INTRODUCTIONParkinson disease (PD) is a degenerating disease with a deceitful character, impairing the central nervous system (CNS) and causing biological, psychological and social changes, presenting motor signs and symptoms characterized by trembling, rigidity and bradykinesia. Additionally, other difficulties in concentration, learning, memory, understanding, dysarthria and dysphagia can occur (1). Although without the same clinical importance, non-motor signs can occur, as follows: depression, sleep disorders and cognitive alterations. In more advanced stages, the impairment on sound articulation can be such that PD oral communication can be greatly affected (1).
It is known that peripheral hearing involves an amplification and a conduction of the sound waves, as well as the perception of sound vibrations that are converted into nerve impulses. Central hearing involves the conduction of the nerve impulses by the auditory pathways towards the auditory cortex, where they will be codified and re-codified, achieving a linguistic meaning (2).
The effects caused by degenerating processes can involve both the inner ear and CNS (3). Alteration of the hearing process (HP) can occur as a result of the changes directly impacting the brain mechanism (2).
According to the definition proposed by the American Speech Hearing and Language Association (ASHA) (4), HP is comprised of mechanisms and processes of the auditory system responsible for several behavioral phenomena, including speech and language, having a neurophysiological and functional association. Accordingly, it is necessary that the acoustic sign is analyzed and interpreted in order to be converted into a meaningful message (5).
The brain is responsible for processing the speech, which starts in cochlea, where the mechanical activity is turned into nerve impulses. The hearing activity, in the physiological meaning consists of three factors: peripheral activity, central auditory activity and CNS processes. When one of these factors is broken, it results in a deficit in the speech recognition ability. The sound perception occurs by the central activity and the sound sensation is originated by the peripheral activities. All these analyses and interpretations are integral parts of HP. While the peripheral auditory system receives and analyzes the hearing stimuli of the environment, the central auditory system and the brain analyze the internal representations of these acoustic stimuli, and a response is programmed by the individual (6). Accordingly, it is necessary that the abilities of detection, sensation, discrimination, localization, recognition, understanding, attention and memory involving the HP, will function.
Auditory memory is a process that allows acoustic information to be obtained, stored and archived. This ability found in the HP development is often changed in the Parkinson patient, due to using some drugs such as levodopa, which is widely used and can result in memory disorders and, in more severe cases, cause mental confusion and hallucinations (7).
The Staggered Spondaic Word Test (SSW) translated into Portuguese as dichotic test of alternate disyllables measures the hearing integrity in the central level, identifies the impairment of both the encephalic trunk of right and left hemispheres and the inter- and intra-hemispheric connections. The dichotic technique uses different acoustic stimuli in both ears simultaneously, with the intention of evaluating the hearing abilities for binaural separation and integration (8, 9).
The diagnosis for a central hearing processing disorder (CHP) is characterized by a difficulty as a result of an impairment of the hearing abilities and it must be considered a hearing disorder. This diagnosis allows the phonoaudiological rehabilitation process to be changed by training the hearing so that a more effective therapeutics can be achieved (9).
Therefore, the objective of this study was to evaluate the central hearing function in PD patients.
METHODThis study was approved by the Research Ethics Committee's Resolution No. 008/2005 and authorized by the patients after signing a Term of Free and Clarified Agreement.
The casuistics was composed by 20 individuals in both sexes, divided into two groups:10 individuals were diagnosed of PD according to Queen Square Brain Bank's criteria used by the Paranaense Association of Parkinsonism Patients (PAPP) called study group (SG) and 10 normal individuals - control group (CG). The average age in both groups was 63.8 and (±SD) 5.96. Both groups were evaluated in the Audiology Laboratory of an Educational Institution in the city of Curitiba / PR.
To create the CG, individuals over 60 years of age with a normal hearing for their age, as ruled by ISO-7029 (10), a preserved cognition, and no inner ear pathology, and individuals with an otological alteration or other abnormalities making examinations unfeasible were excluded.
Firstly, all the individuals were submitted to an anamnesis, otorhinolaryngological and regular audiological evaluations, comprised of a pure-tone threshold audiometer, speech recognition threshold, percentage rate of speech recognition, and immittance audiometry. The audiological evaluation was performed in an acoustic booth with an Interacoustics AC-40 audiometer and a TDH 39P ANSI-69-calibrated phone. To perform the immittance audiometry, Interacoustics AZ-26 iimpedanciometer and TDH 39P phones were used.
Secondly, both groups were submitted to the HP in which the SSW test was performed.
The SSW was proposed by KATZ (8) and customized into the Brazilian Portuguese by BORGES (11). The individuals were told to carefully listen to a sequential four-word group and repeat them in their order of appearance, in a total of forty four-word groups. Each word is received through each ear with a partial superposition, i.e., the second syllable of the first word and the first syllable of the last word are simultaneously received through both ears. The test makes it possible to perform a quantitative and qualitative analysis of the CNS function (5,11,12).
In the quantitative analysis, errors were analyzed regarding each condition of each ear separately and the percentage of right answers was computed, identifying the severity degree of the alteration based on this percentage. The number of right answers equal to or above 90% was considered regular, under the conditions of this research - competitive right-ear (CR): the word is received through the right ear with a simultaneous competition in the left ear, and competitive left-ear (CL): the word is received through the left ear with a simultaneous competition in the right ear.
In the qualitative analysis, the tendencies of found responses were analyzed, such as: order effect (OE) - make more mistakes in the two first spondaic words or in the last two of the test items; auditory effect (AE) - make more mistakes when the test is started through either the right or the left ear; A-type - when there is a great number of mistakes on the same column and, eventually, inversions - when the words of an item are repeated under no order.
The evaluations were performed in a single session lasting around 45 minutes.
The results were analyzed in conformity with the same criteria ad those of the original tests converted by Borges (11).
Statistical method
The obtained results were typed on an EXCEL spreadsheet and analyzed by the statistical tests of Statistica software. Fisher and Mann-Whitney tests were used by taking p<0,05 as significant values.
RESULTSThe results of the audiological evaluation, as ruled by ISO 7029 (10) in the SG, were: 60% of the patients showed standard hearing thresholds bilaterally and 40% showed a slight sensorineural hearing loss with a descending configuration bilaterally.
The CG showed a higher standard rate during competitive right-ear (CR) (80%) and competitive left-ear (CL) (60%), and slight alterations CR (20%) and CL (40%). The SG had alterations ranging from slight to severe CR (30%) and CL (60%) and 70% standard level on CR and 40% on CL.
The Graphics 1 and 2 presented the alteration degree that the CG and SG had, respectively, obtained in the evaluated conditions: CR and CL in the SSW test. When comparing the results of the SSW test under these conditions with the Mann-Whitney test, it was observed that there was no significant difference, the CR condition resulted in p = 0,5228 and the CL resulted in p = 0,1903.
As regards the tendencies of responses, the highest percentage was evident in the SG, according to Graphic 3. When comparing SG and CG, it was observed in the Fisher Test that there was no significant difference, AE resulted in p = 0,6285 and OE resulted in = 0,3698, and the A-type standard A resulted in p = 0,3498.
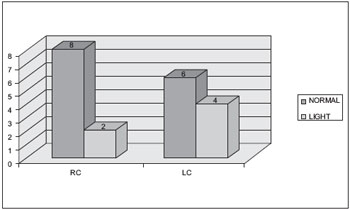
Graphic 1. Results achieved in RC and LC conditions at SSW test in the CG. - CR = competitive right-ear; CL = competitive left-ear; SSW = Staggered Spondaic Word Test; CG = control group.
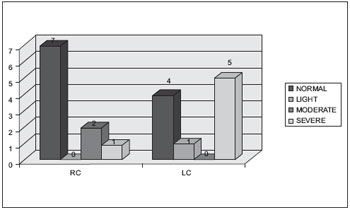
Graphic 2. Results achieved in RC and LC conditions at SSW test in the GE. - CR = competitive right-ear; CL = competitive left-ear; SSW = Staggered Spondaic Word Test; SG = study group.
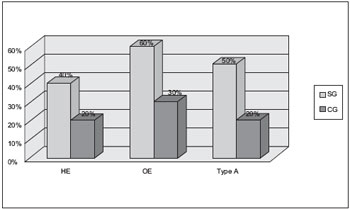
Graphic 3. Results achieved in the tendencies of response to SSW test in both SG and CG - SSW = Staggered Spondaic Word Test; SG = study group; CG = control group; AE = auditory effect; OE = order effect.
With respect to the alteration degree in the SSW test, between the two evaluated groups, the worst results were observed in the SG, although there was no significant difference. This alteration can be associated with aging, for proper physiological modifications derived from pathological processes responsible for the clinical presentation of several of diseases occur in this life stage (13), a noticeable of which is presbycusis. The degenerating effects of aging can involve both the inner ear and CNS (14). Besides presbycusis, a HP alteration can also occur as a result of the metabolic changes and, regarding the age factor, those directly affecting the cerebral mechanism (15).
Studies (14,15) define presbycusis as caused by a wide range of extrinsic and intrinsic negative factors impacting the auditory system. It is clinically approached as an ordinary type of hearing loss provoked by a cochlear degeneration that mainly affects the basal part of the cochlea, impairing the hearing perception at high frequencies. DIVEYI and HAUPT (16) mentions that the sensorineural-type hearing loss cannot be considered the factor determining the HP alterations, however, they can become aggravating. According to the authors (17), the aging effects can involve both the peripheral part and the hearing central part and, when the age factor is directly associated with the peripheral hearing loss, it can be making the dichotic hearing even more difficult. In other studies (18), the authors mention that adults above 50 years of age need a higher sign/noise relation to recognize a sentence in noise and in silence, and age can be a factor that interferes with speech recognition when peripheral hearing is normal.
In both groups, the highest standard percentage in the SSW test occurred on CR. ROSA (19) evaluated three groups of 50-83-year-old individuals subdivided as follows: with a normal hearing for their age and with a hearing loss by using the SSW test. The author found that the right ear presented an advantage of statistically significant right answers in all the evaluated groups. These findings show that there is a difficulty in processing verbal information on the left ear, proving that there is an inefficiency of the inter-hemispheric hearing pathways (20). For the authors (21), the CL deficit occurs when there is an impairment in the corpus callosum. Not all CNS parts can be identified by the SSW test. The areas that are usually not identifiable are called silent areas. These areas involve the visual cortex (occipital lobe) and the parietal posterior-superior area.
In the quantitative analysis, the evident alterations in the SSW test demonstrated a difficulty in the ability of figure and depth and in bineural integration, i.e., the patient has some difficulty in receiving information in both ears and unifying them into a percentile event. This difficulty can occur in pathologies involving the encephalic trunk and its connections. For the authors (22), the CNS structures responsible for this ability are the olivary complex, which receives fibers from both ears and the auditory cortex, which uses intensity differences and arrival time of the sound to make sure where the sound comes from.
In the qualitative analysis, there was a higher number of alterations in the tendencies of responses in the SG than in the CG, although this difference was not significant. A great number of alteration was observed in the SG on high-low (83,33%), what explains the difficulty of the auditory memory in maintaining a received stimulus and properly organizing its emission (23). HP disorder is a specific dysfunction of the hearing processes, but it can also be associated with both memory and attention deficits. The worst performance in the SG's dichotic hearing can be related to an association between the peripheral and central factors. Memory, one of the HP abilities, according to the verified literature (7), is frequently changed because of some drugs that are used.
The OE can also be divided into high-low effect - when there is a higher number of mistakes when the stimuli start through the right ear and low-high - when there is a higher number of mistakes when the stimuli start through the left ear. According to the authors (21), high-low OE is associated with the impairment of the posterior temporal lobe and the auditory cortex.
In the performed statistical tests (Fisher e Mann-Whitney), no significant difference was found between both groups, probably due to the small casuistics, but a qualitative difference can be observed between the groups.
When trying to minimize the altered hearing abilities, some procedures are proposed, such as hearing training (HT) (24). HT is a group of strategies used to develop or rehabilitate the hearing abilities, which are necessary to understand speech. HT is a widespread technique that intervenes in individuals with HP disorders, in order to enhance the auditory system function to resolve acoustic signs based on the neuronal plasticity (24,25).
The information of the audiological evaluation (peripheral and central) are important to identify the functional deficits that will contribute to the procedures to be taken when performing the audiological rehabilitation/capacity on these patients.
CONCLUSIONA qualitative and quantitative difference was observed in SSW test between the evaluated groups, although statistical data does not show significant differences. The importance to evaluate the central hearing process is emphasized when contributing to the procedures to be taken at the therapeutic follow-up.
BIBLIOGRAPHICAL REFERENCES1. Andrade LAF, Barbosa ER, Cardoso F, Teive HAG. Doença de Parkinson: Estratégias atuais de tratamento. São Paulo: Lemos Editorial; 1999.
2. Aquino AMCM et al., organizador. Processamento auditivo - eletrofisiologia & psicoacústica. São Paulo: Lovise; 2002.
3. Fonseca CBF, Iório MCM. Aplicação do teste de lateralização sonora em idosos. Pró-fono. 2006, 18(2):197-206.
4. American Speech Hearing and Language Association Task Force on Central Auditory Processing Consensus Development. Central auditory processing: current status of and research and implications for clinical practice. Am J Audiol. 1996, 5:41-54.
5. Sauer L, Pereira LD, Ciasca SM, Pestun M, Guerreiro MM. Processamento auditivo e SPECT em crianças com dislexia. Arq. Neuropsiquiatr. 2006, 64(1):108-111.
6. Pereira LD, Schochat E. Processamento Auditivo Central: manual de avaliação. São Paulo: Lovise; 1997 p. 175-176.
7. Miranda ES, Pereira LD, Bommarito S, Silva TM. Avaliação do processamento auditivo de sons não-verbais em indivíduos com doença de Parkinson. Rev Bras Otorrinolarinol. 2004, 70(4):534-539.
8. Katz J. The use of spondaic staggered words for assessing the integrity of the central auditory nervous system. J Auditory Res. 1962, 2:327-337.
9. Jerger J,Jerger S. Clinical validity of central auditory tests. Scand Audiol. 1975, 4:147-163.
10. ISO 7029 (Second edition). Acoustics. Statistical distribution of hearing thresholds as a function of age (International Organization for Standardization, Geneva, 2000).
11. Borges ACLC. Adaptação do teste SSW para a língua portuguesa. Acta Awho. 1986, 5(suppl 1):38-40.
12. Pereira LD. Processamento auditivo central: abordagem passo a passo. In: Pereira LD, Schochat E. Processamento auditivo central: manual de avaliação. São Paulo: Lovise; 1997, p. 49-59.
13. Papaléo Neto M, Borgonovi N. Biologia e teorias do envelhecimento. In: Papaléo Neto M, Borgonovi N. Gerontologia: a velhice e o envelhecimento em visão globalizada. São Paulo: Atheneu; 2002. p. 284-96.
14. Fonseca CBF, Iório MCM. Aplicação do teste de lateralização sonora em idosos. Pró-Fono. 2006, 18(2):197-206.
15. Parra VM, Iório MCM, Mizahi MM, Baraldi GS. Testes de padrão de frequência e de duração em idosos com sensibilidade auditiva normal. Rev Bras Otorrinolaringol. 2004, 70(12):517-23.
16. Diveyi PL, Haupt KM. Audiological correlates of speech understanding deficits in elderly listeners with mild to moderate hearing loss. Ear Hear. 1995, 18:19-32.
17. Quintero SM, Marotta RMB, Marone SA. Avaliação do processamento auditivo central em indivíduos idosos com e sem presbiacusia por meio do teste de reconhecimento de dissílabos em tarefa dicótica - SSW. Rev Bras Otorrinolaringol. 2002, 68(1):28-33.
18. Soncini F, Costa MJ, Oliveira TMT. Influência do processo de envelhecimento no reconhecimento da fala em indivíduos normo-ouvintes. Pró-Fono. 2003, 15(3):223-230.
19. Rosa MRD. Processamento Auditivo (Central): estudo da escuta dicótica no processo de envelhecimento [mestrado]. Curitiba (PR): Universidade Tuiuti do Paraná-UTP; 2007.
20. Bellis TJ, Wilber LA.Effects of aging and gender on interhemispheric function. J Speech Lang Hear Res. 2001, 44:246-263.
21. Katz J, Ivery RG. Spondaic procedures in central testing. In: Katz J, editor. Handbook of clinical audiology. 4thed. Baltimore: Willians & Wilkins; 1994. p.239-55.
22. Bonaldi LV, Angelis MAA, Smith RL. Hodologia do sistema auditivo. In: Pereira LD, Schochat E. Processamento auditivo central: manual de avaliação. São Paulo: Lovise; 1997, p.19-25.
23. Silveira KMM, Borges ACLO, Pereira LD. Memória, interação e integração em adultos e idosos de diferentes níveis ocupacionais, avaliados pelos testes da avaliação simplificada e teste dicótico de dígitos. Rev Dist Comum. 2004, 16(3):313-318.
24. Zalcman TE, Schochat E. A eficácia do treinamento auditivo formal em indivíduos com transtorno do processamento auditivo. Rev Soc Bras Fonoauiol. 2007, 12(4):310-314.
25. Grafman J. Conceptualizing functional neuroplasticity. J Commun Disord. 2000, 33(4):346-355.
1 Doctor. Coordinator of the Master Degree Program in Communication Disorder at Tuiuti University of Paraná.
2 Master in Communication Disorders from Tuiuti University of Paraná Clinical Phonoaudiology.
3 Specialist in Clinical Audiology from Tuiuti University of Paraná. Clinical Phonoaudiology.
4 Doctor in Internal Medicine from UFPr. Professor and Coordinator of the Post-Degree Program in Internal Medicine and Health Sciences at UFPr.
5 Master in Communication Disorders from Tuiuti University of Paraná Assistant Professor of Phonoaudiology Degree at Tuiuti University of Paraná.
Institution: Tuiuti University of Paraná. Curitiba / PR - Brazil. Mailing address: Bianca Simone Zeigelboim - Rua Gutemberg, 99 - 9º andar - - Curitiba / PR - Brazil - ZIP Code: 80420-030 - Telephone: (+55 41) 3331-7807 - Email: bianca.zeigelboim@utp.br
Financial sponsorship: National Council for Scientific and Technological Development (CNPQ).
Article received on December 15, 2010. Article approved on February 5, 2011.

