INTRODUCTION The otoacoustic emissions (OAE) finding by KEMP in 1978 contributed largely for the early detection of the auditory deficiency. Since then, several studies were carried out and the results found in the (INHI) identification of neonatal hearing impairment were described. However, it is necessary to go on with these works, mainly in special population, such as the premature neonates.
The auditory loss in the childhood affects 1 to 3 in each 1000 births and about 2 to 4% of the neonates from (ICU) Intensive Care Units. The mean age of the diagnosis occurs at about 3 years of age (1). The neonates are considered to be premature when they are born with gestational age lower than 37 weeks and for presenting special characteristics, and they also need specific cares (2).
Due to the long period of permanence in the Neonatal Intensive Care Unit (NICU), the premature neonates are exposed to an inadequate environment of stimuli and amongst which the excessive noise. In the uterus, the fetus is protected from external noises for the joint action of the uterine wall, the amniotic liquid and also for listening only by osseous way. In the other hand, by losing uterine protection and starting airway hearing, the preterm infant remains exposed to high levels of noise in the NICU. On average, the bottom noise is a NICO of 77.4dB, and may reach noise peaks of 85.8dB in admission, emergency and shift change scenarios, and the maximum allowed by the Ministry of Health is of 55dB (2).
From the hypothesis that the transient evoked otoacoustic emissions (TEOAE) are more used, but have a large number of "failures" in the premature newborns and a number of these "would pass" the distortion product evoked otoacoustic emissions (DPOAE), as observed empirically in the clinical practice, this research aims at carrying out the TEOAE and DPOAE and compare their outcomes in a sample of premature neonates and verify the correlation of both tests.
In addition to this, the premature newborns have a number of risk indicator for hearing loss, and the scientific community needs to deepen the knowledge regarding the features of the cochlea in this population. Then the correlation between the TEOAE and DPOAE may raise new information for the accomplishment of the INHI, especially in premature neonates for they present with particularities such as a reduced size of the external auditory meatus, the high physiological noise, and the presence of risk indicators of hearing loss. Based on this, the objective of this study is to verify the correlation of the outcomes of the TEOAE and DPOAE in premature neonates.
METHOD The project of this research was submitted and approved by the Ethics Committee in Research of the Secretary of State for Health of the Federal District (SESDF). The patients who failed in the TEOAE and DPOAE were forwarded to the otorhinolaryngologist and for audiological diagnosis.
This study was carried out in the neonatology department of a public maternity clinic of high risk pregnancy reference in the city of Brasília - DF. After the babies were discharged from the NICU, they remained with their mothers in a joint lodging called intermediate bed, and in this occasion the procedure was applied only to newborns for whom the parents signed the Term of Free and Clarified Authorization.
During the period from April through August 2006, 50 premature babies were selected at random and consecutively, 23 of feminine sex and 27 of masculine sex, with the presence of one or more of the following criteria of hearing loss risk: disease or state requiring admission in the ICU for 48 hours or longer; mechanical ventilation; use of ototoxic medication.
Patients with other risk factors for hearing loss were excluded from the study because they could present with hearing loss due to factors not related to the prematurity and permanence in the NICU. Patients with nasogastric probe were excluded from the study for being susceptible to otitis media (3).
The TEOAE and DPOAE tests were carried out in both ears, with equipment Audx-plus - Bio-logic® (portable), in the 50 patients and 100 ears were tested with it. The babies remained during the exam n the cradle in postprandial sleep, beside the mothers' beds. The tests were executed in the following order: Initially the TEOAE were performed by using the protocol: "TE Screen 70% to 3/4 frequencies" with stimulus intensity at 80dB. The initially ear to be tested was selected at random. Then the DPOAE tests were performed with the protocol "Diagnostic 2kHz to 8kHz" with stimulus intensity L1=55dB and L2=65dB and F1/F2 ratio=1.22.
In the TEOAE we used the protocol "TE Screen 70% to ¾ frequencies", that tests the frequency bands of 1, 1.5, 2, 3 and 4kHz, but only the bands of the following frequencies were reviewed: 2, 3 and 4kHz as for reproducibility, the amplitude and signal/noise ratio, in line with the protocol adapted to that proposed by GATANU for INHI, namely: reproducibility above 70%, signal/noise ration above 3dB for the band of frequency of 2kHz and 6dB for bands of frequency of 3 and 4kHz.
The exams with suitable response in three frequency out of the five tested were considered to be "approved", and the exams that did not present the pattern adopted were considered to be "failure".
In the DPOAE we used the protocol "Diagnostic 2kHz to 8kHz and the frequencies were tested and reviewed: 2, 3, 4, 6 and 8kHz, in the requirements of amplitude and signal/noise ratio. Then we adopted the protocol proposed by GATANU 4, that suggests the signal/noise ratio of 6dB for the frequencies of 2 to 8kHz, but for the frequency band of 2kHz, the signal/noise ratio of 2dB was accepted. Therefore, only the frequencies with the following standard were considered to be present and reviewed: Amplitude above 10 dB, signal/noise ration above 3 dB for the band of frequency of 2kHz and 6dB for bands of frequency of 3, 4, 6 and 8kHz.
The results of both tests were compared, that is, the presence of the TEOAE and DPOAE in each ear. The criterion "approved/failure" was used with the presence of the OAE in at least three out of the five frequencies tested.
The amplitudes of the frequencies of 2, 3 and 4kHz were related between both procedures: TEOAE and DPOAE.
The data collected were transported to electronic worksheets of the program Microsoft Office Excel® 2003 and the statistical analysis was carried out in the program SPSS for Windows® version 13.0. The data descriptive analysis was made: frequency, central trend (average) and variance measures (standard deviation), presented by means of tables. Ultimately the data statistical analysis was carried out as described below: The Pearson's Chi-Square test for analysis regarding the "approved/failure" criterion of the TEOAE and the DPOAE; The Pearson's R test for analysis of the association between the dependent variables - reproducibility, amplitude and signal/noise average by frequency band in the TEOAE - and the independent variables - ear (right and left) and sex (male and female). The paired t-test for comparison of the amplitudes and the signal/ noise ratio between the bands of frequencies of 2, 3 and 4 kHz in the TEOAE and between the bands of frequencies of 2, 3, 4, 6 and 8kHz in the DPOAE. The Kappa test was applied for the correlation between the results of the TEOAEs and DPOAEs according to the "approved/ failure" criterion. And finally the Pearson correlation coefficient for relation between the amplitude averages of the frequency bands of 2, 3 and 4kHz of the TEOAEs and the DPOAEs. For all statistical tests we used a trust interval of 95% (error ? = 0.05).
RESULTS We studied 50 premature newborns, 23 girls (46 ears) and 27 boys (54 ears), a total o 100 ears. The mean age was of 34 weeks (d.p. 2.42 weeks). All were suitable to the gestational age (GA) with average weight of 1920.23g (d.p. 429,95g)
Out of 100 ears tested, 71 were passed: 34 right ears and 37 left ears in the TEOAEs. Despite the left ear has a major number of failures, this difference was not significant (p= 0.509). Out of 46 female ears, 36 passed and 10 failed for the TEOAEs and out of 54 male ears, 35 passed and 19 failed, but this difference was not significant either (p=0.140).
There was no statistically significant difference between the male and female genders nor between the right and the left ears, regarding the variables: amplitude, reproducibility and signal/noise ratio in the frequencies reviewed in the TEOAE, thus the outcomes were analyzed jointly.
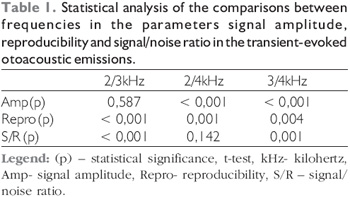
As for the amplitude in the TEOAE, we verify that despite the frequency band of 3kHz presents a higher average, there was no significant difference with the frequency band of 2kHz (p=0.587). However, with the frequency band of 4kHz we verified a significant difference (Table 1). In the reproducibility study we observed a higher average in the frequency of 3kHz, in the statistical analysis we verified a significant difference with the frequency bands averages of 2kHz and 4kHz (Table 1). In the signal/noise ratio analysis, the highest average also occurred in the frequency of 3kHz, with a significant difference between the frequency bands averages of 2kHz and 4kHz (Table 1).
Out of 100 ears tested, 97 passed, 48 right ears and 49 left ears in the DPOAEs. In the gender comparison we verified? 45 female participants passed and only one failed and out of the male participants, 52 passed and 2 failed. There was no significant difference between the right and left ears (p=0.558) nor male and female genders (p= 0.655) as for the approved/failed parameter. Then, in the amplitude and signal/noise ratio review of the DPOAEs, the male and female genders and the right and left ears were grouped.
The analysis of amplitude per frequency band in the DPOAEs showed that the highest averages occurred in the frequency of 2kHz and 8kHz respectively (Table 2). In the statistical analysis between the frequencies we may observe there was no significant difference between the amplitude averages of the frequency bands of 2kHz and 8kHz (p= 0.140). The frequency bands of 3kHz and 4kHz did not either present significant difference (p= 0.129). In the other frequency bands we verified significant differences between the averages (Table 2).
The outcomes of the DPOAEs signal/noise ratio showed a gradual increase of the signal/noise ratio average value with increase of frequency. The statistical analysis (Table 2) confirmed that only between the frequency bands of 2kHz and 3kHz no significant difference was verified (p= 0.481).
A significant correlation was confirmed between the TEOAEs and the DPOAEs in the "approved/failure" criterion (p= 0.006). The, out of the 100 ears: 97 passed the DPOAEs, out of which 71 also passed the TEOAEs and all that passed the TEOAEs also passed the DPOAEs. Out of 29 ears that failed the TEOAEs only 3 failed the DPOAEs, and out of 71 that passed the TEOAEs, no one failed the DPOAEs.
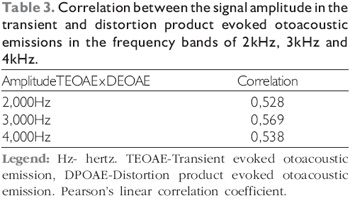
In the correlation between the TEOAEs and the DPOAEs amplitudes in the frequency bands of 2, 3 and 4kHz, we observed an important correlation between all the frequency bands in both types of EOAE (Table 3).
DISCUSSION According to the scientific literature researched the INHI may be carried out both by the TEOAEs and the DPOAEs, but as for the population of premature infants, no specific studies were found with correlation of both types of OAE. The results of this study suggest that for the premature newborns, the performance of the DPOAEs in the INHI programs may be used, since there is a good correlation with the TEOAEs. Because the DPOAEs presented less noise interference, whether physiologically or environmentally of the newborns, there is a lower number of failures, which was also verified in this study.
In this study, we verified that 71% of the neonates had present TEOAE, and such data are close to those of other researches (5,6). However, JARDIM (7) found values higher than those in this study. By evaluating 70 neonates coming from NICU, about 87.1% passed the TEOAE test, but the patients were not separated by the presence or absence of risk factor for hearing impairment, as described in this research.
The results of this study do not indicate significant difference between ears, genders and the outcomes from the TEOAEs concerning the "approve/failure" criterion, which confirmed other studies (5,6,8,9).
However, some studies showed differences related to parameters of amplitude, reproducibility and signal/noise ratio and between genders, like those by KEI and col.(8) who presented a better performance of TEOAE responses related to the reproducibility, amplitude and signal/noise ratio in the female gender and in the right ear. Similar results were found by AIDAN and col. (10) in 1164 neonates' ears evaluated. In the study by, THORNTON, MAROTTA and KENNEDY (11) they also found a better response in the female gender and the right ear in the 14.328 female gender ears and 14.070 ears in the male gender ears evaluated. SAITOH and col. (12) upon researching 332 neonates also verified better responses on amplitude, signal/noise and reproducibility in the right ear and in the female gender. DURANTE and col. (13) carried out a national study of TANU with 1000 neonates and reported higher responses of TEOAE in the right ear and the female gender. It is worth standing out that this difference was confirmed in studies with a higher number of participants and suggests anatomic differences between genders with the possibility of occurring a higher quantity of external hair cells in the female gender's cochlea and factors related to the efferent activity of the right ear. Therefore, we may infer that this study did not find any significant difference between genders and between ears possibly because of the number of participants.
The frequency band of 3kHz presented on average a better response in the three parameters analyzed, in the average of amplitude, reproducibility and signal/noise ratio in the TEOAE. It is worth remarking that despite the frequency band of 3kHz presents a performance better than the others, upon the execution of the statistical analysis between frequencies, there was no significant difference between the averages of the frequency band amplitude of 3kHz and 2kHz. The fact that the frequency band of 3kHz has response values higher than the other frequencies on average is opposed to our studies (8,9,13,14,15) KORRES and col. (16), upon studying the TEOAEs in two groups of neonates tested with different protocols, reported a higher average of signal/noise ratio and reproducibility in the frequency of 3kHz in both groups. According to HALL (17), ULHÔA (18) and SPERI (15) such characteristic must be ascribed to the influence of the spontaneous OAEs in this frequency band.
As for the use of the DPOAE in the INHI, GORGA and col. (19) report that the DPOAEs are suitable for it is a safe, non-invasive test that can be performed in hospital environments, such as maternity clinics and NICU where there is some environmental noise. In the scientific literature we may observe a growing interest in the studies of the DPOAEs in the INHI, mainly for the frequency specificity (19, 20, 21, 22, 23, 24, 25).
In the sample studied, 100 ears of premature neonates, we observed the presence of DPOAE in 97 ears.
The high presence of DPOAE was also found in studies such as that by GORGA and col. (19) with 2348 healthy neonates, 4478 from NICU and 353 with some risk factor, who found 2.4% of "failure", that is, 97.6% "passed" the DPOAE and most of those who "failed" had craniofacial malformations. BORGES and col. (25), upon performance of INHI in a sample of 200 neonates, observed only 1 patient with altered DPOAE, who was born prematurely and with low weight. In the statistical analysis no significant difference was observed between genders and the side of the ears; this finding was also verified in other researches (19, 20, 22).
The highest amplitude average of the DPOAE was found in the frequency band of 2kHz. Upon performance of the comparison by frequency band, no statistically significant difference was observed between the amplitude averages of the frequency bands of 2kHz and 8kHz. Studies such as by SOARES (26), RAINERI and col. (22) and AZEVEDO (27) also found a higher amplitude average in the frequency band of 2kHz. GORGA and col. (19) found a higher amplitude average around the frequencies of 1.5kHz to 2kHz, which confirms the outcomes of this study.
Another parameter analyzed in the DPOAEs was the signal/noise ratio, in which a growing increase was observed towards the high frequency bands. However, there was no statistically significant difference in the comparison of the frequency bands averages of 2kHz and 3kHz. The gradual increase in the signal/noise ratio according to the increase of the frequency is also consistent in the literature and reveals that the higher the frequency the less the physiological and environmental noises interfere with the capturing and register of the DPOAEs (17, 19, 22, 23, 25, 26, 27). GORGA and col. (19) also reported the possibility of the cochlea apex producing less DPOAEs than the cochlea base, and that in the frequencies following 1kHz the middle ear transmission is worse. In the same study the authors compared the outcomes from the DPOAEs with the region in which the exams were carried out: room without acoustic treatment and room with acoustic treatment. They did not verify any significant difference in the signal/noise ratio according to the place of performance of the exam, and suggested the physiological noise of the neonates are the main factor to influence the increase of the signal/noise ratio with the increase of the frequency.
In the comparison between the TEOAEs and the DPOAEs a significant correlation could be confirmed between the tests, which demonstrates the reliability on both types of EOAEs for performance of the INHI in premature neonates. While 71% of the 100 ears tested passed the TEOAEs, 97% of them passed the DPOAEs and the 3% that failed the DPOAEs were within those that failed the TEOAEs. Other studies also observed an agreement between both types of EOAEs with full-term neonates, such as LONSBURY-MARTIN, WHITEHEADA, and MARTIN (28), LOPES-FILHO and col. (29). No comparative studies were found between TEOAEs and DPOAEs with preterm neonates prior to ours.
The fact that "failure" occurs more in the TEOAEs than in the DPOAEs may be explained by the difference between the obtainment technique and the frequencies that were tested in each of the tests. In the TEOAEs, the protocol used tested the frequencies of 1kHz to 4kHz and the DPOAEs protocol tested the frequencies of 2kHz to 8kHz. In the scientific literature researched and the findings of this study, we verify that the low frequencies are more influenced by physiologic and environmental noises (17,19). Therefore, one method supplements another. While the TEOAEs evaluate the low frequency bands, the DPOAEs allow for an evaluation of the frequency band above 4kHz.
NORTON and col. (30) carried out an auditory selection in 4911 newborns, including healthy neonates, neonates admitted in the NICU and neonates with at least one risk factor for hearing loss. They used the three methods indicated by the AAP (American Association of Pediatrics), that is TEOAEs, DPOAEs and AEPs (Encephalic Trunk Audition Evoked Potentials). They found a similar outcome in the methods for hearing loss diagnosis. They state there is no perfect method, since each one has its limitations and ones complement the others.
Despite the techniques for obtainment of the TEOAEs and DPOAEs are different (31, 17), since the TEOAEs stimulate the cochlea as a whole, by means of a brief stimulus (click), the DPOAEs stimulate the specific parts of the cochlea according to the pure tones presented, a sound correlation was observed between the amplitudes of frequency bands of 2, 3 and 4kHz in the sample studied. These data agree with the studies by GRANJEIRO and col. (32) carried out with adults and BALATSOURAS and col. (33) with children aged from 9 to 12 year old, both studies observed a significant correlation between the frequency bands in both types of EOAEs. However no works with premature neonates that correlate the frequency band of the TEOAEs and DPOAEs were found in the scientific literature. Therefore, we verified a need for more studies concerning the fact.
CONCLUSION Based on this work, we may conclude that the correlation between the TEOAEs and DPOAEs results was significant. The TEOAEs were present in 71% of the sample. The frequency band of 3kHz presents a better performance on average in the parameters: reproducibility, amplitude and signal/noise ratio. The DPOAEs were observed in 97% of the 100 ears tested and had a higher average amplitude in the frequency of 2kHz. The signal/ noise ratio values increased on average gradually in the high frequencies. The use of the DPOAEs may be an alternative for diminishing the rate of "failure" in the INHI of premature neonates when compared to the TEOAEs in maternity clinics.
BIBLIOGRAPHICAL REFERENCES 1. Comitê Brasileiro sobre Perdas Auditivas na Infância (CBPAI) - Recomendação 01/99. J do CFFa. 2000, 5:3-7.
2. Ministério da Saúde-Atenção humanizada ao recémnascido de baixo peso - Método Mãe Canguru. In: Manual do Curso. Brasília; 2001 p.204-208.
3. Job A, Nottet JB. DPOAEs in young normal-hearing subjects with histories of otitis media: evidence of sub-clinical impairments. Hearing Research. 2002, 167:28-32.
4. Grupo de Apoio a triagem Auditiva Neonatal Universal (GATANU). [online] 2006 [capturado em: 15 de novembro de 2006] Disponível em: www.gatanu.org
5. Stevens JC, Webb HD, Hutchinson J, Buffin JT, Smith MF. Click Evoked Otoacoutic Emissions in Neontal Screening. A preliminary Analysis of an 8 years study. In: Grandori F, Collet L, Kemp D, Salomon G, Schorn K, Thornton R, editors. Advances in otoacousstic emissions. Vol1 - Fundamental and Clinical Application. New York; 2001. p.123-30.
6. Garcia CFD, Isaac ML, Oliveira JAA. Emissão otoacústica evocada transitória: instrumento para detecção precoce de alterações auditivas em recém-nascidos a termo e pré-termo. Rev. Bras. Otorrinolaringol. 2002, 68(3):344-52.
7. Jardim IS. Emissões otoacústicas evocadas por estímulos transientes e potencial evocado auditivo de tronco encefálico automático na triagem auditiva neonatal. [dissertação] São Paulo (SP): Faculdade de Medicina, Universidade de São Paulo; 2006.
8. Kei J, McPherson B, Smyth V, Latham S, Loscher J. Transient evoked otoacoustic emissions in infants: effects of gender, ear asymmetry and activity status. Audiol. 1996, 36(2):61-71.
9. Almeida VF. Emissões otoacústicas evocadas (EOAE) em recém-nascidos a termo. Comparação dos resultados antes e durante a amamentação - Critério de referência para uso
clínico [tese]. Brasília (DF): Faculdade de Ciências da Saúde. Universidade de Brasília; 2004.
10. Aidan D, Leastang P, Avan P, Bonfis P. Characteristics of transient-evoked otoacoustic emissions (TEOEs) in neonates. Acta Otolaryngol (Stockh). 1997, 117:25-30.
11. Thornton RD, Marotta N, Kennedy CR. The order of testing effect in otoacoustic emissions and its consequences for sex and ear differences in neonates. Hearing Research. 2003, 184:123-30.
12. Saitoh Y, Sakoda T, Hazama M, Funakoshi H, Ikeda H, Shibano A et al. Transient evoked otoacoustic emissions in newborn infants: Effects of ear asymmetry, gender, and age. J Otolaryngol. 2006, 3(2):133-8.
13. Durante AS, Carvallo, RMM, Costa FS, Soares JC. Características das emissões otoacústicas por transientes em programa de triagem auditiva neonatal. Pró-Fono R. Atual. Cient. 2005, 17(2):133-9.
14. Bassetto MCA, Chiari BM, Azevedo MF. Emissões otoacústicas evocadas transientes (EOAET): amplitude de respostas em recém-nascidos a termo e pré-termo. Rev. Bras. Otorrinolaringol. 2003, 69(1):84-92.
15. Speri MRB. Estudo sobre as emissões otoacústicas espontâneas e evocadas por estímulos transientes em recémnascidos a termo e sem risco para perda auditiva [tese]. Brasília (DF): Faculdade de Ciências da Saúde. Universidade de Brasília; 2004.
16. Korres SG, Balatsouras DG, Nikolopoulos T, Korres GS, Economou NC, Ferekidis E. The effect of the number of averaged responses on the measurement of transiently evoked otoacoustic emissions in newborns. Intern J Pediatr Otorhinolaryngol. 2006, 70:429-33.
17. Hall JW. Handbook of Otoacustic Emmissions. San Diego: Singular Publishing Group; 2000. 635 p.
18. Ulhôa MF. Emissões otoacústicas espontâneas e evocadas por estímulo transiente em crianças de até 9 meses de idade com risco para perda auditiva [dissertação]. São Paulo (SP): Pontifica Universidade Católica de São Paulo; 2002.
19. Gorga MP, Norton SJ, Sininger YS, Cone-Wesson B, Folsom RC, Vohr BR et al. Identification of neonatal hearing impairment: distortion product otoacoustic emissions during the perinatal period. Ear and Hearing. 2000. 21(5):400-24.
20. Lopes Filho O, Carlos R, Thomé D, Eckley C. Emissões otoacústicas transitórias e produtos de distorção na avaliação
de recém-nascidos com poucas horas de vida. Rev. Bras. Otorrinilaringol. 1996, 62(3):220-8.
21. Vallejo JC, Soares E, Chiriboga LM. Análise do Padrão de Respostas em Neonatos Normais para Emissões Otoacusticas Evocadas por Produto de Distorção. Rev Bras Otorrinolaringol. 1998, 64(3):251-4.
22. Raineri GG, Coube CZV, Costa Filho AO, Avarenga KF. Emissões otoacústicas evocadas produto de distorção em neonatos audiologicamente normais. Rev. Bras. Otorrinolaringol. 2001, 67(5):644-8.
23. Menezes PL, Soares A, Albuquerque RRC, Moraes MFT. Emissões Otoacústicas Produto de distorção: um estudo da função coclear. J Bras Fonoaudiol. 2002, 3(11):104-7.
24. Johnson JL, White KR, Widen JE, Grave JS, Vohr BR, James M et al. A multisite study to examine the efficacy of the otoacoustic emission/automated auditory brainstem response newborn hearing screening protocol: introduction and overview of the study. Am J Audiol. 2005, 14:178-85.
25. Borges CAB, Moreira LMO, Pena GM, Fernandes FR, Borges BCB, Otani BH. Triagem auditiva neonatal universal. Arq. Intern. Otorrinolaringol. 2006, 10(1):28-34.
26. Soares E. Emissões otoacústicas evocadas em neonatos saudáveis: critérios de referência para uso clínico [dissertação]. São Paulo (SP): Universidade Federal de São Paulo; 2000.
27. Azevedo MF. Emissões otoacústicas. In: Figueredo MS, org. Conhecimentos essenciais para entender bem emissões otoacústicas e bera. São José dos Campos: Pulso; 2003. p.35-83.
28. Lonsbury-Martin BL, Whiteheada ML, Martin GK. Clinical aplications of otoacoustic emissions. J Speech and Hearing Research. 1991, 34:964-81.
29. Lopes Filho O, Carlos R, Thomé D, Eckley C. Emissões otoacústicas transitórias e produtos de distorção na avaliação de recém-nascidos com poucas horas de vida. Rev. Bras. Otorrinilaringol. 1996, 62(3):220-8.
30. Norton SJ, Gorga MP, Widen JE, Folsom RC, Sininger Y, Cone-Wesson B, et al. Identification of neonatal hearing impairment: evaluation of transient evoked otoacoustic emission, distortion product otoacoustic emission, and auditory brainstem response test performance. Ear Hear. 2000, 21(5):508-28.
31. Kemp DT. Otoacoustic emissions in perspective. In: Robinette MS, Glattke TJ, editors. Otoacoustic emissions - clinical applications. New York: Thieme; 1997 p.1-21.
32. Granjeiro R, Kehrle H, Bezerra R, Almeida V, Sampaio A, Oliveira C. Transient and distortion product evoked otoacoustic emissions in normal hearing patients with and without tinnitus. Otolaryngology - Head and Neck Surgery. 2008, 138 (4):502-506.
33. Balatsouras DG, Keberos A, Kloutsos G, Economou NC, Sakellariadis V, Fassolis A, Korres SG. Correlation of transiently evoked to distortion-product otoacoustic emission measures in healthy children. Intern. J Ped. Otorhinolaryngol. 2006, 70:89-93.
1. Master's Degree in Health Sciences - University of Brasília - Professor of Audiology at UNIP.
2. Doctoral Degree in Health Sciences - University of Brasília - Phonoaudiologist of Hospital Santa Luzia.
3. Ph.D University of Minnesota - USA - Head Professor of the Otorhinolaryngology Discipline of UnB.
4. Doctoral Degree in Health Science - Doctor of the Cochlear Implant Sector of the University Hospital of Brasília.
Institution: Serviço de Otorrinolaringologia Hospital Universitário de Brasília Universidade de Brasília. Brasília / DF - Brazil. Mail Address: André L. L. Sampaio - SQN 205 - Bloco B - Apto. 506 - Asa Norte - Brasília / DF - Brazil - Zip code: 70843-020 - Telephone: (+55 61) 3443-3397 - E-mail: andremarjy@uol.com.br
Article received on September 13 2009. Accepted on September 21 2009.