INTRODUCTIONFor several years, scientific studies have demonstrated the theory of participation of the extrinsic muscles of the larynx in the function of phonation. However, some studies cast doubt on the participation of external muscles of the larynx in voice production. In parallel, several studies show that clinical dysphonia, especially hyperkinetic or hyperfunctional, may be related to imbalance of neck muscles. In general, this pattern persists in hyperfunctional phonatory different situations and can promote the development of organ damage. Still, organic changes may induce a functional fit inadequate causing dysphonia.
Some authors consider that musculoskeletal tension syndrome, also known as dysphonia by muscular tension, it is an extensive series of vocal non-specific, and difficult to define a dysphonia. They identify two categories of causal musculoskeletal tension syndrome: the primary, with no structural changes in the larynx, and the secondary, with the presence of tissue reactions. Laryngoscopy the syndrome of primary musculoskeletal strain shows normal structure and mobility of the vocal folds. In the tension syndrome secondary musculoskeletal there laryngeal lesions such as nodules, polyps and edema. Thus, signals are observed as deviations in the posture of the head and neck, hyperextension of the head, neck, grooved, inspiration and enormous strain on inadequate mouth opening to the issue. Therefore, there is clinical aspects related to conditions of dysphonia as postural changes, musculoskeletal and psycho-emotional aspect ratio with the voice.
Thus, this research aims to investigate the relationship of functional voice disorders and organic changes in women with cervical skeletal muscle.
METHODParticipated in this cross-sectional study 50 subjects, aged 25-55 years and 32 (experimental group) with voice complaints and algia cervical and 18 (control group) without voice complaints and independent algia neck.
Inclusion criteria were female gender, presence of vocal and complaint of cervical algia. Exclusion criteria were cardiovascular diseases, autoimmune diseases, and diabetes traqueobroncopulmonares, the use of NSAIDs and hormonal, analgesic, mouthwash or other medication as well as therapeutic procedures that interfere in the vocal complaints or neck.
All subjects signed an informed consent form (00114/2007), where they obtained information about the objectives, procedures and clarifications were made on the guarantees of the study.
Participants in this study were selected through a previously designed questionnaire that contained objective and subjective questions, answers with single, multiple and descriptive. This was distributed to public and private schools, from kindergarten to elementary school, and to selected patients per physician or orthopedist otolaryngologist in private practice. The questionnaire included questions about the identification, professional activity, the presence or absence of vocal complaints, laryngeal sensation, the pain in the neck and shoulders, and the association of pain with dysphonia. Initially, 80 questionnaires were collected which allowed the selection of 50 individuals, 32 (experimental group) with voice complaints and algia cervical and 18 (control group).
All subjects underwent otorhinolaryngological (ENT), orthopedic, physical therapy and vocal register. The evaluation consisted of completion of DSB videolaryngostroboscopy performed by a specialist for diagnosis. The evaluation was performed by orthopedic specialist, that based on complaints of cervical algia applied testing cervical motion in flexion, extension, lateral rotation and right and left lateral tilt in an active, specific tests of tensile, compression, Valsalva maneuver and muscle shortening, as well as palpation of soft tissues. The cervical spine was investigated by X-ray simple, the impact of profile, anteroposterior and posteroanterior. The evaluation consisted of physical therapy postural examination of inspection, in which the individual was positioned in front of a table posture for the visualization of the profiles, lateral and posterior. Following were palpated the trapezius (upper fibers), sternocleidomastoid, scalene fibers (anterior, medial and posterior), bilateral inferior nuchal line and the "base of the neck, in order to identify" trigger points "and the presence of pain. Then, tests were performed for shortening the trapezius (upper fibers), sternocleidomastoid and erector spine. The voice recording provided the perceptual assessment for classification of individuals in groups and not dysphonic dysphonic. To record the voices used a unidirectional condenser microphone headset ultimate professional, stereo, brand Plantronics Audio 90®, coupled to a notebookcomputer Toshiba A135-S4737 model, and the software Multi Speech - MDVP from Kay Elemetrics®, belonging to the voice laboratory at the University Tuiuti. The subject was instructed to speak spontaneously for 30 seconds answering the question: "What do you think of his voice "breathing naturally and pace of speech, with habitual pitch and loudness. The subjects repeated this issue three times, at intervals of 30 seconds between recordings. The perceptual analysis was performed by three speech therapists in a double blind, by consensus, with a sample of spontaneous speech and consisted of the classification of voice type, based on GRBAS - proposed by HIRANO (1981).
The results, isolated and associates, were analyzed by testing differences in proportions, Chi-square test, Fisher and Mann-Whitney, considering the significance level of 0.05%.
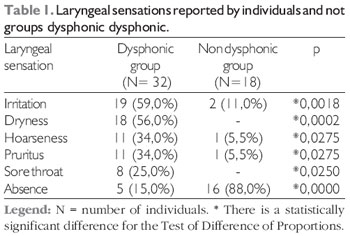
RESULTSThe results for laryngeal sensations, investigated through a questionnaire, showed that in patients with dysphonia, 59% had irritation, dryness 56%, 34% of phlegm and itchy, sore throat in 25% and 15% reported no complaints ( Table 1) with a statistically significant difference compared with the non-dysphonic group (p <0.005).
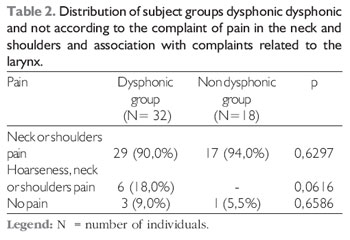
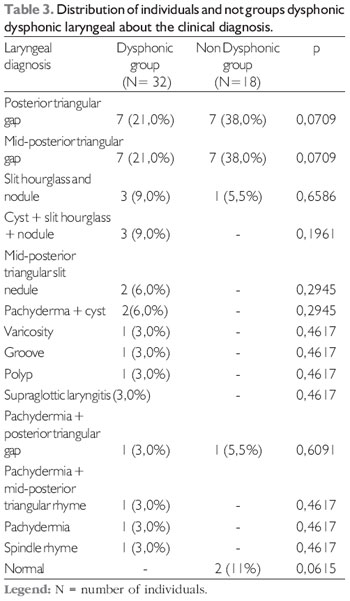
Regarding the assessment of pain in the neck and shoulders are the results in Table 2. In addition, Table 3 shows the relationship between individuals and assessed clinical diagnosis throat.
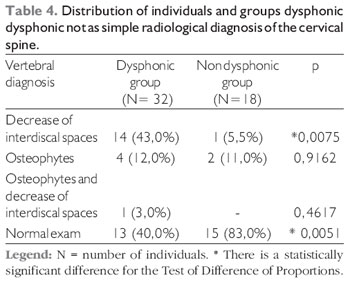
The evaluation of X-ray cervical spine showed statistical difference when comparing the groups with regard to the reduction of spaces interdiscal, more frequent changes in dysphonic and, conversely, normal cervical x-ray, being more prevalent in the control group (Table 4).
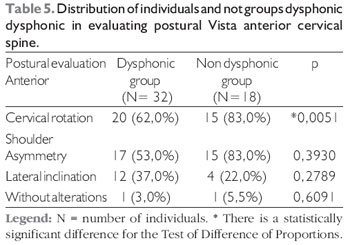
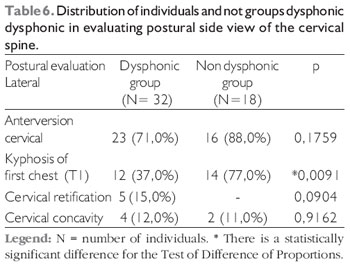
Analyzing the data postural, referring to the anterior cervical spine in patients with dysphonia, 62% had neck rotation, and in patients not dysphonic this disorder was observed in 83%.(Table 5). Still, the assessment of cervical spine lateral group of dysphonic kyphosis from T1 in 37%, while in patients with dysphonia not met 77%, a statistically significant (Table 6).
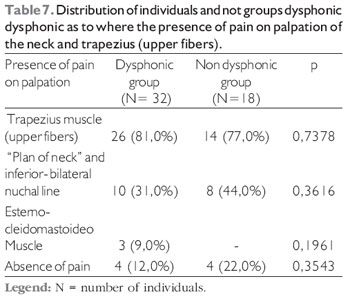
The results for the presence of pain on palpation of the neck and trapezius (upper fibers) is shown in Table 7, but the results are not statistically significant.
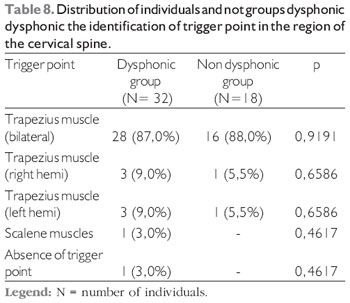
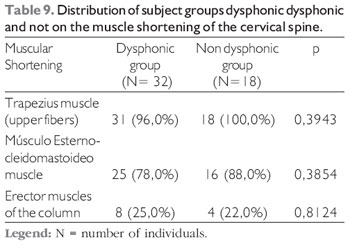
Finally, the identification of trigger points in the region of the cervical spine (Table 8) and also in the evaluation of muscle shortening of the cervical spine (Table 9) showed no differences between the two groups.
DISCUSSIONThe woman elected individual in this research presents the largest number of complaints of vocal disorders, because they speak with greater intensity and frequency as well as use their voice as a resource professional. They will also have a laryngeal anatomy collaborating with small size, coupled with the higher voice, for the development of vocal and neck.
In the present study was reported, through an initial interview, the presence of laryngeal symptoms in both groups and non-dysphonic dysphonic. These feelings cause laryngeal discomfort in the act of speaking and swallowing, preventing the individual from having good vocal production and viable communication and clear, causing disruption in the workplace and even in the social environment. The combination of sensation and laryngeal vocal complaints provoke an intense vocal disorder which is called dysphagia.
Regardless of the presence of vocal, women are predisposed to the presence of pain, discomfort and neck muscle fatigue in the neck. However, no findings in the literature that make reference regarding the symptom of pain in the cervical spine in dysphonic individuals.
In parallel, during the evaluation videolaryngoscopic demonstrated that the diagnosis of posterior triangular glottic rima and mid-posterior is quite common and considered physiological when it comes to rhyming female glottal. However, the perceptual assessment noted the presence of voice alteration, but without lesions of vocal folds. These data lead us to believe the most common causes of dysphonia as the misuse of voice or vocal abuse (1).
Still, the research subjects underwent a radiologic examination of simple in order to identify bone lesions and define the reasons for neck and shoulder pains. It is possible that bone and muscle imbalances as increased thoracic kyphosis caused by bad posture habits and lack of ergonomics, the muscle retractions, the direct and indirect trauma, the physical and emotional stress, environmental factors and even sedentary are the primary causes of these aches, and unlikely causes of bone origin, disagreeing with the results from the literature, which cites as a major cause of osteoarthritis neck pains (2).
In this study, were observed and identified important changes in the cervical region in both women with dysphonia as in without vocal. However, there was a greater number of patients with positional changes in the dysphonic group does not and cannot be attributed therefore dysphonia as a precipitating cause of postural change. It is worth noting that there were no differences in the asymmetry of the shoulders, in disagreement with a study, which found an asymmetry of the shoulders dysphonic patients (3).
The trigger points are in palpable muscle nodules, most painful, originated after minor trauma, direct or indirect injuries that produce muscular fascia. This study detected the presence of considerable trigger points, especially in the trapezius region (upper fibers), similar in both groups. We found no references to the presence of trigger points in the literature in dysphonic women.
In parallel, we identified significant decreases in both muscle groups, but these changes are independent of the inappropriate use of voice. Moreover, this study showed that women dysphonic group showed shortening the sternocleidomastoid muscle and trapezius (upper fibers), in agreement with literature data (4). It is important to remember that most patients presenting with symptoms of functional dysphonia due to vocal abuse or misuse of the voice, which can be obtained from the level of muscle tension and shortening of the cervical region and thus does not show the laryngoscopy characteristic structural changes (5). The increase in tone throughout the intrinsic and extrinsic laryngeal muscles simultaneously, associated with the presence of posterior glottic gap and define the high laryngeal muscle tension dysphonia (6,7,8,9,10). Still, studies report that a speech constantly associated with an inadequate laryngeal posture can lead to organic changes such as nodules or polyps, particularly in women, with the presence of posterior glottic chink, associated to increased laryngeal tension and more directly to the imbalance of posterior cricoarytenoid muscle during speech (8, 11). The results of this study agree with the literature, since most of the participants showed a marked dysphonia dysphonic in auditory-perceptual evaluation, and muscle shortening in the neck, but the diagnosis by videolaryngostroboscopy showed no lesion on the vocal folds (8). The increase in cervical lordosis and / or lumbar, increased thoracic kyphosis and / or changes in head position can lead to compensation in the cervical region and also in the larynx (12, 13).
In spite of much evidence, we put in question the relation of dysphonia with the participation of the neck muscles or external paralaríngea (11), since women do not have many dysphonic dysphonic changes in the contributing to the theory that raises doubts about the participation of external laryngeal muscle on voice.
Above all, this research has proved valuable and surprising as the research and detection of posture in both women with and without vocals. While contributing to the multidisciplinary treatment (otolaryngology, orthopedics, physical therapy and speech therapy) and the continuity of it to get better benefits and information society.
CONCLUSIONThe present study demonstrated that major changes were identified in women with cervical or without dysphonia, it is not possible to determine a causal relationship between them.
BIBLIOGRAPHIC REFERENCES1. Greene MCL. Distúrbios da voz. 4a. ed. São Paulo: Manole; 1989.
2. Knoplich J. Enfermidades da Coluna Vertebral. 2a ed. São Paulo: Panamed; 1986.
3. Nelli EA. Estudo da postura corporal em portadores de disfonia [dissertação]. Bauru (SP): Universidade de São Paulo; 2006.
4. Anelli W, Xavier C. Novo enfoque de atendimento a pacientes disfônicos em instituição: grupos de orientação In: Marchezan IQ, Bolaffi C, Gomes ICD, Zorzi JL. Tópicos em Fonoaudiologia. São Paulo: Lovise; 1995. p. 331-347.
5. Imamura R, Tsuji DH. Disfonia espasmódica de adução, tremor vocal e disfonia de tensão muscular: é possível fazer o diagnóstico diferencial? RevBras Otorrinolaringol. 2006, 72(4):434.
6. Aronson AE, Brown JR, Litin EM, Pearson JS. Spastic dysphonia. II. Comparison with essential (voice) tremor and other neurologic and psychogenic dysphonias. J Speech Hear Disord. 1968, 33(3):219-31.
7. Barkmeier JM, Case JL. Differential diagnosis of adductor-type spasmodic dysphonia, vocal tremor, and muscle tension dysphonia. Curr Opin Otolaryngol Head Neck Surg. 2000, 8(3):174-9.
8. Morrison MD, Rammage LA, Belisle GM, Pullan CB, Nichol H. Muscular tension dysphonia. The Journal of Otolaryngology. 1983, 12(5):302-6.
9. Aronson AE. Organic voice disorders: neurologic disease. In: Clinical voice disorders. New York: Thieme Inc.;1985. p. 76-125.
10. Colton RH, Casper JK. Compreendendo os problemas de voz: uma perspectiva fisiológica ao diagnóstico e ao tratamento. Porto Alegre: Artes Médicas; 1996. p. 3-215.
11. Angsuwarangsee T, Morrison M. Extrinsic laryngeal muscular tension in patients with voice disorders. J Voice. 2002, 16:333-43.
12. Grini MN, Oaknine M, Giovanni A. Contemporary postural and segmental modification of forced voice. Rev. Laryngol Otol Rhinol. 1998, 119(4):253-7.
13. Hsiung MW, Hsiao YC. The Characteristic Features of Muscle Tension Dysphonia before and after Surgery in Benign Lesions of the Vocal Fold. ORL. 2004, 66:246-254.
1 Master in Communication Disorders at the University Tuiuti. Physiotherapist.
2 PhD, UNIFESP. Professor of the Masters Program in Communication Disorders at the University Tuiuti.
3 Doctor Unicamp. Professor, Master's and Doctoral Program in Communication Disorders at the University Tuiuti.
4 PhD in Clinical - Surgical UFPR. Head of the Department of Laryngology of the Hospital Angelina Caron.
5 Medical. ENT resident.
Institution: University of Tuiuti Paraná. Curitiba / PR - Brazil. Mail Address: Nathália Martini Monti Wolff - Sector Master Program in Communication Disorders - Rua Sydnei A Rangel Santos, 238 - Curitiba / PR - Brazil - Zip code: 82010-330 - Telephone: (+55 41) 3331-7700 - E-mail: nathaliawolff@terra.com.br
Article received on June 14, 2010. Approved on 1 October 2010.