INTRODUCTIONThe hearing loss interferes with the child's linguistic development, impairs its insertion in the society and produces cognitive and emotional consequences in case he or she is not inserted in an early educational program that takes into account the deafness and its particularities. The delay in the language acquisition reduces social contacts occasions and may lead to cognitive deficits, which become source of frustration for the deaf children and their parents (1).
Several authors emphasize the need for early detection and intervention as an essential factor so that the deaf children may acquire language efficiently and at the adequate age. For these authors, the first years of life are ideal for auditory stimulation because they are considered to be the neurological maturation period, a time in which the auditory capacities may be acquired more efficiently (2,3,4,5,6,7)
Moreover, the effects provoked by late intervention also influence the costs for future education of this child. Experiences in developed countries show that the cost may be three times higher when these children need special school (8). In the other hand, the hearing loss detection is still more economically feasible than the tracking of the phenylketonuria, hypothyroidism and sickle cell anemia (9).
In view of the damages caused by late detection and intervention of the deafness, in 1998 the Group of Support for Neonatal Auditory Triad (GANATU) was created. It is a non-governmental organization whose objective is to publish, normalize, operate and register the services of Universal Neonatal Auditory Triad (TANU) in Brazil (10).
In 1999, the resolution 01/99 was prepared by the Brazilian Committee on Children Auditory Losses (CBPAI). According to this resolution, "all children must be tested upon birth or at most up to 03 (three) months old and in case of confirmed auditory deficiency they must receive educational intervention until 6 (six) months." To ensure the access of most children to early intervention, the Committee recommends to evaluate them before maternity discharge (8).
According to CBPAI, the incidence of hearing loss in healthy newly-born children is estimated between 1 to 3 newborns in each 1000 births, but this value increases to about 2 to 4 % in those coming from Intensive Care Units (ICUs). Due to its high prevalence, it represents a real public health problem (9). It also has a higher prevalence when compared to diseases susceptible to triad upon the birth (8).
In 2004, the Ministry of Health organized the National Policy for Auditory Health, by means of decree GM 2073/04. This policy sets up the actions of basic attention and of medium and high complexity to be performed by the three spheres of the government (11).
Taking into account the importance of early detection and intervention of deafness for linguistic, social and cognitive development of the individuals, the high incidence of people with hearing loss, the action of the non-governmental organizations and the preparation of public policies for hearing health, the objective of this work is to characterize how this early detection and intervention process occurs in children inserted to special schools for deaf people of the city of Salvador / BA.
METHODWe evaluated the records and carried out interview with the mothers of 22 congenital deaf children. This population represented 100% of the population present in the institution that operated as research field and met the proposed inclusion criteria.
We set up as inclusion criterion: the presence of severe or deep congenital hearing loss, considering the auditory thresholds of the best ear; the age between six and eight years, an age in which all children must already have developed oral and written language; and come from homes of hearing families. The exclusion criterion was the presence of medical diagnosis that indicates neurological or neuropsychiatric pathologies as well as multiple deficiency.
We initially carried out a survey in the special schools registered with the Secretary of Education of Bahia, aiming at identifying those who had specific classrooms for the deaf population. We detected four schools: two public and two private schools.
Then we made an initial contact with each institution to clarify the objectives of this work and request the use of the place as a research field. Out of these, two schools met the inclusion criteria and agreed to take part in the study. We then requested from the legal coordinator of each institution the signature of free and clarified authorization, according to CNS 196/96 of the Ministry of Health, to authorize the performance of the research in the place.
After approval of the Ethics Committee in Research of the University of the State of Bahia, through protocol no. 603060009437, the legal representatives of each child were informed of the objective and method of the study and a free and clarified authorization signature was requested.
The data collected were about the age of the deafness suspicion; the development of language; phonoaudiological follow-up; the reports of exams made; the time in which the child had access to language in the auditory-oral and/or visual-spatial modality and if they used hearing aid (AASI). This data was supplied through interview with the mothers or legal responsible person and complimented with information from the records or registration forms of each child in the institution.
RESULTSThe data about age of deafness suspicion, beginning o educational and/or therapeutic service and beginning of use of hearing aid are described in Table 1.
The average age of the children when there was suspicion of deafness is discreetly better than those found in the researches carried out with the Brazilian population, from 1.3 years (7) and 1.5 years (5).
As for the age of these children when they were inserted in a program of educational and/or therapeutic service for the deaf population, we observe a value identical to that reported in other study with the Brazilian population (7). In a North-American research there was an average age of 1.8 years (4), 1.6 year less than in the children evaluated. Comparing to the age approved by CBPAI (8) for the beginning of therapeutic process, the delay is of 2.8 years.
Upon analysis of the use of hearing aid, we observe that less then the half of the children use the device and had a late access to it. Such values are below those found in other research, with the Brazilian population, which confirmed an average age of 3.11 years (5). When we compare with the research carried out in the North-American population, we observe an average age of 1.10 years in this population (4). For the CBPAI (8) the delay is of 3.0 years.
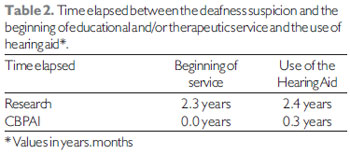
The time elapsed between the suspicion of deafness and the insertion in a specific educational program or the beginning of use of hearing aid is very long compared to that approved by CBPAI (Table 2), which may interfere considerably with the linguistic development of these children.
As for the therapeutic service profile, only 37.5% attend phonoaudiologic therapy in individual sessions with duration from 40 to 50 minutes that occurs only once a week. All children evaluated use the Brazilian signals language and only 9.1% has also oral language.
DISCUSSIONThe deaf children evaluated had a late access to language, both oral and signalized, and some do not use hearing aid or began to use it at late ages and a few have phonoaudiological therapy, being deprived of the effective contact with the language during the first years of life.
The parents generally suspect that their sons have hearing problems about the beginning of the second year of life, when the delay in the language acquisition becomes apparent. The failure to identify the children with hearing loss results in late diagnosis and intervention.
It is important to emphasize that due to the hearing sensorial deprivation, that interferes with oral language acquisition, the deaf children of hearing parents generally achieve the school age without having a systematized language and begin to acquire it only when they get into an educational program that considers their specificities. In the case of oral language, the deafness makes the access to the sound face of the language difficult and in the case of the signals language, the poor practice with this language modality by the hearing parents damages the interaction with the deaf children (12, 13, 14, 15, 16).
Despite the National Program of Hearing Health approves the use of hearing aid in the beginning of the therapeutic program until the 3 years of age (11), we know that at this age one loses the highest part of the period taken as essential so that the language develops efficiently (2,3,6,8,17). According to CBPAI, the treatment must begin preferably until the six months of life (8).
We also observe that most children were inserted in educational and/or therapeutic program even without the use of hearing aid. The late use or lack of use of a hearing aid, in turn, makes oral language acquisition difficult, because the present residual hearing ability is not enough for perception and effective discrimination of the sound information present in the environment (6,18,19,20).
Moreover, if the phonoaudiological therapy were being used by all the research individuals or in cases such session used a higher number of week hours, it could facilitate the oral language acquisition in these children. Through the use of specific strategies for the development of auditory capacities and construction of the dialogic space, the phonoaudiological therapy will create condition so that the deaf child develops the oral language (21,22,23).
It is important to emphasize that the aspects regarding the early detection and intervention were evaluated in children who are inserted in an educational and/or therapeutic program and registered in special schools. Therefore, the children who remain excluded from this process were not analyzed, which could describe results even more distant from the ideal approved by the CBPAI.
The accomplishment of the routine Universal Neonatal Auditory Triad (TANU), started since the maternities, enables the early identification of hearing loss and diminishes the effects resulting from late intervention (10). TANU has been considered the best method for early diagnosis and intervention of the hearing loss, since it comprises a large number of newborns, because it starts in the maternity, in addition to being fast and efficient. Then it is necessary that TANU's performance becomes mandatory for all children, right in the first years of life, by including the first step in all the state's maternities.
The steps following the triad, in turn, need to be carried out at specialized places. Therefore, the structuring of reference system is essential for the treatment of the children who failed in the auditory test so that all of them receive the audiologic diagnosis and are submitted to the hearing aid and phonoaudiological therapy processes. In addition, all these steps need to be carried out as soon as possible, then this reference system needs to be adequately structured so as to become efficient and meet its final objective.
According to decree GM 2073/04, we must promote the wide coverage in the service for hearing impaired in Brazil, by ensuring universality, equity, integrality and social control of the auditory health. However, this fact was not found in the population studied.
CONCLUSIONTaking into account the cost-benefit relations and the life quality of the deaf, the advantages of early detection of auditory changes are evident, as well as the population awareness about this subject.
The public health work must include in their actions the accomplishment of educative activities intended for the prevention and early detection of deafness by means of integrated actions with the several professional that deal with collective and mother and child health. The services and health professionals in articulation with the governmental organizations and the society need to operate for the implementation of public policies intended for auditory health in the children and neonatal population by enabling integral, universal and quality attention.
BIBLIOGRAPHICAL REFERENCES1. Corvera J, Gonzalez F. Psicodinamia de la Sordera. Gaceta Medica de Mexico. 2000, 136(2):139-51.
2. Carney AE, Moeller MP. Treatment Efficacy: Hearing Loss in Children. Journal of Speech and Hearing Research. 1998, 41(1):61-84.
3. Yoshinaga-Itano C. et al. Language of Early- and Later-identified Children With Hearing Loss. Pediatrics. 1998, 102(5):1161-71.
4. Moeller MP. Early Intervention and Language Development in Children Who Are Deaf and Hard of Hearing. Pediatrics. 2000, 106(3):e43.
5. Ferro L, Gonçalves I, Cieri CC. Tempo de Latência entre Suspeita, Diagnóstico e Intervenção em Crianças Portadoras de Deficiência Auditiva na Cidade de Campo Grande/MS. Jornal Brasileiro de Fonoaudiologia. 2002, 3(11):108-13.
6. Bevilacqua MC, Formigoni GM. Audiologia Educacional: Uma Opção Terapêutica para a Criança Deficiente Auditiva. 3ª ed. São Paulo: Pró-Fono; 2003.
7. Heck F, Raymann BCW. Tempo Decorrido entre a Suspeita da Surdez, a Primeira Ida ao Médico e/ou Fonoaudiólogo, o Diagnóstico e o Início da Reabilitação com Crianças Surdas. Jornal Brasileiro de Fonoaudiologia. 2003, 4(16):175-85.
8. CBPAI. Comitê Brasileiro Sobre Perdas Auditivas da Infância. Resolução 01/99. Disponível em: http://www.gatanu.org/gatanu/cbpai.php.
9. Oliveira P, Castro F, Ribeiro A. Surdez Infantil. Rev Bras Otorrinolaringol. 2002, 68(3):417-23.
10. Gatanu. Grupo de Apoio à Triagem Auditiva Neonatal. 2005. Disponível em: www.gatanu.org.
11. Ministério da Saúde. Portaria no 2073/GM em 28 de setembro de 2004. Disponível em: http://dtr2001.saude. gov.br/sas/PORTARIAS/Port2004/ GM/GM-2073.htm.
12. Trenche MCB. A Inclusão da Criança Surda no Ensino Comum. Distúrbios da Comunicação. 1998, 10(1):9-19.
13. Kyle J. Deaf Children Learning to Sign. Rev da Biblioteca Prof. Joel Martins. 2001, 2(3):27-37.
14. Lacerda CBF. O desenvolvimento do Narrar em Crianças Surdas: Focalizando as Primeiras Produções em Sinais. Revista da Sociedade Brasileira de Fonoaudiologia. 2004, 9(2):65-72.
15. Goldfeld M, Chiari BM. O Brincar na Relação entre Mães Ouvintes e seus Filhos Surdos. Pró-Fono Revista de Atualização Científica. 2005, 17(1):77-88.
16. Luz RD. Violência Psíquica e Surdez - Caminhos de um (Des) Encontro. Revista Espaço do Instituto Nacional de Educação de Surdos. 2003, 20:3-12.
17. Moret ALM, Ficker LB, Martinez MGNS. Fórum de (Re) Habilitação Auditiva / 2000: XV Encontro Internacional de Audiologia. Distúrbios da Comunicação, São Paulo. 2000, 11(2):339-348.
18. Lima MCMP, Gonçalves VMG, Quagliato EMAB. Detecção da Deficiência Auditiva por Meio da Escala de Aquisições Iniciais de Linguagem (ELM): Um Estudo Piloto. Distúrbios da Comunicação. 1998, 10(1):77-90.
19. Jacob LCB, Bevilacqua MC. Privação Sensorial da Função Auditiva. Distúrbios da Comunicação. 2001, 12(2):161-72.
20. Mello JM, et al. Estratégias de Comunicação Utilizadas por Portadores de Deficiência Auditiva Neurossensorial Moderada. Pró-Fono Revista de Atualização Científica. 2004, 16(1):111-18.
21. Balieiro CR, Ficker LB. Reabilitação Aural: A Clínica Fonoaudiológica e o Deficiente Auditivo. In: Lopes Filho O. (org.). Tratado de Fonoaudiologia. São Paulo: Roca; 1997, pp. 327-357.
22. Melo ME, Novaes BCAC. Caderno de Experiências no Processo Terapêutico de uma Criança Portadora de Deficiência Auditiva. Pró-Fono Revista de Atualização Científica. 2001, 13(2):242-48.
23. Novaes BCAC, Balieiro CR. Terapia Fonoaudiológica da Criança Surda. In: Ferreira LP, Befi-Lopes DM, Limongi SCO. Tratado de Fonoaudiologia. São Paulo: Roca; 2004, pp. 732-39.
1. Specialization in Multiprofessional Residence in Neonatology. In Course for Master's Degree in Public Health at UFBA.
2. Master's Degree in Communication Disorder. Professor at Unijorge.
Institution: Universidade do Estado da Bahia. Salvador / BA - Brazil.
Mail address:
Lavínia Santos de Carvalho
Rua Alberto Fiúza, 270 - Imbuí
Salvador / BA - Brazil - Zip code: 41720-025
Telephone: (+55 71) 3362- 3038 / 9933 6339
E-mail: lavinia.sc@gmail.com
Article received on May 26 2008.
Approved on June 12 2009.