INTRODUCTION The Otoneurology is the science that studies the auditory and vestibular system, its expansion and relations with the central nervous system. To maintain the balance needed multiple peripheral and central systems, beyond the end organs and nerves labyrinth (1).
Vertigo is the most common symptom of a vestibular dysfunction, while their most frequent signs are the spontaneous nystagmus (SN) and voluntary eye movements and abnormal (2).
The otoneurological is accomplished through a set of procedures which includes medical history, ENT examination, audiologic and vestibular (1).
In assessing vestibular eye movements are recorded through tests such as electronystagmography (ENG). It is based on the uptake of corneal-retinal potential, environmental influences likely to suffer physiological and pathological conditions (3).
The vectonystagmography (VENG) is the improvement of ENG in which two channels were added, allowing for improved characterization of eye movements, especially the nystagmus and is still able to assess most of the supranuclear ocular motor systems and record the movements Eye on the various tests that are part of the assessment battery vestibular-ocular (4, 5).
By means of specific methods associated with computer records of nystagmus was possible to obtain greater precision and comparing the intensity of the different stimuli received in the various tests and assessments, better visualization of nystagmus and effective data archiving (6).
During the frontal fixation of gaze nystagmus can occur both eyes open and eyes closed, what is called the NE. In normal patients may experience the onset of horizontal nystagmus with closed eyes VACL less than or equal to 6o/s (7).
The presence of NE, together with complaints related to balance is a sign of pathological vestibular disorder (8), and for other authors, even without complaints, the presence of this may indicate problems in the functioning of the vestibular system (9).
The NE can modify the degree of the results of rotational chair testing (PRPD) and caloric test, directional preponderance causing the same side of nystagmus (10), and cause directional asymmetry than the limit of the normal pattern of post-caloric nystagmus (11).
In cases with abnormalities of post-caloric nystagmus in caloric tests in air at 42 and 18o C, it was found that stimulation by cold (10o C), the influence of NE may be withdrawn in most cases, showing that through this we can identify abnormalities that are not observed and further confirmed unilateral vestibular hyporeflexia (12).
Thus, the study of spontaneous nystagmus with eyes closed (NEOF) becomes relevant since it can modify the results obtained during some evidence of vestibular (10, 12), leading to wrong conclusions from it. Studies have shown that the presence of eye movement, even in the absence of complaints may indicate vestibular problems, besides being the most frequent sign in vestibular disorders and for the evaluation of this system. Moreover, the scarcity of specific research on the subject in literature, especially in our community, motivated us to assess how the NE influences the assessment of patients with chronic peripheral.
This study aimed to characterize patients and type of influence NEOF in tests of digital VENG in patients with chronic peripheral vestibular dysfunction.
METHOD It was a retrospective study that relied on survey charts of patients who underwent the test with a digital VENG, in the years 2000 to 2007, with approval of the Ethics Committee of this institution (protocol number 1562/07).
To select the sample, were analyzed tests of vestibular function with caloric vectonystagmography digital air (both Neurograff Eletromedicina Ind. e Com - EPT - Brazil).
We included subjects aged from 18 years, regardless of gender, presence of NEOF and caloric test, complete with hot and cold stimulation, with complaints of chronic dizziness of peripheral origin.
From this sample, those who showed abnormal vestibular central origin or associated with abnormal ocular motility were excluded.
Patients should necessarily have been submitted to ENT examination, medical history, physical examination and audiological assessment consisting of pure tone audiometry, speech audiometry (SRT and SDT) measures of acoustic immittance and acoustic reflex testing, but his analysis is not part of this study.
Before evaluation, patients were asked to remain fasting four hours before the exam, avoid stress, fatigue, smoking, drugs or medicines as painkillers, tranquilizers and anti-vertigo, chocolate and beverages containing caffeine (like tea, coffee, soft drinks ) or alcohol three days before the evaluation (3) and not wear contact lenses, makeup or face creams on exam day.
Tests included: research on positioning and positional nystagmus, eye movement calibration, NE (made in fixing the front look with eyes open and closed), semi-spontaneous saccadic movements, pendular tracking, optokinetic nystagmus, rotatory test pendular and caloric test with air at 42o and 18o C and in some cases, at 10o C.
In the caloric test the patient was supine with the head elevated at 30o and was instructed to perform mental activity for no cortical inhibition during the test. The evaluation was performed by means of thermal stimulation in the ears separately, with air at 42o and 18o C for 80 seconds, with intervals of three minutes between stimulation and another.
The presence of NEOF and / or pre-caloric and its influence on test results were investigated, besides the characterization of his VACL, its direction and symmetry of the evidence.
The criteria for performance and interpretation were based on pre-established values (1) for use of this equipment (1).
From the data collected, comparisons were made between genders, ages, angular velocity and direction of spontaneous nystagmus, caloric test results and completion of entrance examination.
After sample collection, the results were analyzed statistically. We used the Test of Equal Proportions and two p-value <0.005 was considered statistically significant.
RESULTS We analyzed 373 patients attended the entrance examination for the years 2000 to 2007 with the presence of NEOF. Of the 373 tests analyzed, 300 met the requirements for inclusion.
The sample comprised 73.7% females and 26.3% were male, and the difference between the sexes was statistically significant.
Regarding age, subjects were divided into age groups: 4.33% ageless, 1.33% of 18-20 years, 21-40 to 14.67%, 43.33% of 41-60, 34, 67% 61-80% 80-100 1.67. The age of 41-60 years had significant values in comparison to other ages.
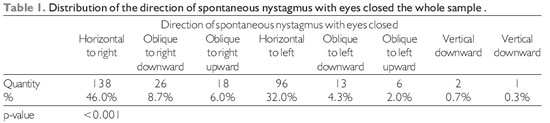
Characteristics of NEOF, we found that the direction was more prevalent horizontal to the right, being significant in relation to others (Table 1).
It was noted that most individuals presented VACL smaller than the 7o/s (86.6%), which was statistically significant than the cases with more than VACL 7o/s (12.33%). 1% showed vertical nystagmus and had no measure of VACL, since it was used in this study only VACL average values related to the first channel of record VENG. In 86% of individuals who had some kind of influence NEOF the VACL of NEOF was lower than the 7o/s and 14% was equal to or greater than the 7o/s.
The other stages of vestibulometry were analyzed, but there were no influences of NEOF.
Of the total sample, 59% had some kind of influence caused by NEOF in the caloric and 41% had not had any influence, the difference being statistically significant.
The NEOF influence the answers of caloric tests in the following ways: hyperreflexia, hyporeflexia, reversal of the nystagmus, abnormal PL, NDP abnormal in conventional tests (hot and cold) and the calculation of symmetry in the cold caloric test.
Inversions were observed unilateral post-caloric nystagmus in 14% and 86% of patients were not observed inversions, and the absence of this finding was statistically significant.Reversals of the post-caloric nystagmus occurred in the opposite direction to that expected in all cases with this type of influence, ie to beat the same side of the eye movement. All inversions were unilateral and in some cases, occurred in more than one stimulation. All presented the findings of the hot caloric test, and 2.3% were also on caloric cold, ear opposite the hot race that appeared in and 11.9% were also frozen at the caloric test on the same side that appeared in the test cold. Statistical analysis showed that the inversion in the warm caloric test had a statistically significant value compared to the same stimuli found in cold and icy.
There were no significant values when comparing the reversal by the influence of laterality NEOF and the three temperatures.
In warm caloric test, we observed normoreflexia values (between 2o/s and 19o/s) in 72.3%, 3.3% hyporeflexia, hyperreflexia (values above 19o/ s) 10.3 % and inversion (right or left ear) in 14%. The normoreflexia obtained a statistically significant value in relation to other abnormal findings.
In cold proof, 46% presented normoreflexia, 2% hyporeflexia, hyperreflexia 49.7% and 2.3% reversal of post-caloric nystagmus. The most prevalent response was "hyper-reflexia, but this was not considered statistically different from the percentage of response" normoreflexia "but in relation to others, hyperreflexia showed statistically significant values.
Of those who had hyperreflexia in the warm caloric test, 32.3% had bilateral hyperreflexia and 67.7% unilateral, and 66.7% for the same side in NEOF, and 33.3% for the opposite NEOF In both cases the values were significant.
Of those who had hyperreflexia in the cold caloric test, 63.8% had bilateral hyperreflexia and 36.2% unilateral, and 74.1% for the same side in NEOF, and 25.9% for the opposite NEOF .Both values were statistically significant.
Of the 51 who had SVPD, we observed that 36 had lower values and showed no inversions. In the analysis of data from the hot caloric test, 58.3% showed reduced values for the same side of NEOF, while 41.7% showed these values to the opposite side. In the analysis of data from the cold caloric test, 41.7% showed reduced values for the same side of NEOF and 58.3% had values for the opposite side. The values were not statistically significant.
On completion of entrance examination, we obtained 36.0% with EVN, 4.7% with the IPVS D, 5% with the IPVS And BIPVS with 28.7%, 7.7% with the SVPD D, 6.7% SVPD with the E, with 2.7% and 8.7% SVPDB as inconclusive. The most frequent finding was the normal vestibular tests, which was statistically significant compared to other conclusions. However, when analyzing the statistical test results, we observed that this percentage cannot be considered statistically significant considering the percentage of completion of BIPVS, present in 28.7% of cases.
In warm caloric test, among the 36 who presented the final conclusion SVPD, 58.3% had lower values for the same side of NEOF and 41.7% had lower values for the opposite side. Already in the cold caloric test, 41.7% had lower values for the same side of NEOF while 58.3% had lower values for the opposite side. In both tests there were no statistically significant values.
In analyzing the relative values of the caloric test of the whole sample, comparing the values of hot and cold stimulation, 28.3% and 29.3% had NDP PL. Of the 116 who took the cold caloric test, was calculated at 33.7 the NDP (symmetry), and 8.7% of the total sample could not perform any calculation. There was no significant values in this analysis.
Of individuals who had the NDP, 82% were normal, while 18% had abnormal results. NDP 60% had changed to the same side of NEOF, and 40% for the opposite side of NEOF.
LP was observed in 78.4% normal and abnormal in 21.6. 42.1% PL was changed to the same side of NEOF and 57.9% in the PL was changed to the opposite NEOF.
Comparing the abnormal values of the NDP, PL, hyperreflexia and hyporeflexia at 42 and 18oC, we observed that when compared with NDP MP and NDP with hyperreflexia, no statistically significant figures, but the NDP compared with PL, hyperreflexia and hyporeflexia at 42o and 18oC value was significant. By comparing PL with hyperreflexia and hyporeflexia at 42o and 18oC, it was verified that these were statistically significant. Comparing hyperreflexia and hyporeflexia 18o and 42o C there was no significant value.
Of the total sample, 38.7% of subjects underwent caloric frozen while 61.3% did not accomplish, and those who did not undergo the cold caloric test, statistically significant compared to those who carried out this test.
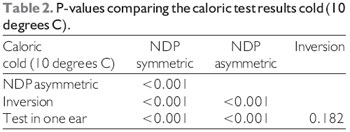
In calculating the NDP of the 116 who took the cold caloric test (10oC), 56.9% had symmetry of responses (30%), 30.2% showed asymmetry and 12.9% could not perform any calculation therefore 4.3% had unilateral reversal of post-caloric nystagmus, and 8.6% in this test was done only in one ear (the same one that was influenced by the cold stimulation). It was concluded that the symmetry in the calculation of PDN was statistically significant compared to other findings in this test.
In 57.8% of subjects who underwent caloric ice was observed some kind of influence NEOF, while 42.2% did not. Those who had some kind of influence NEOF were significant compared to patients without influence.
Of the 67 who had some kind of influence NEOF and held the cold caloric test, 79% was reached on a final exam, and you can say that in these cases was the influence of NEOF withdrawal, while 21% were inconclusive as because it was not possible to remove the influence of NEOF. The tests were inconclusive, and higher prevalence were statistically significant in relation to inconclusive.
Of the 116 who took the cold caloric test, it was possible to reach a conclusion only in 80.2% and 19.8% remained inconclusive. Those who could reach a conclusion, the values were statistically significant in relation to inconclusive.
By comparing the cold caloric test results related to the NDP as symmetrical or asymmetrical, or reversal test performed only in one ear, it was observed that the comparison of values between NDP symmetric with asymmetric findings, inversion and test performed only in one ear, was statistically significant, the values of the comparison between the NDP and reversal with asymmetric caloric test only in one ear were also statistically significant, and comparing with reversal test performed in only one ear had no significant values (Table 2).
DISCUSSION The study population consisted of mostly women (73.7%), with a mean age of 55.08 years. These findings were similar to those found by several authors (12-17).
The direction was more prevalent NEOF the horizontal to the right, with significant values compared to other directions, a result similar to those found in the literature (8,12,18,19).
We find the values of VACL NEOF smaller than the 7o/ s in 86.7% of the total sample, and 86% of those who had some kind of influence NEOF VACL also showed less than 7o/ s. In both comparisons, these values were statistically significant. Stands out, so that the NEOF, even presenting within the normal range, influenced the majority of examinations, becoming thus the finding of relevant importance, requiring greater caution when performing the examinations and tests confirm the diagnosis for an individual who fails to do so in error, since the influence can change significantly the responses of post-caloric nystagmus.
In surveys analyzed, were found only in NEOF influences caloric test. Some authors stated that the preponderance NE may lead to the same side of nystagmus (10), and can cause directional asymmetry than the limit of the normal pattern of post-caloric nystagmus (11).
In warm caloric test, it was observed as a result normoreflexia most common (72.3%) and 66.7% was found hyperreflexia in the same direction of unilateral NEOF. In cold test, 49.7% had hyperreflexia, and unilateral in 74.1% in the same direction NEOF. In all analysis values were statistically significant, similar to the literature (18,20).
According to the authors NE could, algebra, it can be added or subtracted on the post-caloric nystagmus. This was not observed in this study, since even very small values of the VACL NEOF also caused hyperreflexia, at different rates quoted by the author.
Among patients with PDN (15%) or PL (21.6%) abnormal, we find values similar to those found by several authors (12,20). The NDP may reflect the effect of NEOF or may be associated with hyporeflexia or unilateral Bilateral (21). The NDP occurs when the response of post-caloric nystagmus is greater for one direction than another. In his clinic, found that the NDP was more prevalent in patients with strong IR (22).
The conclusions of VENG more prevalent in this sample were: EVN and BIPVS, both being statistically significant when compared to other conclusions, but there was no difference between the two, similar to the literature (18, 23). Even before the examinations within the normal range, we can not say that this outcome is the same in the absence of NEOF, which could influence the caloric responses, decreasing the values opposite him, or override the direction in which it occurs, masking, so the actual values of this test.
It was observed that the population of those who carried out the cold caloric test was lower than in individuals who did not perform this test, showing that is not widely used, as reported in the literature (24). However, it can be stated that the cold caloric test was efficient in the removal of the influence of NEOF since after their application has been possible to reach definitive conclusions in 79% of those who had some influence NEOF and underwent this stimulation, according to the literature that the findings prove ice provides the most reliable diagnostic (12-18). Moreover in some cases the influence of NE can not be removed even when performed cold caloric test (21).
Thus, it was possible to verify that the evaluation and detailed minusciosa NEOF is required since this causes interference relevant during testing of the caloric test, resulting in erroneous or misleading conclusions, and interesting to conduct more specific studies in this area.
CONCLUSION Given the findings of this study in patients with chronic peripheral vestibular dysfunction and presence of digital NEOF VENG can conclude: NEOF most common type was horizontal, with VACL smaller than the 7o/ s, which influenced the majority of examinations and only the results of the air caloric test with reversal of post-caloric nystagmus, hyperreflexia and hyporeflexia, NDP and PL altered; the findings were more prevalent and BIPVS EVN, and the cold caloric test (10 C) removed the influence of NEOF in most of the individuals who performed, allowing to reach a final conclusion.
BIBLIOGRAPHICAL REFERENCES 1. Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG, Frazza MM. As etapas da equilibriometria. In: Caovila HH, Ganança MM, Munhoz MSL, Silva MLG. Equilibriometria Clínica. 5a ed. São Paulo: Atheneu; 2000, p. 41-114.
2. Honrubia V. Testes quantitativos da função vestibular e o exame clínico. In: Herdman SJ. Reabilitação Vestibular. 2a ed. São Paulo: Manole; 2002, p. 105-68.
3. Albernaz PLM, Ganança MM, Ito YI, Falsetti HCD, Caovilla HH, Ramos RF, Queirós BMA, Filho PMA. Aspectos Técnicos da Electronistagmografia. ACTA AWHO. 1982, 1(2): 41-4.
4. Caovilla HH, Ganança MM, Munhoz MSL, Silva MLG, Ganança FF, Ganança CF. O registro dos movimentos oculares. In: Caovila HH, Ganança MM, Munhoz MSL, Silva MLG. Equilibriometria Clínica. 5a ed. São Paulo: Atheneu; 2000. p. 31-40.
5. Boaglio M. Da Vectonistagmografia Computadorizada em Portadores de Doença de Ménière [tese]. São Paulo. Universidade Federal de São Paulo; 2001.
6. Watanabe Y, Takeda S. Computerized Electro-nystagmography. Acta Otolaryngol (Stockh). 1996; Suppl 522:26-31.
7. Coats AC. The diagnostic significance of spontaneous nystagmus as observed in the electronystagmographic examination. Acta Otolaryngol. 1969, 67:33-42.
8. Takahashi J, Kitamura K, Miyata M. Spontaneous Nystagmus in Normal Subjects. ORL. 1996, 58:42-45.
9. Kenneth H, Brookler MD. Direction-fixed positional nystagmus; spontaneous nystagmus. ENT-Ear, Nose & Throat Journal. October 1999.
10. Toupet M. Comment Le Nystagmus Spontané Modifie Le Nystagmus Provoqué Par La Stimulation Vestibulaire Calorique, Chez 34 Patients Atteints de Névrite Vestibulaire. Ann. Oto-Laryng, Paris. 1982, 99:453-464.
11. Albernaz PLM, Ganança MM. Atlas de eltronistagmografia. São Paulo: Editamed; 1977, p.44.
12. Santos FA. Da Estimulação Calórica Gelada nas Vestibulopatias Periféricas Com Nistagmo Espontâneo de Olhos Fechados [tese]. São Paulo. Universidade Federal de São Paulo; 2007.
13. Gazzola JM, Ganança FF, Aratani MC, Perracini MR, Ganança MM. Caracterização clínica de idosos com disfunção vestibuar crônica. Rev Bras Otorrinolaringol. 2006, 72(4): 512-22.
14. Traldi L, Pedalini MEB, Bittar RSM, Bottino MA. Relação entre os resultados da prova calórica e evolução de pacientes submetidos à reabilitação vestibular. Arquivos Internacionais de ORL. 2004, 8(4):294-98.
15. Bovolini A, Ganança CF, Ganança FF, Ganança MM,Caovila HH. Prevalência de anormalidades às provas calóricas com água e com ar em vestibulopatias periféricas crônicas. ACTA ORL/Técnincas em Otorrinolariongologia. 2007, 25(2):165-69.
16. Pedalini MEB, Bittar RSM, Formigoni LG, Cruz OLM, Bento RF, Miniti A. Reablitação vestibular como tratamento da tontura: experiência com 116 casos. Arquivos Internacionais de ORL. 1999, 3(2):87-92.
17. Assunção ARM, Albertino S, Lima MAMT. Auto-rotação cefálica ativa em pacientes com tontura / vertigem. Rev Bras Otorrinolaringol. 2002, 68(1):57-63.
18. Manso A, Bruner AP, Ganança CF, Silva SMR, Bellini AC. Influência do nistagmo espontâneo de olhos fechados sobre o resultado da prova calórica no exame vestibular. In: XX Encontro Internacional de Audiologia; 2005. São Paulo (SP); 21 a 24 de Abril.
19. Braga HM. Do Nistagmo Espontâneo e Semi-Espontâneo em Indivíduos Normais. Pesquisa Vecto-Eletronistag-mográfica [tese]. São Paulo. Universidade federal de São Paulo; 1980.
20. Resque JR, Filho MS. Prova calórica gelada em indivíduos com presença de nistagmo espontâneo de olhos fechados na vectonistagmografia computadorizada. In: XXIII Encontro Internacional de Audiologia; 2008. Itajaí (SC); 12 a 15 de Março.
21. Shepard NT, Teilan SA. Pratical management of the balance disorder patient. San Diego: Singular, 1996.
22. Jacobson GP, Newman CW, Peterson EL. Interpretation and usefulness of caloric testing. In: Jacobson GP, Newman CW, Kartush JM. Handbook of balance function testing. St. Louis: Mosby; 1993. p. 193-233.
23. Almeida RP, Câmara MFS. Análise comparativa do nistagmo pós-calórico com duas e quatro estimulações através da vectonistagmografia. Revista Brasileira e Promoção de Saúde. 2004, 17(3):135-7.
24. Gonçalves DU, Felipe L, Lima TMA. Interpretação e utilidade da prova calórica. Rev Bras Otorrinolaringol. 2008, 74(3):440-6.
1 Bachelor's Degree in Speech Pathology, UNIFESP-EPM. Speech.
2 Master of Science Program of Human Communication Disorders, UNIFESP-EPM. Hospital Speech Cema.
3 Doctor of Science, Program of Human Communication Disorders, UNIFESP-EPM. Visiting Professor in the Department of Otoneurology of Speech Therapy, UNIFESP-EPM.
Institution: Departments of Otolaryngology and Speech Pathology, Federal University of São Paulo - UNIFESP. São Paulo / SP - Brazil. Mail Address: Andrew Manso - Avenida Conception, 111 - Apt. 22 - Tower A2 - Carandiru, São Paulo / SP - Brazil - Zip code: 02072-000 - Telephone: (11) 9249-9803 - E-mail: andreamanso@bol.com.br
Article received in November 4, 2009. Article accepted in March 25, 2010.