INTRODUCTIONNoise-induced hearing loss results from injury to the ear due to exposure to noise, and its severity depends on both the intensity and exposure time and the susceptibility of the cochlea to noise (1). More precisely, the perception of deafness results from injury to the sensory cells of the inner ear (cochlea) (2).
Due to sound increases in the school environment in recent years, several studies have evaluated noise intensity at school, where children stay an average of 4 h per day (3). Although the Brazilian Technical Standards Association (ABNT) stipulates that the noise inside the classroom should not exceed a maximum of 50 dB (4), a study by Celani, Bevilácqua, and branches (5) found that the noise in the school environment can reach 94.3 dB.
METHODThis cross-sectional study was approved by the Committee of Ethics and Research Protocol on April 24, 2009 with CEP/UNITAU 062/09. The survey was conducted in the public school E.M.E.F. Prof. Álvaro, Marcondes with students in the sixth year of elementary school during the first half of 2009 from the following classrooms: B, 12 students; C, 7students; and D, 9 students. The questionnaires were delivered to the 30 parents of the students with the best and the worst notes of the 3 rooms without prior knowledge of the researchers as to each student's school. The questionnaire asked about any diseases the student had experienced in childhood, any for which they were still in treatment, any deafness-related diseases of family members, and the student's developmental history. A term of consent explained the instruments that would be used in the research and the expected results. Positive response to questions 6, 11, 12, and 13 of the questionnaire met the evaluation criteria of possible prior cochlear injury.
After the questionnaires were returned, students were subjected to an otoscopy exam to rule out other disorders of the external ear and cochlear function assessment carried out by means of acoustic emission analysis evoked by a distortion-product otoacoustic emission (DPOAE) using an Eroscan (Maico Inc, Minneapolis, MN, USA) at frequencies of 2, 3, 4, and 5 KHz in booth audiométrica.
On the day of the field research, students were isolated in a room and subjected to analyses carried out on 2 occasions: before entering the classroom at the start of the school day and soon after the end of the day. Measurements of noise inside the classroom were made using a digital sound level meter MSL-1325 MINIPA Ltda. (São Paulo) in 5 distinct locations (in 4 and ends in the Center). Between lessons, we also measured noise levels in places of recreation.
With the values obtained with the level meter was observed minimum and maximum intensity of noise inside the classroom with the presence of all students and in the forecourt, during the interval. We compared the initial and final DPOAE for the existence of possible changes suggesting cochlear injury after noise exposure at school, a value that was defined as being changed if there was no reply in 2 or more frequencies and worsened when one more frequently if present absent in the second exam. These data were crossed-referenced with the questionnaire responses regarding the students with the best and worst notes to define a pattern that can justify the difference between the school of the 2 groups plus a possible hearing loss.
RESULTSThe 28 students (13 females, 15 males) who participated in the study were 10-14 years of age. Most of the students (57.1%) were 11 years old and the average age was 11.11 (standard deviation = 0.916). These 28 students were divided by school performance: 14 (12 males, 2 females) had insufficient grades, while the other 14 (11 females, 3 males) had sufficient grades. According to the noise injury screening questions, 7 students did not meet any criteria, 9 students met criteria 1 and 7, students fill out 02 04 students meet criteria, criteria and only 03 01 students met all 4 criteria.
Chart 1 shows the minimum and maximum noise levels in classrooms B, C, and D, room B in the morning and rooms C and D in the evening, with all students present and noise inside the room where the test of acoustic emissions, outside audiométrica. Rooms B, C, and D had maximum values of 84.3, 96.2, and 93 dB and minimum values of 66.1, 71.1, and 67. 4 dB, respectively.
Chart 2 presents the maximum noise levels in the morning (83.8 and 88.7 dB) and evening (102 and 100 dB) intervals and the minimum noise levels in the morning (75.7 and 59.5 dB) and evening (78.6 and 79.7 dB) intervals in the courtyard during the school day.
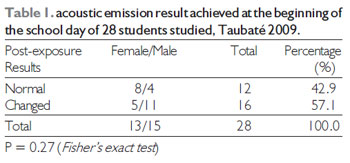
As shown in Table 1, of the 28 students surveyed, 16 (57.1%) showed some degree of change in the cochlear response in examination carried out at the beginning of the school day. Of these 16 students, 11 were male and 5 were female.
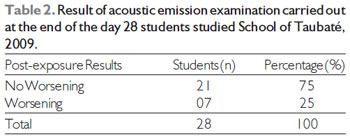
Table 2 shows that of the 28 students, 7 (25%) had worsened cochlear responses compared to the initial examination.
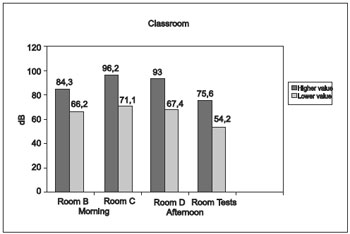
Chart 1. Intensity of noise in classrooms, Taubaté 2009.
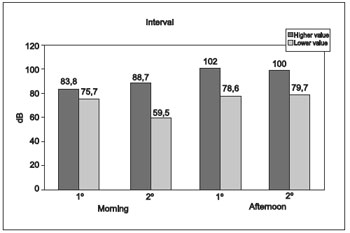
Chart 2. Intensity of noise during intervals, Taubaté 2009.
The numerous causes of sensorineural deafness made it necessary to administer a questionnaire to correlate noise with responses to acoustic emission examination of the students who participated in the study.
The questionnaire regarding noise injury included the following questions: Does your child watch TV at high volume? Does your child use an mp3 player at high volume? Is your child exposed to loud sounds from speakers? Has your child been exposed to loud noises such as exploding fireworks? A total of 9 students who met at least one criterion had insufficient grades, while a total of 7 students who responded to at least one criterion also experienced cochlear changes after acoustic emission. This finding may suggest that a well-crafted questionnaire may indicate hearing changes in patients with inadequate school.
Bacterial and viral infections, especially measles, mumps, and meningitis: his son had mumps, measles, or meningitis? Which one? Only 3 students, one in each room, had a history of infections (meningitis in 2, parotidites in one), all 3 of whom had insufficient grades. Cochlear 02 arrived with Amendment préexposição to school one day presented worsens post exposure. Such a questionnaire can help when researchers do not have the ability to administer auditory examinations.
Use of medications, particularly antibiotics, aminoglycosides and antineoplastic: his son was hospitalized and received antibiotics by vein for more than 3 days? Which the infection? Only 2 students in addition to the other disclosed infections had previously been given an antibiotic injection. Both were among the inadequately performing students.
You, the student's mother, had some infection diagnosed during pregnancy? There was some problem during pregnancy of this child? Only 4 mothers had gestational infections (urinary tract infection) and only those 4 experienced problems during childbirth. Of these students, 3 were in the insufficient group and all had cochlear problems-one before exposure and 3 after exposure.
Menière's disease: your child complains of dizziness or zonzeira? He has complained of noise or buzzing in the head? Since this question is subjective, we had difficulty interpreting the answers.
Parents were also asked whether they had to repeat themselves several times for their child to understand and whether their child frequently increased the TV volume.
Evoked otoacoustic emissions (EOAEs) are low-intensity noise energies that are amplified by contraction of the outer hair cells of the cochlea that may be captured in the external acoustic meatus in response to an acoustic stimulus (6). EOAEs are classified into 3 categories: transient or transient raised by a brief acoustic stimulus, usually a click, over a broad spectrum covering a range of frequencies; a DPOAE raised by 2 simultaneous pure tones (f1 and f2) that produce a distortion product (2f1-f2) by intermodulation; and a stimulus frequency raised by a continuous low-intensity signal matching the frequency of the presented stimulus. These are less used clinically as a result of your registration offer many technical difficulties and the time of examination be greater (7).
EOAE are recorded in the vast majority of individuals with normal hearing regardless of age or sex. Their presence indicates the integrity of cochlear mechanism and establishes whether the activity in the exposed ear is within normal limits regardless of patient intention or cooperation. Otoacoustic emission screening exposes fewer false positives and false negatives. Its speed, non-invasive nature, and accuracy make it a test with an ideal profile for screening programs (7).
Several factors can be related to the fact that 12 of the 14 students with insufficient grades were male. Studies report that boys tend to have lower school performance than girls because they are busier, have a lesser ability to concentrate, and mature more slowly than girls (6).
This work showed that the noise inside the 3 classroom of the studied school exceeded the recommended maximum values. The maximum values of rooms A, B, and C were 84.3, 96.2, and 93 dB, respectively, while the minimum values were 66.1, 71.1, and 67.4, respectively. Room C obtained maximum minimum values both as too superior rooms (96.2 -71.1) and the noise levels of all 3 studied rooms were above the value of 50 dB advocated by ABNT (4). The intensity found in this study was similar to that of CELANI et al. (5) and larger than that of SERAFINI et al. (8). However, compared to the study by REDDY et al. (9), whose peak values surpassed 100 dB (A) in series 3, the results of this study were minors.
The noise produced during the breaks was also excessive in both school periods (morning and evening) with maximum values reaching 88, 3BS in the morning and 102 dB in the afternoon, surpassing the Protocol of the Ministry of Health, which is 85 dB (1). However, the students were exposed to this noise level for approximately 20 min (interval length). The ABNT (4) states that exposure to noise levels e" 108 dB for 20 min results in cochlear injury. We did not study values exceeding this threshold during this evaluation, but we did identify that the hearing loss of 2 students from room B (in the morning) worsened in the acoustic emission examination at the end of the school day, while the hearing loss of a larger number of students of the evening period (room C, 4 students; room D, one student) worsened after exposure.
Studies show that excessive noise leads to stress, difficulty concentrating, neuropsychomotor development retardation, aggression, and low income (7). The noise found in classrooms and on the patio in this study compared with data from the Brazilian Society of Otorhinolaryngology show that the same noise levels (80-110 dB) are caused by heavy traffic, race cars, and underground trains (10), demonstrating that the values found in this study are not appropriate for the school environment, so little to the physical and mental health of children in this learning phases for the other school professionals.
Of the 28 students evaluated, 16 (57.1%) reported some degree of pre-existing hearing loss. Of these 16, 7 students had insufficient academic performance. It is possible that the school performance is related to the detected hearing changes. Also noted that these 6 replied that they were exposed to intense sound (i.e., they met at least one of the criteria for sound exposure). Considering these data and our limited number of samples, we cannot claim that these pre-existing changes are due to exposure to noise produced during a student's school life, but these findings did alert us to the fact that not only the noise inside the school but also the students' habits (e.g., using an mp3 player at high volume, exposure to loud music in discos, high-volume conversations) contributed to the detected hearing loss.
In the afternoon examinations, we found that the hearing of 7 students had worsened in relation to the first examination, all of whom were part of the group of 16 students who had pre-existing hearing loss. Of these 7 students with worsening hearing, 4 were male and 3 were female. Two were tested in the morning (room B), while the others were tested in the afternoon (4 in room C and one in room D). Of these students with worsening hearing, 07 04 03 boys and girls were; 02 were the morning period (room B), and the rest of the evening period (room C and 04 01 Student Room D). Room C had the highest noise intensity and, as expected, the largest number of students with worsening cochlear responses.
CONCLUSIONSThis study revealed the following:
-The noise produced in this school exceeds the recommended limits defined by ABNT and the Ministry of Health.
-Almost half (42.85%) of the students who showed worsening hearing in the acoustic emission examination had insufficient school performance.
-A good portion (25%) of the students showed worsening hearing in the acoustic emission examination after one-day exposure to noise at school.
BIBLIOGRAPHIC REFERENCES 1. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Perda auditiva induzida por ruído (PAIR). Série A. Normas e Manuais Técnicos. Brasília: Editora MS, 2006. Disponível em http://portal.saude.gov.br/portal/arquivos/pdf/06_0444_M.pdf.
2. Hungria H. Otorrinolaringologia. 8 ed. Rio de Janeiro: Guanabara Koogan, 2000.
3. Cruz OLM, Costa SS. Disacusias Neurossensoriais Induzidas por Ruído. In: Cruz OLM, Costa SS, Oliveira JAA. Otorrinolaringologia: Princípios e prática. Porto Alegre: Artes Médicas, 1994, 21:222-3. ABNT. Associação Brasileira de Normas Técnicas.
4. NBR 10152: Níveis de Ruído para conforto acústico. Rio de Janeiro: ABNT, dez 1987.
5. Celani AC, Bevilácqua MC, Ramos CR. Ruído em escolas. Fono: Rev. Atual. Cient. 1994, 6(2):1-4.
6. Dal'igna MC. Desempenho escolar de meninos e meninas: há diferença? Educ. Rev. 2007, 46:41-267.
7. Pialarissi P, Gattaz G. Emissões Otoacústicas: Conceitos Básicos e Aplicações Clínicas. Arq. Int. Otorrinolaringol. 1997, 1(2). Disponível em http://www.arquivosdeorl.org.br/conteudo/acervo_port.asp?id=13.
8. Serafini F., Moreira PAC, Santos ECC, Merotti FO, Bortoleto MS, Lenci R. Can noise induced hearing loss happen in elementary schools? Proceedings of XXX Congress of the NES. Oporto Portugal. 2003. Disponível em: http://www.neurootology.org/archives/22.
9. Ribeiro MER, Oliveira RLS, Santos TMM, Scharlach RC. A percepção dos professores de uma escola particular de Viçosa sobre o ruído nas salas de aula. Rev. Equilíbrio Corporal e Saúde. 2010, 2(1):27-45.
1) Undergraduate student.
2) Graduate in medicine school.
3) PhD Professor and Chair of the Department of Oto-Rhyno-Laryngologyat Taubate University Hospital -UNITAU.
Institution: Taubate University-Medicine School. Taubaté / SP - Brazil. Mailling address: Nelson de Almeida Filho - Rodovia Geraldo Scavone 1000, Lote 68 - Jacareí / SP - Brazil - Fax: (+55 12) 3951-8577 - E-mail: nelson_almeida41@hotmail.com
Article received in June 1st of 2011. Article approved in July 10th of 2011.