INTRODUCTIONThe hearing loss, which prevents the elder to fully play his or her role in the society, is one of the most incapacitating communication disturbances.
Presbyacusis is the hearing sensitivity loss resulting from aging. It is characterized for being bilateral for high-frequency sounds, due to the degenerative and physiologic change of the hearing system (1), followed of a decrease in the speech distinguishing (2). Taking into account the hearing deficiency prevalence is extremely high, and reaches 84.2% of the elders (3), this is taken as a public health problem. The peripheral sensitivity loss is highly correlated with the cognitive decline in elders (4,5). The presbyacusis affects the capacity for the elders' daily life activities and increases the risk of functional decline. Many times, before a patient with a severe disease, such deficiencies are disregarded, which makes the rehabilitation process seriously difficult (6).
When the relationship between the cognitive performance and hearing loss is considered, by using the Mini-Mental State Examination (MMSE), the researchers showed the elders with moderate to severe hearing loss have lower scores that the elders without hearing loss (7).
In another study, carried out to determine what causes low scores in the MMSE test, except for dementia, the authors concluded that, in 10% of the sample components, the visual and hearing changes and low education degree were the main responsible for lower scores (8).
Studies on the use of hearing aids influence to the cognitive performance were also accomplished. They showed the rehabilitation provided the cognitive global measurements an improvement (9) and that the relatives also realized an enhancement in the attention, reversion of the social isolation and the communicative and emotional difficulty, which therefore contributed for an improvement in the quality of life (10). However, another study revealed the use of hearing aids by elders didn't influence their cognitive performance (11).
An analysis carried out with a group of people with the initial phase Alzheimer disease verified the hearing abilities were affected compared to the results of a control group in the same age range but without the disease (12).
This is thus important to know the relations between the hearing loss and cognitive disturbances, specially in the elders, since generally there are no complaints in the early period. As a result, diagnoses and interventions are not made, but the effects may be significant. This is a complex area because both a neuropathology may jointly determine cognitive and sensorial deficiencies, and the chronic sensorial deficiency, regarding the non-intervention, may make the cognitive deficiency more severe (13).
According to theoretical assumption described, the objective of this study is to verify if there is a relationship between, hearing, age, sex, education and the cognitive performance in a non-institutionalized group of elders.
METHODThe research is of transversal and observational drawing. The sample was composed by 33 non-institutionalized elders who were submitted to auditory assessment in a Phonoaudiology College Clinic. The individual aged 60 years or older was considered to be elder (14).
The participants in the study were invited to take part of the research after the performance of the audiologic assessment. Those who accepted to take part, signed an Free and Clarified Authorization Term and responded to the MMSE. The audiologic evaluation results were obtained in the Clinic College records.
In order to determine the degree of hearing loss, the classification of Davis and Silvermann (15) was used (15). It consists of the tonal thresholds average for frequencies of 500, 1000 and 2000Hz. The results deemed to be normal were from 0 to 25 dB NA; light loss, from 26 to 40 dB NA; moderate, from 41 to 70 dB NA, severe, from 71 to 90 dB NA; and deep loss, over 91 dB NA.
The MMSE was applied always by the same examiner. The results analysis was made based on the MMSE evaluation protocol (16, 17). The test is composed by several questions grouped into seven categories, each one aimed at assessing the specific cognitive functions: time orientation (5 points); 3-word register (3 points); attention and calculation (5 points); 3-word recalling (3 points); language (8 points); visual constructive capacity (1 point). The test consists of questions and commands to be performed by the patient. The MMSE score may vary from a minimum of 0 until a total of 30 points, the addition is made after the exam completion. Results lower than 24 points indicate a cognitive deficiency (16).
The data were inserted in the SPSS software version 10.0. Statistical techniques used were descriptive such as simple frequency transversal tables and the Kappa concordance coefficient. For comparison between the MMSE and the loss degrees, the non-parametric test of Kruskal-Wallis was used. For education comparison the Mann-Whitney test was used.
The research was approved by the Ethics Committee in the University Research, under protocol 166h.
RESULTSThe data analysis confirmed that out of the 33 (100%) elders assessed, 20 (60.6%) were men and 13 (39.4%) were women. The ages ranged from 60 to 82 years: 16 (43.4%) were between 60 and 69 years; 15 (45.4%) between 70 and 79 years; and 2 (6.06%) between 80 and 82 years of age.
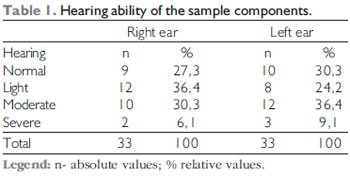
From the 66 ears evaluated, we confirmed that, in both ears, normal auditory thresholds were obtained (RE -27.3%, LE - 30.3%) and light hearing losses (RE - 36.4%, LE - 24.2%), moderate (RE - 30.3%, LE - 36.4%) and severe (RE - 6.1%, LE - 9.1%) (Table 1). We confirmed that most elders assessed presented with normal auditory thresholds or hearing loss of light or moderate degree.
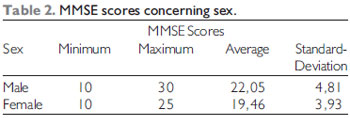
Table 2 contain the analysis data from the results obtained in the MMSE concerning sex. The male sex individuals achieved the minimal value of 10 and maximal of 30. The average of hits for the responses was of 22.05. The women presented at least 10 and at most 25 hits, with an average of 19.46.
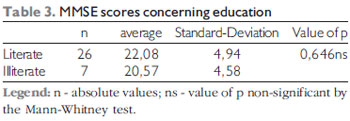
As shown in the data of Table 3, 26 (78.7%) elders were literate and 7 (21.3) were not literate. The data analysis confirmed the education didn't influence the scores obtained, which differs from most researches carried out.
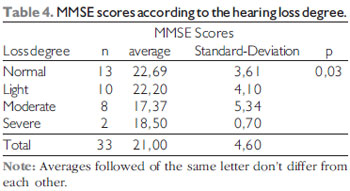
In order to verify the relationship between the individuals hearing loss and the cognitive performance, an analysis was performed, that considered the degree of hearing loss in the best ear and the average of scores obtained in the MMSE. The results are presented in Table 4. It was verified that the elders with normal hearing thresholds or light degree hearing loss in the best ear presented significant better scores that those with moderate or severe degree hearing loss.
Graphic 1 contain the analysis of results obtained in the MMSE concerning age. Such findings confirm that the older the patient, the worse is the performance in the test, that is, age may influence in the MMSE. Despite there is a gradual diminishing on the scores with the increase of age, the differences are not significant. This may be explained by the low number of individuals in the age range of 80 years.
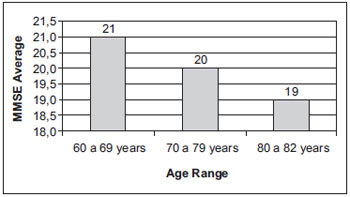
Graphic 1. MMSE results concerning age.
As for the degree of hearing loss of the samples individuals, the results are similar to those obtained by other authors (2, 18, 19, 20, 21), that is, most elders evaluated presented with normal auditory thresholds or light or moderate hearing loss. This degree of hearing loss doesn't fully prevent the individual from perceiving the environmental sounds, but generates a series of disorders, since the speech is hardly understood and may cause social life avoidance, and seriously affects the individuals' cognitive performance.
As for the sex, despite the elderly women obtained lower scores than men, the analysis of the results confirmed this variable didn't influence the MMSE results. Such data are similar to those obtained by other authors (17, 22), but differ from the findings of other ones (23). This difference between the studies may be explained by the size of the sample.
Since some individuals in the sample were not literate and that the literature research (24) confirms education influences the scores obtained, we opted for an MMSE results analysis also according to the education of the sample components. Differently from predicted, the education didn't influence the results obtained. Maybe this difference found concerning the several researches is explained by the low level of education of the literate elders. We confirmed that most of them had incomplete elementary school, having received only two or three years of regular schooling, which didn't differ them significantly from the illiterate individuals. In case elders with a higher education level had been included in the sample, maybe this variable would have influenced the results significantly.
When the presence and degree of hearing loss were considered, we confirmed that, in the elders assessed, the hearing loss was one of the factors that related to the MMSE scores diminishing, which enables to state that there is a significant relationship between the elders hearing loss and cognitive performance, and confirms prior studies (7, 8).
The gradual hearing loss, as in the case of presbyacusis, leads to a growing difficulty in oral communication and to consequent social isolation, with implications to cognition (10, 25). The forwarding for hearing aids selection and fitting is, therefore, important, since, as the hearing loss is associated to a cognitive worsening, the rehabilitation may be connected to the global improvement to the cognitive measurements (9, 10).
CONCLUSIONIn this work sample findings, the individuals with light and moderate degree hearing loss presented with better scores in the MMSE than those with severe and deep degree hearing loss. Therefore, we conclude there is a relationship between hearing loss and cognitive performance. The other variables studied (age, sex and education) didn't influence the tests' scores.
BIBLIOGRAPHICAL REFERENCES1. Huang T. Age-related hearing loss. Minn Med. 2007, 90 (10): 48-50.
2. Pinheiro MMC, Pereira LD. Processamento auditivo em idosos: estudo da interação por meio de testes com estímulos verbais e não verbais. Rev Bras Otorrinolaringol. 2004, 70(2): 209-14.
3. Béria JU, Raymann BCW, Gigante LP, Figueiredo ACL, Jotz GP, Roithmann R et al, Hearing impairment and socioeconomic factors: a population-based survey of na urban locality in southern Brazil. Pan Am J Public Health. 2007, 21(6): 381-7.
4. Martin JS, Jerger JF. Some effects of aging on central auditory processing. JRRD. 2005, 42 (4): 25-44.
5. Pichora-Fuller MK, Stingh G. Effects of age on auditory and cognitive processing: implications for hearing aid fitting and audiologic rehabilitation. Trends in Amplification. 2006, 10(1): 29-59.
6. Monego ET, Costa EFA. Avaliação geriátrica ampla. Revista da UFG. 2003, 5(2): 11-5.
7. Tay T, Wang JJ, Kifley A, Lindley R, Newall P, Mitchell P. Sensory and cognitive association in older persons: findings from an older australian population. Gerontology. 2006, 52: 386-94
8. Räihä I, Isoaho R, Ojanlatva A, Viramo P, Sulkava R, Kivelä SL. Poor performance in the mini-mental state examination due to causes other than dementia. Scand J Prim Health Care. 2001, 19(1): 34-8.
9. Allen NH, Burns A, Newton V, Hickson F, Ramsden R, Rogers J et al. The effects of improving hearing in dementia. Age Ageing. 2003, 32(2): 189-93.
10. Silva AS, Venites JB, Bilton T. A relação entre o uso do aparelho de amplificação sonora individual - AASI - e a melhora da função cognitiva no envelhecimento. Distúrb Comun. 2002, 14(1): 63-89.
11. van Horen SAH, Anteunis LJC, Valentjin SAM, Bosma H, Ponds RWHM, Jolles J et al. Does cognitive function in older adults with hearing impairment improve by hearing aid use? Int J Audiol. 2005, 44: 265-71.
12. Azevedo T, Ribas A. Estudo comparativo do teste SSW em indivíduos com e sem a doença de Alzheimer. Fonoaudiologia Brasil. 2004, 1(5): 1-3.
13. Valk HMJ, Haveman MJ, Maaskant MA, Kessels AGH, Urlings HFJ, Sturmans F. The need for assessment of sensory functioning in ageing people with mental handicap. J Intellectual Dis Res. 1994, 38(3): 289-98.
14. Pereira RJ, Cotta RMM, Priore SE. Políticas sobre envelhecimento e saúde no mundo. In: Pessini L, Barchifontaine CP. Bioética e Longevidade Humana. São Paulo: Loyola, 2006. p.289-307.
15. Davis H, Silvemann RS. Hearing and Deafness. New York: Holt, Rinehart e Winston, 1970.
16. Folstein MF, Folstein SE, McHugh PR. Mini-mental State: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J Psychiatr Res. 1975, 12: 189-98.
17. Almeida OP. The Mini-mental state examination and the diagnossi of dementia in Brazil. Art Neuro-Psiquiatr. 1998, 56(3): 605-12.
18. Amaral LCG, Sena APRC. Perfil audiológico dos pacientes de terceira idade atendidos no Núcleo de Atenção Médica Integrada da Universidade de Fortaleza. Fono Atual. 2004, 27(7): 58-64.
19. Baraldi GS, Almeida LC, Borges ACLC. Perda auditiva e hipertensão: achados em um grupo de idosos. Rev Bras Otorrinolaringol. 2004, 70(5): 640-4.
20. Teixeira AR, Freitas CLR, Millão LF, Gonçalves AK, Becker Jr B, Vieira AF et al. Relação entre perda auditiva, idade, gênero e qualidade de vida em idosos. Arq Int Otorrinolaringol. 2008, 12(1): 62-70.
21. Teixeira AR, Almeida LG, Jotz GP, De Barba MC. Qualidade de vida de adultos e idosos pós adaptação de próteses auditivas. Rev Soc Bras Fonoaudiol. 2008, 13(4): 357-61.
22. Küçükdeveci AA, Kutlay S, Elhan AH, Tennant A. Int J Rehabil Res. 2005, 28(1): 77-9.
23. Rait G, Fletcher A, Smeeth L, Brayne C, Stirling S, Nunes M et al. Prevalence of cognitive impairment: results from the MRC trial of assessment and management of older people in th community. Age Ageing. 2005, 34(3): 242-8.
24. Launer LJ, Dinkgreve MA, Jonker C, Hooijer C, Lindeboom J. Are age and education independent correlates of the Mini-Mental State Exame performance of community-dwelling elderly? J Gerontol. 1993, 48(6): P271-7.
25. Britto PR, Cabral JE. O papel da educação no miniexame do estado mental: um estudo no nordeste do Brasil. Arq Neuro-Psiquiatr. 2004, 62(2): 206-11.
26. Kasper JD, Phillips CL. Physical disability and social interation: Factors associated with low social contact and home confinement in disabled older women. Jornal of Gerontology. 1998, 53B: S209-17.
1. Specialist in Audiology (IPA - RS). Clinical Phonoaudiologist.
2. Doctoral Degree in Biomedical Gerontology (PUCRS) Audiology Laboratory Phonoaudiologist (RS)
3. In Course for Doctoral Degree in Medical Sciences: Pediatrics (UFRGS). Clinical Phonoaudiologist.
Institution: Universidade Luterana do Brasil (ULBRA). Canoas / RS - Brazil.
Mail address:
Adriane Ribeiro Teixeira
Praça Dom Feliciano, 26 cj.604 Centro
Porto Alegre / RS - Brazil - Zip code: 90020-160
Telephone: (+55 51) 3028-9610
E-mail: adriteixeira@yahoo.com.br
Article received on January 08, 2008.
Approved on February 09, 2009.