INTRODUCTION The osteoma is a benign mesenchymal osteoblastic tumor composed by a well differentiated mature osseous tissue with a laminar structure predominance and of slow growth (8, 21). The osteomas in the regions of head and neck are localized mainly in the frontal ethmoidal region. Its location in the temporal bone is uncommon (1, 2, 3, 7, 11, 13, 16, 18, 19, 26). When localized in the mastoid region or temporal bone squama it provokes cosmetic deformities and manifests by a tumoration or as an auricular protrusion (6).
Its diagnosis is through clinical and imaging exam, but its confirmation is made by the histopathological exam. Its treatment is surgical and with excellent curative results.
The authors present two cases of mastoid osteoma and discuss its clinical picture, complimentary exams, differential diagnosis, treatment and results.
CASES REPORT Case 1
FSR. A 12-year-old male student. Tumoration in the head for one year. He denies local traumatism. Physical exam: Osseous consistency tumoration located in the right mastoid region, with 2 cm x 1.5 cm at its largest dimensions (Picture 1A), painless to superficial and deep palpation. Absence of inflammatory signals. Neurological exam: normal. Radiographic exam in lateral position, cranium profile: Radiolucent lesion localized in the right mastoid region without commitment of the inner table of the temporal bone (Picture 1B). Cranial computed tomography (CCT): Hyperdense lesion in the right mastoid region without commitment of the adjacent intracranial structures (Picture 1C). Submitted to total exeresis of the lesion under general anesthesia (Picture 1D,E). Result of the anatomopathological exam: osteoma. Medical discharge with excellent curative and esthetic result.
Case 2
JCS. 19-year-old female maid. Mentions a stone in her head for two years. She denies local traumatism. Physical exam: Tumoration located in the right mastoid region, with about 2cm x 3cm at its largest dimensions, osseous consistency, painless to superficial and deep palpation. Absence of inflammatory signals. Neurological exam: normal. Cranial simple X-ray: Presence of hyperdense lesion in the right mastoid region. Cranial computed tomography: Hyperdense lesion in the right mastoid region without involvement of the diploe and the inner table of the cranium (Pic. 2A,B,C). Submitted to exeresis of the lesion under general anesthesia. Histopathological result: osteoma. Was discharged in good state. Excellent esthetic result.
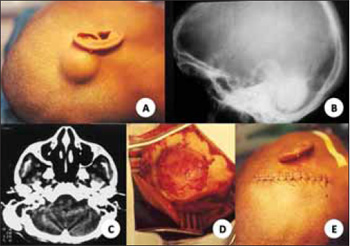
Picture 1. (A) Tumoration of osseous consistency in the right mastoid; (B) View upon radiographic exam, cranium profile; CCT in axial cut; (D) Surgical approach; (E) Immediate postoperative.
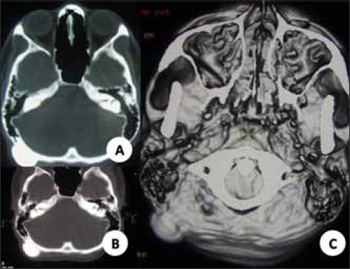
Picture 2. CCT in axial cut (A; B) and reconstruction in 3D (C).
Osteoma is a benign mesenchymal osteoblastic tumor with a normal osseous architecture and prone to grow from the outer table of the cranium, jaw and paranasal sinuses (5). It is generally an incidental finding. Its occurrence is of 0.1% to 1% of all benign tumors of the cranial cap (22,25). The mastoid osteoma etiology includes trauma, previous surgery, radiotherapy, chronic infection and hormonal factors with dysfunction in the hypophyseal gland (1,11). The osteomas are reported in all portions of the temporal bone, including squama, mastoid, internal and external auditory meatus, glenoid cavity, middle ear, Eustachian tube, petrous apex and styloid process (2, 7, 9, 26). DENIA and col (6) reported that the extracanalicular osteomas of the temporal bone locate mainly in the mastoid portion.
The osteoma is mainly composed of the mature bone and histologically presents a dense lamina organized with canals of Havers. The intertrabecular stroma contains osteoblasts, fibroblasts and giant cells (12). There are several degrees of osteoblastic and osteoclastic activity (12). There are histologically three types of osteoma: Compact, spongiotic and mixed (11, 12, 27).
Upon macroscopic exam, it presents a zone of well defined homogeneous hyperostosis with characteristics of dense lamellar bone growing outwards without producing mass effect with infiltration or alteration of the bone marrow space. Upon optical microscopy exam, it presents as a sclerotic, lamellar and dense bone, similar to the bone's cortical (10, 17).
They have slow growth and remain stable for some years (11, 12). When in the squamous or mastoid portion of the temporal bone, they may present esthetic deformities, such as external tumoration and auricular protrusion (12). Generally, the skin is not involved. The mastoid osteomas are clinically asymptomatic, which is the case of our patients. Pain upon external compression may be mentioned for the neck, auricle or middle ear (12). When there is obstruction of the meatus, it develops a diminishing of the auditory conduction and chronic suppuration (20, 24). Our cases present with tumoration in the mastoid region and painless with superficial and deep palpation.
It has a differential diagnosis with osteosarcoma, osteoblastic metastasis, isolated eosinophilic granuloma, ossifying fibroma, Paget's disease, giant cells tumor, osteoid osteoma, hemangioma, calcified meningioma, monostotic fibrous dysplasia (10, 12, 15, 17, 19). The edges of such lesions are generally less evident than the osteomas. They are generally distinguished by imaging exams associated to the anatomopathological study (10).
The osteomas are easily identified in the cranium radiographic exam as a radiolucent area with a central zone of calcification that expands outwards the original bone and the diploe is generally preserved (14, 15, 27). Computed tomography (CT) is the key-exam for its diagnosis, an osseous window and a tridimensional reconstruction may be carried out for a better anatomic localization, size, probable lesions associated and surgical planning. The osteoma presents as a low opacity and well delimited osseous tissue, involved by a sclerotic area of high opacity. In the osseous cintilography, the osteoma presents as an area of hypercaptation for a probable increase of the local metabolism (4). The magnetic resonance (MR) is excellent to view the inflammatory tissue around the lesion (17, 23). At T1 it is hypointense and at T2 the sign intensity ranges with the histological subtype (27).
The mastoid osteoma treatment is surgical resection, followed by cranioplasty in cases of extensive osseous failures (19). Its surgical indication depends upon several factors and amongst which the extension volume, symptomatology and complications. When small and asymptomatic they are submitted to conservative treatment, clinically monitored and followed up with tomography, and in cases of constant pain, neurological symptoms and extension to adjacent structure or esthetic alterations, the surgical approach is indicated. According to GUÉRIN and col (11) the early surgical intervention has been indicated to prevent voluminous growth and possible risk of complications in the surgical procedure. Our patients were submitted to total exeresis of the lesion, with excellent esthetic and curative results.
Their prognosis has been considered to be good in a esthetic and curative point of view when submitted to surgical exeresis. Recurrence is uncommon and malignant transformation has not been reported in the medical literature (6, 20).
BIBLIOGRAPHICAL REFERENCES 1. Birrell JF. Osteoma of the mastoid. J R Coll Surg Edinb. 1978, 23:305-309.
2. Burton DM, Gonzalez C. Mastoid osteomas. Ear Nose Throat J. 1991, 70:161-162.
3. Carvalho RWF, Antunes AA, Melo MRT, Andrade ESS, Pereira CU. Osteoma craniofacial: Estudo de 35 casos. Rev Bras Cir Cabeça Pescoço. 2008, 37:212-214.
4. Chang CH, Piatt ED, Thomas KE, Watne AL. Bone abnormalities in Gardener's syndrome. Am J Roentgenol Radium Ther Nucl Med. 1968, 103:645-652.
5. de Chalain T, Tan B. Ivory osteoma of the craniofacial skeleton. J Craniofac Surg. 2003, 14:729-735.
6.Denia A, Perez F, Canalis RR, Graham MD. Extracanalicular osteomas of the temporal bone. Arch Otolaryngol. 1979, 105:706-709.
7. D'Ottvai LR, Piccirillo E, De Sanctis S, Cenqua N. Mastoid osteomas: review of the literature and presentation of two clinical cases. Acta Otorrinolaringol Ital. 1997, 17:136-139.
8. Fechner RE, Mills SE. Osseous lesions. In: Fechner RE, Mills SE (eds). Atlas of tumor pathology. Tumors of the bone and joints. 3 rd series. Fascicle 8. Washington DC: Armed Forces Institute of Pathology. 1993, pp. 26-8.
9. Gil Tutor E. Osteoma of the mastoid. Case report. An Otorrinolaringol Ibero Am. 1991, 18:325-330.
10. Greenspan A. Benign bone-forming lesions: osteoma, osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal Radiol. 1993, 22:485-500.
11. Guérin N, Chauveau E, Julien M, Dumont JM, Meignarques E. Osteoma of the mastoid bone: report of two cases. Laryngol Otol Rhinol. 1996, 117:127-132.
12. Güngör A, Cincik H, Poyrazoglu E, Saglam O, Candan H. Mastoid osteomas: report of two cases. Otol Neurootol. 2004, 25:95-97.
13. Gupta OP, Samant HC. Osteoma of the mastoid. Laryngoscope. 1972, 82:172-176.
14. Izci Y. Management of the large cranial osteoma: Experience with 13 adults patients. Acta Neurochir (Wien). 2005, 147:1151-1155.
15. Kieffer AS, Long DM, Chou NS, King GA, Cacayorin ED. Tumors of the skull. In: Youmans JR (ed). Neurological Surgery. Philadelphia. WB Saunders, 1990, pp: 3599-601.
16. Magliulo G, Pullice G. Mastoid osteoma. Case report. An Otorrinolaringol Ibero Am. 2005, 32:271-278.
17. Metha JS, Shur MM, Penney CC. Unusual radiological appearance of a skull osteoma. Brit J Neurosurg. 1999, 13:332-334.
18. Morais Pérez D, Bernat Gilli A, Ayerbe Torrero V, Fernández Gómez J, Oncins Torres R. Osteoma of the mastoid. Case report. Acta Otorrinolaringol Esp. 1990, 41:343-346.
19. Pereira CU, Leão JDBC, Silva AD, Sousa PRM, Soares WGP, Santos MBO. Osteoma craniano. Considerações sobre oito casos. Arq Bras Neurocir. 2000, 19:170-173.
20. Probst LE, Shankar L, Fox R. Osteoma the mastoid bone. J Otolaryngol. 1991, 20:228-230.
21. Schajowicz F. Bone-forming tumors. In: Schajowicz F (ed) Tumors and tumor like lesions of bone. Pathology, radiology and treatment. 2 ed. Berlin: Springer-Verlag; 1994. pp. 29-140.
22. Schartz CW. Cranial osteomas from a roentgenologic viewpoint. Am J Roentgenol. 1940, 44:188-196.
23. Shibata Y, Matsumura A, Yoshii Y, Nose T. Osteomas of the skull: comparison of magnetic resonance imaging and histological findings. Neurol MedicoChirurg. 1995, 35:13-16.
24. Singh I, Sanasam JC, Bhatia PL, Singh LS. Giant osteoma of the mastoid. Ear Nose Throat J. 1979, 58:243-245.
25. Smud D, Augustin G, Kekez T, Kurda E, Majerovicc M, Jelincicz Z. Gardner's syndrome: Genetic testing and colonoscopy are indicated in adolescent and young adults with cranial osteomas. A case report. World J Gastroenterol. 2007, 13:3900-3903.
26. Van Dellen JR. A mastoid osteoma causing intracranial complications: a case report. S Afr Med J. 1977, 51:597-598.
27. Willatt JMG, Quaghebeur G. Calvarial masses of infants and children. A radiological approach. Clin Radiol. 2004, 59:474-486.
1. Doctor. Assistant Doctor Professor of the Medical Department of the Federal University of Sergipe - UFS.
2. Graduate. Resident in Surgery and Buco-Maxilo-Facial Traumatology at the School Hospital Oswaldo Cruz, of University of Pernambuco.
3. In Graduation Course Academic in Medicine of the Federal University of Sergipe.
Institution: Universidade Federal de Sergipe. Aracajú / SE - Brazil. Mail Address: Carlos Umberto Pereira - Avenida Augusto Maynard, 245/404 - Bairro: São José - Aracaju / SE - Brazil - Zip code: 49015-380 - Telephone: (+ 55 81) 8810-0954 - E-mail: wathson@ig.com.br
Article received on July 2 2009. Approved on July 12 2009.

