lane A, Piso H, Pillsbry H. Allergy testing and immunotherapy in an academic otolaryngology practice a 20-year review. Otolaryngology Head and Neck Surgery. 2001, 124(1):9-15.
19. Gordon BR. Approaches to testing for food and chemical sensitivities. Otolaryngologic Clinics of North America. 2003, 36:917-40.
1. Otorhinolaryngologist medical doctor. In course for Post-Graduation, Doctoral Degree of the Otorhinolaryngology Discipline of the Medicine College of USP.
2. Medicine Doctoral Degree. Assistant Doctor of the Otorhinolaryngology Department Otoneurology Group of HCFMUSP.
3. Medicine Doctoral Degree Professor. Assistant Doctor of the Otorhinolaryngology Department of HCFMUSP.
Institution: Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo. São Paulo / SP - Brazil.
Mail address:
Erika Cisi Domingues - Departamento de Otorrinolaringologia da FMUSP ICHC
Avenida Enéas de Carvalho Aguiar 255, 6º andar - Sala 6021
São Paulo / SP - Brazil - Zip code: 05403-000
E-mail: erikacisi@globo.com
Article received on January 13, 2009.
Approved on February 13, 2009.