INTRODUCTIONThe peripheral facial paralysis (PFP), resulting from affection of the seventh nerve is the most common pathology of the cranial pairs. Its incidence ranges from 20 to 30 cases per 100.000 people. The appointed causes are: Viral infections such as simple herpes and herpes zoster, trauma, inflammatory affections of the middle ear, metabolic diseases and tumors.
The etiologic diagnosis of PFP is many times a challenge in the management of this pathology and in 60% to 75% the cause is idiopathic paralysis or Bell's palsy, that is thus the most frequent cause. Several studies have been presenting conflicting results as for its epidemiology. Most of which appoint the similarity as for the incidence in both sexes (1). Some state that the pathology is more frequent in young adults (2), but others find an incidence increase with the aging (1) Findings related to the season, geography and ethny have not been consistent. In the last years there has been a growing range of studies proposing that the Bell's palsy origin is the reactivation of Type 1 Simple Herpes Virus, which is latent in the geniculate ganglion.
Trauma is the second most frequent cause. The clinical or surgical treatment depends on the lesion extension. In these cases image exams are essential, in addition to electrophysiological exams to research the degree and evolution of the neuronal lesion.
The herpes zoster is latent in the geniculate ganglion and its reactivation generally originates the Ramsay Hunt Syndrome, in which the patient presents with acute facial paralysis followed by severe pain and vesicular eruptions of the external auditory meatus; only 50% of these patients recover completely (3).
The acute otitis media may be present with the facial paralysis as a complication. The incidence is higher among children, the prognosis is fortunately very favorable and there is full recovery in most cases. In the chronic otitis media, a PFP may indicate there is a cholesteatoma in the middle ear.
The Schwanomas of the 7th and 8th cranial pairs are less common causes of facial paralysis, but they must be recalled due to clinical implications they may cause. Approximately 4% of the patients with Schwanoma of the 8th cranial pair, the most frequent one, will have facial paralysis as the first signal. Therefore, the schwannoma of the 7th pair will only affect its function when in highly advanced stage (4)
The paralysis graduation is important for the clinical and postoperative follow-up. Various methods of graduation have been proposed along the years, and lately the scores of House Braxkmann and Yanagihara have been widely used. Both scores have good clinical applicability and offer few differences in the characters evaluated (3).
Based on the afference and efference functions of the facial nerves tests like: Schirmer, Stapedial Reflex, Electrogustometry and Salivary Flow are important to set up the topodiagnosis or the probable lesion place in addition to contribute for the prognosis evaluation. However, image exams such as: Computed Tomography and Magnetic Resonance are also used to compose the diagnosis.
Faced with a case of facial paralysis the electrophysiological exams are generally very important for the prognosis and the indication of some more aggressive treatments. Tests such as Hilger, Electroneurography and Electromyography are largely used everyday. Such evidences help the professional make the decision 48 hs after the beginning of the symptoms when the ischemia time has already set up the actual percentage of injured fibers (5-12).
The treatment of paralysis focuses on the basic cause therapy. In cases of Bell's palsy, the form of treatment is not fully established yet. Some studies have sought to use Antiviral Agents, Corticoids and even surgical decompression of the nerve in search of some significant result. The literature so far has been presenting very contradictory results (13-19). The emphasis is the ocular protection to prevent lesions of the cornea and conjunctiva, which are very frequent in these cases.
The objective of this work is to outline the incidence of several etiologies and the profile of patients attended with peripheral facial paralysis in the Otorhinolaryngology Service of the Medical and Biological Sciences College of the Pontifical Catholic University of São Paulo - Sorocaba Campus in 2007 and 2008. The study was approved by the Ethics Committee in Research of the Hospital Group of Sorocaba, where the patients were attended (Protocol: FR181515).
METHODWe analyzed retrospectively the records of the patients with peripheral facial paralysis attended in the otorhinolaryngology service in 2007 and 2008.
The data were obtained from the protocol of the service where they were registered: signals and symptoms, time of evolution of the disease, sex, age, side affected and etiology.
The patients were submitted to audiometric exams, Hilger, and routine Schirmer's test. The image exams, mostly in computed tomography and electroneuromyography, were carried out as necessary.
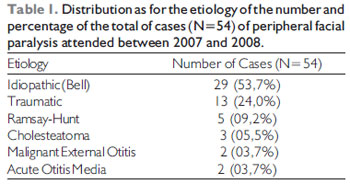
RESULTSIn the period of 2007 and 2008, 54 patients were attended, of whom the distribution of the frequencies were presented as to etiology, described in Table 1.
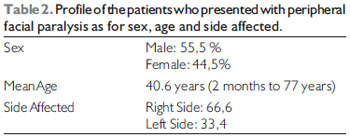
Table 2 emphasizes the results related to the patients' profile.
We also found symptoms associated in the following proportions: Paresthesia of the affected hemiface: 28 (51.85%); lacrimation increase: 36 (66,6%); otalgia: 22 (40.7%); gustative alteration: 10 (18,5%).
DISCUSSIONThe data related to the etiology draw attention because of the profile of the Otorhinolaryngology service of a tertiary hospital.
It is almost a universal consensus that the Bell's palsy, formerly considered to be idiopathic, results from a reactivation of type I herpes virus (HSV-1) (20) and, taking into account the worldwide statistics, it represents the main cause for peripheral facial paralysis. In these cases, inflammation, edema and compression of the nerve has as consequence the paralysis of their motor, secretory and sensitivity functions, depending on the area of the lesion. Fortunately it is a benign affection, since its spontaneous or assisted recovery occurs in over 96% of the cases as shown in the work by Yeo SW et all, but even so the literature reports that more than 8000 people keep motor sequels yearly in the United States of America (21). Campbell K show that the arid and cold climate may be risk conditions for the Bell's palsy (20).
Then, as shown in most part of the literature, in this series the Bell's palsy also occupies the first place as an etiology, and appears with a frequency of 53.7%. In a study with 3454 patients, Schiatkin B & May M presented results similar to ours with prevalence of Bell's palsy cases (48.3%) (22). Santos-Lasaosa et al. described a frequency much larger of idiopathic cases between 62% and 93%, probably due to the fact the study was carried out with patients attended in basic health units (23). Likewise, Steiner I et al. present a frequency of Bell's palsy between 60% and 75% of the cases of facial paralysis (24) and in a study of 38 cases Rodrigues R et al. found 73.6% of idiopathic cases (25).
Another viral etiology responsible for the PFP, resulting from Oticus Herpes Zoster, also known as Ramsay Hunt's Syndrome, is a varicella-zoster virus manifestation, which is dormant but reactivated in the extramedular ganglion (geniculate ganglion), probably during an immunity fall of the patient. It also has as aggravating factors the age, diabetes and hypertension. Opposite from Bell's palsy, the recovery prognosis is very poor and leaves permanent sequels. In a study with 2570 patients, in a period of 25 years, Peitersen shows that these patients present a more severe facial paralysis and only 21% achieve a complete recovery (26). In his 31-year series, Schiatkin B & May M found 7% of Ramsay-Hunt cases (22). In their study with 38 cases, Rodrigues R et al. Found 2 cases of Ramsay-Hunt (25).
Our study presented very similar data, with 9.2% (5 cases) with diagnosis of Ramsay-Hunt's Syndrome, taking the third frequency position.
As for other infectious causes, we find the acute otitis media, the cholesteatomatous chronic otitis media and the malignant external otitis appearing as not much frequent etiologies. In this study, we observed that out of the total of 54 cases, 12.9% involve these diagnosis distributed as 3 cases (5.5%) of CCOM, 2 cases (3.7%) of AOM and 2 cases (3.7) of malignant external otitis. In their study, Rodrigues R et al. Appoint 13.1% of infectious causes from which this study classifies as such: acute otitis media, chronic otitis media and Ramsay-Hunt's Syndrome (25), while Schiatkin B & May M indicate only 4% (22).
In addition, the traumatic facial paralysis has a fundamental importance due to its high incidence in our environment. Because it has a long intracranial way, the facial nerve favors lesions that affect its function partly or totally. The traumas may be caused by: fracture in the temporal bone, facial bones fracture, fire arm injury, facial contuse injury, birth canal and iatrogenic traumas. The lesions for trauma of the temporal bone are the most frequent cause of traumatic facial paralysis with 50% of the cases (35); they rarely section the nerve totally and the nerve mostly suffers compression of the nervous sheath. Out of these fractures, the longitudinal affection of the temporal bone has a very larger incidence and a better prognosis compared to the transverse or cominutive fractures. The lesions originated from fire arm injury more frequently reach the nerves entirely; such cause has been highly increasing the statistics mainly due to cases of aggression or attempts of suicide. Schiatkin B & May M present 23% of traumatic causes (32), Rodrigues R et al mention 7.8% of the cases of his analysis. In a study with 82 patients, Pinna BR et al describe 2 cases of iatrogenic origin (27).
Our study presents 24% of traumatic cause, and 02 cases were proven to be iatrogenic.
As for the mean age (40.6 years), the frequency on the sexes, 55.5% masculine and 44.5% feminine, this study presents results similar to those found by Ayala Mejías et al., who, in a study of 63 cases, presented the mean age of 41 years with 60% of the cases in men (28). Rodrigues R et al. also showed an incidence without statistical difference between the sexes and a stronger in the 4th decade of life (25).
Ayala Mejías et al confirmed prevalence on the left side of the face with 60% of the cases, differently from the results in which we found a predominance on the right side, with 66.6% of the cases. However, the same study emphasizes the frequency of 62% of the patients with hemiface paresthesia with a symptom associated to the case (28), similar to our data that evidenced 51.85% of the cases reporting hemiface paresthesia affected in the case acute phase. We also emphasize that our study showed an increase of lacrimation (66.6%), otalgia (40.7%) and gustative changes (18.5%) with symptoms commonly associated to the acute phase.
In our study, we witnessed one case of gradual evolution paralysis due to an occurrence of Cholesteatomatous Chronic Otitis Media. In spite it is not very common as a cause of facial paralysis, such event has already been described in other studies. In a retrospective study involving 206 surgeries of the facial nerve decompression, Testa J et al found 4.85% of the patients with cholesteatoma arising out from the facial paralysis (29).
In our work, 3 patients appeared in the service with more than 30 days of evolution of the disease, but the others appeared between 05 and 15 from the beginning of the clinical result. The late cases were not forwarded to the service in the acute phase and represent findings of exam in consultation of patients due to other complaints.
In a study between 1983 and 1992, Ramos et al. reported 12 cases of idiopathic facial paralysis in pregnant women predominantly in the 3rd pregnancy quarter (5 cases) and puerperium (4 cases) (30). In studies with 180 patients, Moraes et al. confirmed 8 cases of idiopathic facial paralysis in pregnant women, and 5 cases in the 3rd quarter of pregnancy and 3 cases on puerperium (31). Our study found 3 cases of idiopathic facial paralysis in pregnant women and 1 case in the 2nd pregnancy quarter, 1 case in the 3rd quarter and 1 case in the puerperium.
CONCLUSIONOur work presented findings similar to most part of the literature so far. The mean age of the affected was of 40.6 years with a slight prevalence of 55.5% in the male sex, a stronger incidence of affection of the right hemiface with 66.6% and with predominance of cases of Bell's palsy with 53.7% of the cases followed by the traumatic causes totalizing 24% of the patients.
BIBLIOGRAPHICAL REFERENCES1. Morgan M, Nathwant D. Facial palsy and infection: the unfolding story. Clin Infect Dis. 1992, 14:263-71.
2. De Diego JI, Prim MP, Madero R, Gavilàn J. Seasonal patterns of idiopathic facial paralysis: a 16-year study. Otolaryngol Head Neck Surg. 1999, 120:269-71.
3. Yeo SW, Lee DH, Jun BC, Chang KH, Park YS. Analysis of prognostic factors in Bell's palsy and Ramsay Hunt syndrome. Auris Nasus Larynx. 2007, 34:159-164.
4. Rosenberg SI. Natural history of acoustic neuromas. Laryngoscope. 2000,110:497-508.
5. Satoh Y, Kanzaki J, Yoshihara S. A comparison and conversion table of 'the House-Brackmann facial nerve grading system' and 'the Yanagihara grading system. Auris Nasus Larynx. 2000, 27:207-211.
6. Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical management of Bell's palsy. Laryngoscope. 1999, 109:1177-1188.
7. Thomander L, Stalberg E. Electroneurography in the prognostication of Bell's palsy. Acta Otolaryngol. 1981, 92:221-37.
8. May M, Blumenthal F, Klein SR. Acute Bell's palsy: prognostic value of evoked electromyography, maximal stimulation and other electrical tests. Am J Otol. 1983, 5:1-7.
9. Fisch U. Prognostic value of electrical tests in acute facial paralysis. Am J Otol. 1984, 5:494-8.
10. Sillman JS, Niparko JK, Lee SS, Kileny PR. Prognostic value of evoked and standard electromyography in acute facial paralysis. Otolaryngol Head Neck Surg. 1992, 107:377-81.
11. Smith IM, Maynard C, Mountain RE, Barr-Hamilton R, Armstrong M, Murray JA. The prognostic value of facial electroneurography in Bell's palsy. Clin Otolaryngol. 1994, 19:201-3.
12. Chow LC, Tam RC, Li MF. Use of electroneurography as a prognostic indicator of Bell's palsy in Chinese patients. Otol Neurotol. 2002, 23:598-601.
13. May MM, Taylor FH, Frank B. Bell's palsy: surgery based upon prognostic indicators and results. Laryngoscope. 1981, 91:2092-2105.
14. May MM, Klein SR, Taylor FH. Idiopathic (Bell's) facial palsy: natural history defies steroid or surgical treatment. Laryngoscope. 1995, 406-40.
15. Fisch U. Surgery for Bell's palsy. Arch Otolaryngol. 1981, 107:1-11.
16. Taverner D. Cortisone treatment of Bell's palsy. Lancet. 1954, 2:1052-1056.
17. Brown JS. Bell's palsy: a 5-year review of 174 consecutive cases: an attempted double blind study. Laryngoscope. 1982, 92:1369-1373.
18. Austin JR, Peskind SP, Austin SG, Rice DH. Idiopathic facial nerve paralysis: a randomized double blind controlled study of placebo versus prednisone. Laryngoscope. 1993, 103:1326-1333.
19. Allen D, & Dunn L. Acyclovir or valacyclovir for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst. 2004.
20. Campbell K. and Brundage J. Effects of Climate, Latitude, and Season on the Incidence of Bell's Palsy in the US Armed Forces, October 1997 to September 1999. American Journal of Epidemiology. 2002, 156:32-39.
21. Yeo SW, Lee DH, et al. Analysis of prognostic factors in Bell's palsy and Ramsay Hunt syndrome. Auris Nasus Larynx. 2007, 34:159-164.
22. Schiatkin B, & May M. Disorders of the facial nerve. Scott-Brown's Otolaryngology, 6th edn, Kerr AG, & Booth JB. (eds). Butterworth-Heinemann, Oxford. vol. 3, pp. 24/1-24/38.
23. Santos-Lasaosa, Pascual-Millán LF, Tejero-Juste C, Morales-Asín F. Peripheral facial paralysis: etiology, diagnosis and treatment. Rev Neurol. 2000, 30:1048-53.
24. Steiner I, Mattan Y. Bell's palsy and herpes viruses: to acyclovir or not to acyclovir? J Neurol Sci. 1999, 170:19-23.
25. Rodrigues REC, Ceccato SB, Rezende CEB, Garcia RID, Costa KS, Campilongo M, et al. Paralisia Facial Periférica: análise de 38 casos. Arq Med ABC. 2002, 27:62-66.
26. Peitersen P. Natural history of Bell's palsy. Acta Otolaryngol. 1992, 492:122-4.
27. Pinna BR, Testa RG, Fukuda Y. Estudo de paralisias faciais traumáticas: análise de casos clínicos e cirúrgicos. Rev Bras Otorrinolaringol. 2004, 70(4).
28. Ayala MA, Casqueiro SJC, Durio CE, Sanz FR. Peripheral Facial Palsy. Descriptive study at the university hospital in Getafe. Acta Otolaringol Esp. 2007, 58:52-55.
29. Testa JRG, Vicente AO, Abreu ECC, Benbassat SF, Antunes ML, Barros FA. Colesteatoma causando paralisia facial. Rev Bras Otorrinolaringol. 2003, 69(5).
30. Ramos AHC, Tanit GS, Bento RF. Paralisia facial periférica idiopática em gestantes. Rev Bras Otorrinolaringol. 1993, 59:279-280.
31. Moraes VM, Valença L, Andrade PA, Martins LMC. Paralisia facial periférica idiopática de Bell: a propósito de 180 pacientes. Arquivos de Neuro-Psiquiatria. 2001, 59:Set.
1. Graduation. Resident.
2. Doctoral Degree. Head Professor of the Otorhinolaryngology Discipline of the Medicine College of the Pontifical Catholic University of São Paulo - Sorocaba Campus.
3. Otorhinolaryngologist and Former-Resident of the Otorhinolaryngology Discipline of the Medicine College of the Pontifical Catholic University of São Paulo - Sorocaba Campus. Resident in the 4th Year of the Otorhinolaryngology Discipline of the Federal University of Uberlândia.
4. Student of the Sixth Year of the Medicine College of the Pontifical Catholic University of São Paulo - Sorocaba Campus (Academic)
Institution: Faculdade de Medicina da Pontifícia Universidade Católica de São Paulo - Campus Sorocaba. Sorocaba / SP - Brazil.
Mail address:
Nédio Atolini Junior
Rua dos Andradas, 175 - Bloco 4 - Apto. 21
Sorocaba / SP - Brazil - Zip code: 18030-175
Telephone: (+55 15) 9797-3658 / 3418-1923
E-mail: nedioat@yahoo.com.br
Article received on May 03 2009.
Accepted on May 31 2009.