INTRODUCTIONEvidences are increasingly more consistent in the literature (1,2,3) that the gastroesophageal reflux (GER) contributes for the airways affections (mainly in children), although there isn't any direct confirmation of the cause and effect relation yet (4,5). The first difficulty in the GER disease diagnosis is to set up the individual limits to be considered between physiological and pathological GER. Another aspect to take into account is the meaning of a number of findings in the posterior region of the larynx, called posterior laryngitis (1-5).
We believe the gastroesophageal reflux is associated to a variety of laryngeal disorders, among which the laryngitis for reflux is the most frequent. The estimate is that 4.0% to 10.0% of the adults who look for otorhinolaryngological assistance have GER and about 60% to 80% of whom present signs and symptoms of laryngitis (2,6). However, this estimate doesn't apply for children (7,8).
The alterations found that are mostly suggestive of laryngitis for reflux are edema and hyperemia of vocal cords (PPVV), of interarytenoid and/or retrocricoid region, granulomas in the larynx posterior region and, in extreme cases, subglottic stenosis and laryngeal carcinoma (9,10,11).
The increase of GER prevalence and the several questions still without definitive answers regarding physiopathology, diagnosis, evolution and treatment of the extra-esophageal manifestations, compose an exhaustible research field (12,13).
It's important to emphasize that the respiratory atypical manifestations may be the first signals of the hidden gastroesophageal affection (14, 15), and nasolaryngoscopy is one of the initial propaedeutic resources for evaluation of the nasal, pharyngeal and laryngeal cavities (16, 17).
The scarcity of publications on the theme in children constituted motivation for the study that contemplates the accomplishment of naso-laryngoscopy of children submitted to esophageal pH monitoring for extra-esophageal reflux clinical manifestations.
The objective of the study is to relate the nasolaryngoscopic findings with prolonged pH esophageal monitoring in children with clinical manifestations of extra-esophageal reflux.
METHODIn this transversal prospective clinical study, we evaluated 44 children from four to 12 years old, of both genders, by means of nasolaryngoscopy.
This study was approved by the Ethics Committee in Research of UFMG and the authorization informed was obtained from all the participants' relatives.
All children were previously submitted to pH probe monitoring for research of hidden reflux due to cases of otitis, sinusitis, asthma, laryngitis and/or dysphonia in the last 12 months. The pH monitoring was performed in the Pediatric Gastroenterology Service of UFMG, by using semi-disposable pediatric probes with antimony sensor and distal esophageal pH monitoring, according to the standard procedure. The records were made for a minimum of 18 hours, while the patients exerted normal activities (18,19). The definitive diagnosis of reflux was based on a positive study of the 24-hour esophageal pH monitoring (DeMesster's Score > 14.72).
We excluded from the study patients with aerodigestive congenital malformations or who were submitted to digestive system surgery, with airways acute infection, protein allergy from cow milk, who were using oral or inhaled corticosteroid, acid gastric secretion blockers, procinetic and anti-acids within 14 days before the otorhinolaryngological evaluation.
The nasolaryngoscopy were carried out from January 2005 to April 2006 at Clínica Otomed BH. The children were placed sitting on their parents' lap in the examination chair. The vasoconstriction and nasal anesthesia were made minutes before the procedure (topical lidocaine at 2% and pediatric nasal neosinefrine spray). The endoscopies were carried out by using Machida optic fiber (3.2mm of diameter) and the images recorded in videocassette tapes (VHS) for further analysis.
Today there is no single instrument that has been validated or that is widely used in academic or private contexts (36) and the posterior laryngitis findings are currently accepted as the most common laryngoscopic signals of reflux, based on international research among otorhinolaryngologists (37).
The parameters considered in the nasolaryngoscopic evaluation were:
a) presence or absence of purulent secretion in nasal cavity;
b) adenoids volume;
c) presence or absence of interarytenoid mucosa edema;
d) presence or absence of retrocricoid region edema;
e) presence or absence of nodes in PPVV.
The data collected form individual evaluation protocols were performed using SPSS 11.0.1. For the analyses we considered the patients who had normal pH monitoring (negative) and altered (positive). The hypotheses tested considered p<0.05 to be statistically significant.
To compare the nasolaryngoscopic findings between the children groups who had normal and altered pH monitoring we employed the chi-square test (evaluation of the associations between variables) or Fisher's exact test for analysis of the categorical variables (age, sex etc.).
RESULTSThe 44 patients' mean age was of four years and 16 (36.0%) were girls and 28 (64.0%) boys. Twenty nine (66%) had an altered pH monitoring and 15 (34.0%) a normal one. Out of 29 with altered pH monitoring, 19 (65.5%) were boys and 10 (34.5%) were girls. Despite there was a discreet predominance of GER occurrence in the male population there was no statistically significant difference between the samples genders (p>0.05). Out of the 44 children six presented with purulent secretion in nasal cavity.
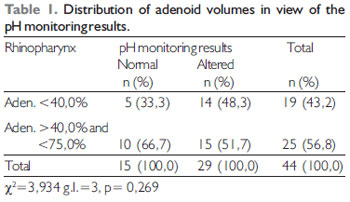
In Table 1 we may note the distribution of the adenoid volumes.
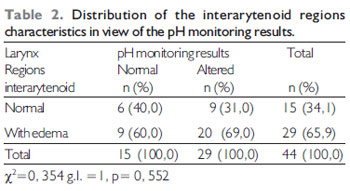
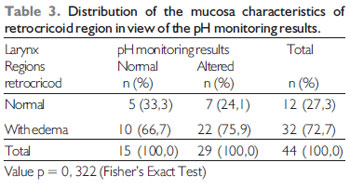
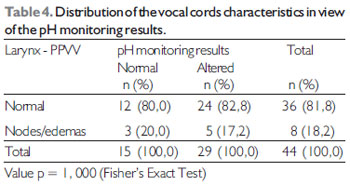
The frequency distributions of presence or absence of edema of the interarytenoid, retrocricoid regions and nodes in PPVV in view of the pH monitoring procedures are shown in Tables 2, 3 and 4.+'
There was no statistically significant difference (p>0.05) as for the parameters evaluated in the nasolaryngoscopy procedures between groups of children with normal and altered pH monitoring results. In the analysis we found at least one sign of posterior laryngitis upon nasolaryngoscopy in 15 (80.0%) children who had normal pH monitoring result and in 29 (89.7%) with altered result.
DISCUSSIONIs spite GER is a frequent and generally benignant condition in the childhood, it may relate to several respiratory affections; therefore, the awareness of the several forms of presentation of the extra-esophageal manifestations, associated with a good clinical history is very important for a GER diagnosis.
In the literature, the most frequently symptoms and affections presented by the children with hidden GER are: crises of asthma, apnea, laryngeal stridor, chronic cough, sinusitis, otitis and recurrent pneumonias etc. (3, 5, 21). Which differs from the most frequently presented by the adults that are: sensation of globus pharyngeus, chronic cough, hoarseness, persistent raucousness, thoracic pain etc. (22, 23).
The GER prevalence of 66.0% in the population studied was very significant, despite the lack of definitive laryngoscopic findings. In fact, other studies in the literature (24, 25, 26) found similar data. In addition, no matter the direction of the relationship between GER and respiratory affections, non-treated GER has many potential complications (24, 25, 26).
A Brazilian study (27) involving adults found a prevalence of 12.0% of GER among those who presented with typical symptoms of heartburn twice a week. However, this study didn't take into account the atypical manifestations, which, would probably raise such figures.
The pH monitoring of the studied patients was carried out by using only a distal sensor. Some authors considered the use of proximal or pharyngeal esophageal electrode doesn't increase the pH monitoring diagnostic power (28). Moreover, the pharynx and proximal esophagus pH monitoring results were not fully validated and yet there are controversies about the real importance in the diagnosis of patients with atypical manifestations (29).
Phipps et al. (26), used duo probe pH monitoring to evaluate 30 patients aged from two to 18 years old, with chronic sinusitis. Nineteen of whom (63%) had pathological GER in the distal esophagus and only six presented with nasopharyngeal reflux, and 15 had an improvement after clinical treatment. The clinical treatment institution consideration in all patients who had distal esophagus pH results alterations and who presented a clinical improvement reinforces the existing controversy regarding the real need and importance for use of proximal electrode.
The pH monitoring positive results between the genders didn't find any statistically significant difference, despite there had been a discreet predominance of GER occurrence in the male population. Similar data were also found in studies carried out by other authors (30, 31).
None of the 14 children evaluated had adenoids occupying more than 75.0% of the cavity of concha aerial column. In the literature reviewed, only one article (24) found higher volumes in children with additional GER diagnosis.
The prevalence of nodes in the children's vocal cords with altered pH monitoring results was of 17.2% and in those with normal pH monitoring was of 20.0%. Which contrasts with the literature involving adults that found a prevalence of 55.0% to 75.0% of nodes in the patients with GER (7,8). Such difference may be explained for the shorter time of presence of GER in the population studied.
In the literature, the percentage of posterior laryngitis findings in patients with GER are variable. Koufman et al. (23) found a prevalence of 60.0% to 82.0% of interarytenoid and retrocricoid edema in the adults examined. This association relation has been based by other scholars (32) upon the technological development of equipment that measures acidity in the proximal, distal esophagus and the pharynx (8), as well as the optic fibers, widely used in the clinical practice and that facilitated the larynx view. However, the endoscopic procedures standardization by means of protocols with the laryngeal region macroscopic characterization would be very helpful.
In the literature evaluated, the posterior laryngitis endoscopic findings didn't show any relation with the pH monitoring positive results. A study carried out by McMurray et al. (33) also didn't find a relationship between posterior laryngitis and esophagitis findings upon digestive endoscopy, when compared to the pH monitoring results. Another study (34) didn't either relate the esophagitis findings of the digestive endoscopy to the pH monitoring results.
The laryngeal alterations found in 80.0% of the children with normal pH monitoring results and in 89.7% of those with altered pH monitoring results may reflect the existence of non-acid refluxes not detected by the method, the histological characteristics of the region evaluated in this age range or even the crying normally present during the performance of nasal endoscopy.
CONCLUSIONThe result of this study alerts for the considerable prevalence of the gastroesophageal reflux in children with recurrent respiratory and/or otorhinolaryngological affections. However, in the evaluation of the GER extra-esophageal complications, the data obtained didn't show statistically significant difference (p<0.05) between the nasolaryngoscopic findings associated or not with the presence of acid GER, confirmed by pH monitoring. Therefore, it was not possible to describe the relationship between the pathological acid GER and nasolaryngoscopic alterations of children with reflux extra-esophageal manifestations. Nevertheless, the follow-up and clinical treatment of these patients could define the real importance of the GER in the physiopathology of the respiratory and otorhinolaryngological manifestations of the population evaluated.
But it's important to mention that the GER extra-esophageal manifestations still represent a challenge for doctors, patients and researchers.
BIBLIOGRAPHICAL REFERENCES1. Contencin P, Narcy P. Nasopharyngeal pH monitoring in infants and children with chronic rinopharyngitis. Int J Pediatr Otorhinolaryngol. 1995, 22(3):249-256.
2. Koufman J, Staloff R T, Toohill R. Laryngopharingeal reflux: consensus conference report J Voice .1996, 10(3):215-6.
3. Colin DR. Supraesophageal Complications of Gastroesophageal Reflux in Children: Challenges in Diagnosis and Treatment. The American Journal of Medicine. 2003, 115(3A):150-6.
4. Shepard R W, Evans J W S, Laender M et al. Gastroesophageal reflux in children. Clin Pediatric. 1987, 26:55-60.
5. Gilger MA. Pediatric otolaryngologic manifestations of gastroesophageal reflux disease. Curr Gastroenterol Rep. 2003, 5(3):247-52.
6. Shaker R. Introduction: Symposium on gastroesophageal reflux consensus reports. Am J Med. 1997, 103:1S.
7. Kalasch N et al. Dual-probe pH monitoring for assessment of gastroesophageal reflux in the course of chronic hoarseness in children. Turk J Pediatr. 2000, 42(3):186-191.
8. Katz PO. Ambulatory intragastric pH monitoring: clinical laboratory to clinical practice. Rev Gastroenterol Disord. 2003, 3(4):S3-9.
9. Kamel PL, Hanson D, Kahrilas PJ. Omeprazole for the treatment of posterior laryngitis. Am J Med. 1994,96: 321-6.
10. Fraser AG, Morton RP, Gillibrand J. Presumed laryngopharyngeal reflux: investigate or treat? J Laryngol Otol. 2000, 114:441-7.
11. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the Reflux Finding Score (RFS). Laryngoscope. 2002, 111(8):1313-7.
12. Gold BD, Freston JW. Gastroesophageal reflux in children, pathogenesis, prevalence, diagnosis, and role of proton pump inhibitors in treatment. Pediatric Drugs. 2002, 4:673-85.
13. Mccool FD. Global physilogy and pathophysyology of cough. ACCP evidence-based clinical practice guidelines. Chest. 2006, 129(1):48S-53S.
14. Waring JP et al. Childhood gastroesophageal reflux symptoms in adult patients. J Pediatr Gastroenterol Nutr. 2002, 35(3):334-8.
15. Gold BD et al. What outcome measures are needed to asses gastroesphageal reflux disease in children? What estudy design is appropriate? What new knowledge is needed? J Pediatr Gastroenterol Nutr. 2003, 37(10):S72-5.
16. Marambaia O et al. Refluxo laringofaringeano: estudo prospectivo correlacionando achados laringológicos precoces com a pH-metria de 24 horas de 02 canais. Rev Bras de Otorrinolaringologia. 2002, 68:527-531.
17. Siupsinskiene N et al. Quality of Life in Laryngopharingeal reflux Patients. Laryngoscope. 2007, 117(3):480-4.
18. Horgan P et al. Distal oesophageal pH monitoring for gastroesophageal reflux. Ir Med J. 1990, 83(4): 142-4.
19. Dobhan R, Castell DO. Prolonged intraesophageal pH monitoring with 16-hr overnight recording. Comparison with 24-hr analysis. Dig Dis Sci. 1992, 37(6):857-64.
20. DeMeester TR, Wang C, Wernly JA et al. Techinique, indications and clinical use of 24 hour esophageal pH monitoring. J Thorac Cardiovasc Surg. 1980, 79(5):656-7.
21. Mansfield L E et al. The role of the vaque nerve in airway narrowing caused by intraesophageal hydrochloric acid provocation and esophageal distencion. Ann Allergy. 1981, 47:431-4.
22. David T et al. Perspectives in Laryngopharyngeal Reflux: An international Survey. Laryngoscope. 2002, 112:1399-1406.
23. Koufman JA, Aviv J E, Casiano RR, Shaw GY. Laryngopharyngeal Reflux Position Statement of committee on speech, voice and Swallowing Disorders of the American Academy of Otolaryngology. Otolaryngol Head Neck Surg. 2002, 127:32-5.
24. Keles B, Ozturk K, Gunel E, Airbag H, Ozer B. Pharyngeal reflux in children with chronic otitis media with efusion. Acta Otolaryngol. 2004, 1249(10):1178-1181.
25. Velepic M et al. Gastroesophageal reflux allergy and cronic tubotympanic disorders in children. Int J Pediatr Otorhinolayngol. 2000, 16(55) 3:187-90.
26. Phipps CD et al. Gastroesophageal reflux contributing to chronic sinus disease in children: a prospective analysis. Arch Otolaryngol Head Neck Surg. 2000, 126(7):831-6.
27. Moraes-Filho JPP et al. Brazilian Consensus on gastroesophageal reflux disease: proposals for assessment, classification, and management. Am J Gastroenterol. 2002, 97:241-8.
28. Cucchiara S et al. Simultaneous prolonged recordings of proximal and distal intraesophageal pH in children with gastroesophageal reflux disease and respiratory symptoms. Am J Gastroenterol. 1995, 90:1791-6.
29. Noordzij JP et al. Correlation of pH probe-measured laryngopharyngeal reflux with symptoms and signs of reflux laryngitis. Laryngoscope. 2002, 112(12):2192-5.
30. Spechler SJ. Comparison of medical and Surgical Therapy for complicated gastroesophageal reflux disease in veterans. N Engl J Med. 1992, 326(12):786-792.
31. Gibbons TE, Stockwell J, Kreh R P. Population based epidemiologic survey of gastroesophageal reflux disease in hospitalized U. S. children. Gastroenterology. 2001, 120(1):154.
32. Eckley CA, Marinho V, Ruiz WS, Costa HO. O uso da pH-metria esofágica de dois canais no diagnóstico da laringite crônica por refluxo gastroesfágico. Rev Bras Otorrinolaringol. 1999, 66(2):110-4.
33. Mcmurray JS et al. Role of laryngoscopy dual pH probe monitoring and laryngeal mucosal biopsy in the diagnosis of pharyngoesophageal reflux. Ann Otol Rhinol Laryngol. 2001, 110:299-304.
34. Haggitt RC. Histopathology of reflux-induced esophageal and supraesophageal injuries. Am J Med. 2000, 108(4A):109S-11S.
35. Vandenplas Y. Reflux esophagites: biopsy or not? J Pediatr Gastroenterol Nutr. 1996, 22(3):326-7.
36. Park W, Hicks DM, Khandwala F, et al. Laryngopharyngeal reflux: prospective cohort study evaluating optimal dose of proton-pump inhibitor therapy and preditors of response. Laryngoscope. 2005, 115:1230-8.
37. Book DT, Rhee JS, Toohill RJ, et al. Perspectives in laryngopharyngeal reflux: an international survey. Laryngoscope. 2002, 112:1399-1406.
1. Master's Degree in Health Sciences, Technical Director for Otomed Clinica de Otorrino Belo Horizonte / MG.
2. Doctoral Degree in Health Sciences. Head Professor of the Pediatrics Department of UFMG.
Institution: UFMG, Departamento de Pediatria. Belo Horizonte / MG - Brazil.
Mail address:
Neide Fatima Cordeiro Oliveira
Rua dos Otoni, 881 - Sala 402 - Bairro Santa Efigênia
Belo Horizonte / MG - Brazil - Zip code: 30150-270
Telefone: (+55 31) 3273-2000
E-mail: otomed@uai.com.br
Article received on April 06 2008.
Approved on May 27 2009.