INTRODUCTIONPatients with noise-induced hearing loss (NIHL) frequently have several symptoms such as tinnitus, vertigo, gradual decreases or distortions in hearing, and alterations in speech comprehension. NIHL is irreversible and permanent; however, it is preventable with the use of hearing protectors during noise exposure. The magnitude of hearing loss that results from excessive exposure to noise depends on factors that are associated with the exposure, including sound pressure level, duration, type of noise, and frequency, and the characteristics of the individual being exposed, including susceptibility to NIHL, age, and prior history of hearing damage (1-4).
DIAS et al. evaluated 284 workers and found an NIHL prevalence of approximately 63% and that of tinnitus was approximately 48%; this study reported an association between noise-induced hearing loss and occupational noise (5).
OGIDO et al. previously reported that tinnitus was present in 80.81% of the population, and concluded that auditory dysfunction is frequent and that research and evaluation of hearing disorders using surveys of workers that were exposed to occupational noise is critical, as symptoms such as tinnitus can cause distress and negatively affect the quality of life of workers (6). In addition to occupational exposure, hearing loss, tinnitus, and dizziness have been associated with smoking, hypertension, diabetes, aging, health history, and leisure activities, and the incidence of ear symptoms appears to be correlated with noise exposure throughout life (1-3,7-9).
Presbycusis, which the third most common chronic condition that is reported by the elderly, can be defined as hearing loss associated with aging, thus reflecting the loss of auditory sensitivity associated with advanced aging. The typical audiometric profile observed clinically in presbycusis is symmetrical bilateral sensorineural high-frequency hearing loss that progresses with age, and the associated buzzing sound is a highly prevelant symptom that has a high impact on the quality of life of the elder patient (10-12).
A study by FERREIRA et al. (12) observed that tinnitus was a cause of intense dissatisfaction in elderly patients, as it impaired their daily activities and resulted in emotional and sleep disorders. This study found a correlation between the presence of hypertension in patients and tinnitus; however, a correlation between the degree of hearing loss and the level of audiometric discomfort that is felt by the patient has not been established.
The purpose of the present study was to assess the prevalence of tinnitus in elderly individuals with and without history of occupational noise exposure.
METHODThis cross-sectional study was carried out at Universidade Norte of Paraná (UNOPAR) in Londrina. The study protocol was approved by the bioethical committee of the UNOPAR University, with the approval number PP/0063/09. This was the first large, rigorous survey that examined 502 elderly individuals in this particular city. The subjects were sent by the Study on Aging and Longevity (EELO) project.
The anamnesis included questions about age, gender, hearing loss complaints, tinnitus, noise exposure history, and medical history. The audiological evaluation was performed individually in a soundproof booth with an interacoustics audiometer.
The variables that were studied included the frequency of tinnitus and the history of occupational noise.
Logistic regression was used to control for confusion or modification of the effects of other variables on the associations of interest. Confounding variables that had values of up to a 20% association with a history of occupational noise (in a univariate model) were included in the adjusted logistic regression model. The procedures were performed using Bio Stat software, version 5.0, while adopting a significance level of 5%.
RESULTSIn the present study, calculations of the sample results of 382 individuals were necessary to extrapolate the results found in the study population.
Considering possible losses of data during its collection, 519 patients were evaluated, of which 502 patients were included in the study and 17 patients were excluded from the study due to a lack of evaluation days.
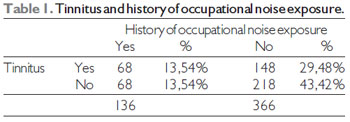
Of the 502 patients that were included in this study, 366 (72.90%) had no history of occupational noise exposure, and 136 (27.09%) had history of exposure to occupational noise.
Of the 502 subjects, 286 (56.97%) did not have tinnitus and 216 (43.02%) had tinnitus.
Among the 366 who were not exposed to occupational noise, 148 had tinnitus (40.43%) and 218 did not have tinnitus (59.56%).
Of the 136 subjects who were exposed to occupational noise, 68 (50%) had tinnitus and 68 (50%) had no tinnitus (Table 1).
Sixty-eight subjects (13.54%) had tinnitus and were exposed to occupational noise, 68 subjects (13.54%) did not have tinnitus and were exposed to occupational noise, 148 (29.48%) had tinnitus and were not exposed to occupational noise, and 218 (43.42%) had neither tinnitus nor exposure to occupational noise.
By using the chi-square test, we obtained a chi-square value of 3.699 (p = 0.0544), which indicated that there was not a significant difference between the subjects that were exposed to occupational noise and those that were not exposed with regard to tinnitus, when measured in subjects older than 60 years of age.
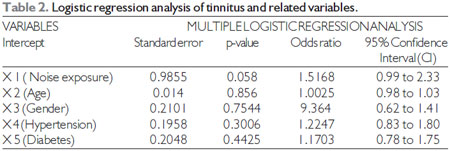
Multiple logistic regression analysis was also performed from the data of 498 subjects, which excluded patients who had not been assessed in the selected variables; tinnitus was the dependent variable (y) and noise exposure, age, gender, hypertension, and diabetes were the independent variables (x).
The results indicated that there were no significant differences between the independent variables (exposure to noise, p = 0.0580; age, p = 0.8560; gender, p = 0.7544; hypertension, p = 0.3006; and diabetes, p = 0.4425; Table 2).
DISCUSSIONData from a gerontological and geriatric study population in Sweden (13) indicated that the age-related deterioration of hearing is more pronounced in older men (between 70 and 75 years of age) that were exposed to noise compared with those that were not exposed to noise. However, a limiting factor to the differential diagnosis of hearing disorders in the elderly is that the hearing loss that is normally associated with aging tends to be confounded by the previous effects of noise exposure in individuals who worked in a noisy environment (11). In this study, the presence of tinnitus regardless of history of occupational noise exposure may be due to the accumulated noise exposure over time and other comorbidities in the elderly.
A lifetime of noise exposure increases the likelihood of negative effects on hearing, but it is difficult to determine the specific interactions between noise, alterations in hearing, and presbycusis, as presbycusis has a complex etiology that includes both intrinsic and extrinsic factors. The influence of noise on presbycusis has been postulated in numerous reports for nearly a century; however, is difficult to identify the noise exposure as a single factor for hearing impairment in elderly (4-14).
The possible correlations between hearing loss and history of occupational noise exposure in the elderly reveals a complex picture due to the variety of factors that are associated with aging.
It is difficult to determine whether hearing loss in the elderly is caused by general degeneration that is associated with aging.
Tinnitus, in which an individual perceives sounds that do not correspond with an external sound, is a symptom that is often reported in individuals that are exposed to high sound pressure levels, and several studies have reported that prolonged exposure to occupational noise can not only lead to a decrease in hearing, but also to tinnitus and hyperacusis. In addition, excessive exposure to noise is the most important risk factor for hearing impairment and the onset of tinnitus, followed by age and gender, and it has been recommended that tinnitus prevention should be included in hearing loss prevention programs to promote hearing health in potentially affected workers (16).
Given the high prevalence of hearing impairment in the elderly population and the differences between the groups, there is a clear need to understand its nature and causes in various populations to improve prevention and to develop intervention strategies (4-9,17).
CONCLUSIONThis study aimed to determine whether noise exposure was a potential causal factor for tinnitus in the elderly; however due to the aforementioned difficulty in defining the causes of hearing impairment in the elderly, the numerous comorbidities present in this population, and the degenerative nature of the aging process, there was no significant association between elderly individuals with a history of occupational noise and tinnitus. However, the similar high-frequency tinnitus that occurred in both populations regardless of history of occupational noise exposure shows the need to be aware of the prevalence of tinnitus among elderly individuals.
BIBLIOGRAPHIC REFERENCES 1. Marchiori LLM, Rego Filho E A, Matsuo T. Hypertension as a factor with hearing loss. Rev Bras Otorrinolaringol. 2006, 72(4):533-540.
2. Agrawal Y, Platz EA, Niparko JK. Risk factors for hearing loss in US adults: data from the National Health and Nutrition Examination Survey, 1999 to 2002. Otol Neurotol. 2009, 30(2):139-145.
3. Collee A, Legrand C, Bernadette Govaerts, Van Der Veken P, Boodt F, Degrave E (2011). Occupational exposure to noise and the prevalence of hearing loss in a Belgian military population: A cross-sectional study. Noise & Health. 2011, 13: (50) 64-70.
4. Marchiori LLM, Melo JJ, Meneses CL. Comparison of hearing loss in Elderly with and without history of occupational noise exposure. Proceeding of the 10th International Congress on Noise as a Public Health, London, 2011.
5. Dias A, Cordeiro R, Corrente JE, Gonçalves CGO. Associação entre perda auditiva induzida pelo ruído e zumbidos. Cad Saude Publica. 2006, 22(1):63-8.
6. Ogido R, Costa EA, Machado HC. Prevalência de sintomas auditivos e vestibulares em trabalhadores expostos a ruído ocupacional. Rev Saúde Pública. 2009, 43(2): 377-380.
7. Jokitulppo J, Toivonen M, Björk E (2005). Estimated leisure-time noise exposure, thresholds, and hearing symptoms of Finnish Conscripts. Mil Méd. 2006, 171:112-116.
8. Marchiori LLM, Rego Filho EA. Queixa de vertigem e hipertensão arterial. Rev. CEFAC. 2007, 9(1):116-121.
9. Poli-Frederico RC, Marchiori LLM, Melo JJ, Carvalho LL. Possible identification of Noise-Induced Hearing Loss susceptibility genes.Proceeding of the 10th International Congress on Noise as a Public Health, London, 2011.
10. Lethbridge-Cejku M, Schiller JS, Bernadel L. Summary health statistics for U.S. adults: National Health Interview Survey. Vital Health Stat. 2004, 10(222).
11. Krishnamurti S. International Journal of Environmental Research and Public Health. 2009, 6(3):889-899.
12. Ferreira LMBM, Ramos Júnior AN, Mendes E P. Caracterização do zumbido em idosos e de possíveis transtornos relacionados. Rev Bras Otorrinolaringol. 2009, 75(2):245-248.
13. Gates AG, Schmid P, Kujawa SG, Nam B, D'Agostino R. Longitudinal threshold changes in older men with audiometric notches. Hear Res. 2000, 141(1-2):220-228.
14. Rosenhall U. The influence of ageing on noise-induced hearing loss. Noise and Health Year. 2003, 5(20):47-53.
15. Mattos LC, Veras RP. The prevalence of hearing loss in an elderly population in Rio de Janeiro: a-sectional study. Rev Bras Otorrinolaringol. 2007, 73(5):654-59.
16. Steinmetz LG, Zeigelboim BS, Lacerda A B, Morata T C, Marques J M. Características do zumbido em trabalhadores expostos a ruído. Rev Bras Otorrinolaringol. 2009, 75(1):7-14.
17. Pratt SR, Kuller L, Talbott EO, McHugh-Pemu K, Buhari AM, Xu X. Prevalence of Hearing Loss in Black and White Elders: Results of the Cardiovascular Health Study. Journal of Speech, Language, and Hearing Research. 2009, 52: 973-89.
1) Master. Speech Therapy Course Coordinator - UNOPAR/North Parana State University.
2) Master Student of Rehabilitation Science UNOPAR/UEL - North Parana State University/Londrina State University. Clinical Speech Therapy.
3) Ph.D. in Medicine and Health Science/ UEL. Professor for Mastering Course in Rehabilitation Science at UNOPAR/UEL- North Parana State University/Londrina State University.
Institution: North Parana State University - UNOPAR. Londrina / PR - Brazil. Mailing address: Campus Universitário de Londrina (Clinica de Fonoaudiologia - UNOPAR) - Paris Avenue, 675 - Londrina / PR - Brazil - Zip-code: 86041-140 - Caixa Postal: 401 - Telephone: (+55 43) 3371-7775
Article received in October 10, 2011. Article approved in October 26, 2011.