INTRODUCTIONThe OSAS presents a large variety of symptoms, and the most important are snoring (in 90% of the cases), excessive daily somnolence, humor change, morning headache, sexual impotence, reduction of intellectual efficiency and cardiologic and neurologic changes. It is characterized by the occurrence of apneas and hypopneas (at a number of 5 or more per hour), due to the stop or reduction of the air passage through the upper airways with minimal duration of 10 seconds, and occurs many times and exclusively during sleep (1,2).
The polissonography is the choice exam and has the feature of classifying the OSAS and is therefore the essential exam for the choice of the procedure to be used in each case, by means of the determination of the number of times the respiratory events occur, which is called apnea-hypopnea index per hour (AHI) and 5 is the normal quantity (4).
The treatment of OSAS may be clinical or surgical and is directly related to the AHI determination. In the patients with AHI up to 15, the behavioral measures, such as losing weight, avoiding the use of alcohol and sedatives, quitting smoking, must be considered important auxiliary methods in the treatment (1). The clinical treatment mostly used nowadays is the application of mask, with positive pressure in the upper airways connected to an air compressor: nasal continuous positive airway pressure (CPAP). This method was introduced by Sullivan (5) in 1981 and became the most popular treatment for OSAS. The ideal pressure, that must vary according to the individual nasal resistance, size of the upper airways and acceptance of the volumetric analysis pressure, is between 5 and 15 cm H2O and its use for a long period depends upon the patient's adhesion (6).
Apnea and snoring respond well to CPAP in patients with AHI>30, because they have an immediate improvement and tolerate the use of mask (2). The fitting and comfort of the mask associated to the CPAP pressure adequate determination are the most influential factors for the treatment efficacy (7).
The use of CPAP is a very efficient method, but with adhesion problems. The collateral effects relate to the mask and the pressure, as well as the equipment noise, which influences in this method acceptance. Nasal obstructive diseases (chronic rhinitis, hypertrophic rhinitis, rhinosinusitis and nose septal deviation) may increase the pressure for the use of the CPAP, cause discomfort and require a treatment to ease the equipment tolerance. Nasal congestion may be the primary reason for the treatment interruption. The surgical correction may be used in patients who will further receive the CPAP, since the success of this therapy requires a relatively patent upper airway (8, 9). The patients must interrupt the treatment when they have infection of the upper airways due to the nasal obstruction, as well as use nasal depletion components to facilitate the tolerance to the CPAP (10).
Due to the abovementioned fact that the nasal obstruction is an important aspect for the non-acceptance of the CPAP treatment, the use of devices for dilatation of the nasal valve has been recommended by several authors, with a significant reduction of the snoring noise level (11,12). Such dilatation may be carried out with external or intranasal device, with relative effects to snoring reduction, but it does not reduce the number of apneas and hypopneas and does not improve oxygen saturation (12).
The use of intranasal dilator is not effective in patients with moderate or severe OSAS, because the nasal resistance reduction doesn't prevent hypopharyngeal obstruction (13).
With the abovementioned fact the pressure is an important factor for the treatment acceptance, the objective of this article is to determine the CPAP pressure diminishing with the use of metallic intranasal dilator ("RINOSTENT") in patients selected with the sleep apnea-hypopnea syndrome being treated.
METHODThe patients in this study were forwarded to CPAP services (Sleep Institute and Hospital CEMA) and private clinics (Clínica Ademir Baptista and Hospital Paulista). They were all being treated with CPAP for a period of at most 6 months, with problems of adhesion or not, between November 2003 and June 2006. They were evaluated with clinical history, otorhinolaryngological exam and of nasal cavities with rigid telescope of the STORZ trademark of 30o with 4mm thick.
After evaluation of the patients forwarded by the assistant doctors, the inclusion criteria were: being in therapy with CPAP, with problem of adhesion or not, pathology severity and CPAP pressure volumetric analysis. The result was the selection of 30 patients out of whom 15 were excluded due to lesions in the nasal cavity (nose septal deviation for trauma, polyps and/or other tumors, strong hypertrophy of the nasal turbinates), buccal cavity (strong hypertrophy of palatine tonsils) and in the rhinopharynx (tumors), craniofacial malformations and syndromes with specific treatments, due to the primary impossibility to use CPAP as treatment, with the authorization of the assistant doctor they were sent for evaluation by an otorhinolaryngologist and/or buccomaxillofacial surgeon.
Figure 1. Rinostent - Metallic intranasal dilator.
We included 15 patients aged between 32 and 68 years divided into two groups: Group 1 - ten patients with complaint in the treatment with CPAP, namely: discomfort with the mask or pressure, nasal or oropharyngeal discomfort (dry mouth) and Group 2 - five patients without any complaint with the use of CPAP.
We then placed the intranasal metallic dilator into both nasal cavities to perform the new polissonography for pressure volumetric analysis. We used an intranasal metallic dilator patented with the name RINOSTENT, aiming at increasing the opening of the nasal valve. This product is a model similar to other dilators, by produced in silver alloy in a double spiral shape with central arc for expansion of the nasal vestibule diameter.
We did not include patients who had lesions in the nasal cavity (nose septal deviation for trauma, polyps and/or other tumors, strong hypertrophy of the nasal turbinates), buccal cavity (strong hypertrophy of palatine tonsils) and in the rhinopharynx (tumors), craniofacial malformations and syndromes with specific treatments, due to the impossibility to use the CPAP.
The patients signed an informed authorization and the research project was approved by the Ethics Committee in Research of the Hospital Heliópolis, registered under no. 266.
Upon arrival at the sleep laboratory, the patients were received by the technician, who checked the data and the exam prescription requested by the doctor and sent to the room. The patients filled in a pre-sleep questionnaire, with personal information and on their OSAS-related problems, they changed their clothes and were informed that their sleep would be monitored during the night by means of an audio and video monitor.
We placed electrodes to register the electroencephalogram, according to the International System 10-20 of Electrodes Placing; two electrodes for registering ocular movements, that were one at 1 cm above and out of the external corner of the right eye and another 1 cm below and out of the external corner of the left eye; two electrodes in the mental and submental regions; one electrode in each leg, on the respective anterior tibial muscle for registering the electromyogram and electrodes applied to the thorax, and oblique derivation was suggested (V1 modified): above on the right / below on the left for the electrocardiogram. A cannula was placed under the nose of the patient so that it was possible to capture the adequate signal of the air pressure of both nostrils. We put elastic belts on the thorax and abdomen for register of the respiratory effort. A vibration sensor (or microphone) was placed besides the trachea (thyroid cartilage) to register snoring. A sensor for research of oxymetry was put on the index finger.
Placement of the continuous positive airway pressure device (CPAP)We explained to the patients how the device works, possible discomforts, the previous placing of the intranasal dilator and that the mask should be fit on the face, without disturbing to avoid air leakage, that both inspiration and expiration should be made only by the nose, the mouth breathing and speaking would be difficult, which is normal, and that breathing should be natural and not forced by the device. We requested that the patients warned us on any discomfort and that they could remove the trachea if they felt asphyxiated and in this case they should inform the technician.
The standard method was proceeded for adjustment of the continuous PAP device pressure (CPAP), with initial pressure of 4 cmH2O and, after the beginning of sleep it would be increased one by one cmH2O, mechanically or automatically in case of apnea, hypopnea, snoring, awakenings or saturation of oxygen below 90%, the pressure should not exceed 18 cmH2O, under the watching of a professional.
The statistical analysis was made by method ANOVA (continuous independent and dependent variables and ANCOVA (categorical over dependent variables).
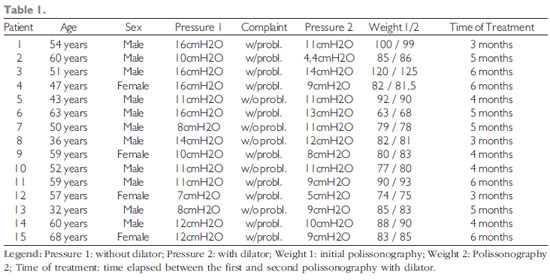
RESULTSThe evaluation with new polissonography was made without difficulties. Table 1 include the patients who presented some type of complaint in the treatment with CPAP, such as: Discomfort with the mask or the pressure, nasal or oropharynx discomfort (dry mouth) and the patients with no complaint; the initial and final pressures of the nasal dilator, the time of treatment did not exceed 6 months and the weight did not presented much importance due to the low variation through the therapy discontinuity (group 1). All patients with complaints had the pressured diminished after the use of the dilator.
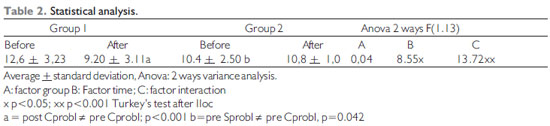
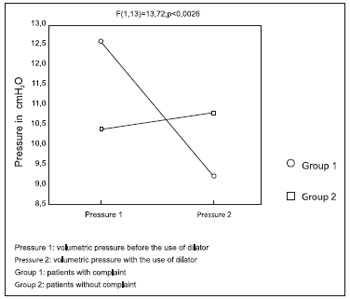
In Table 2 we find the statistical analysis showing the reduction of the pressure levels after the use of the dilator in Group 1 and practically no change in Group 2.
Once the groups started the treatment of different thresholds, namely: Pre Sprobl ¹ pre Cprobl; p = 0.042, the Ancova test was used and showed: F (1.12) = 10.005 p < 0.001.
The covariance analysis (Ancova) is commonly described for the adjustment of variables that cannot be controlled by the researcher.
DISCUSSIONThe CPAP therapy was introduced by Sullivan (5) in 1981 and has become the most popular treatment for OSAS, specially in the patients who did not accept surgery, have no clinical conditions for surgical treatment or need an immediate improvement of symptom, such as, excessive somnolence. The patients must be observed in sleep laboratory to determine the ideal pressure value to improve the snoring and apnea. The ideal pressure is between 5 and 15 cmH2O and must vary according to individual nasal resistance, size of VAS and acceptance of volumetric analysis pressure. The use of CPAP for a long period of time depends on the patient's adhesion.
In an important retrospective preliminary study, Wigand, Zwillich (1994) (6), reported that 60 to 90% of the patients with OSAS state regular use of CPAP in the first months of treatment and that the patients who abandon the use do it also in the first months due to collateral effects, inconvenience and perception of inefficacy.
The acceptance of the CPAP is parallel with the OSAS severity, and the higher it will be the more apneas occur and the longer the respiratory stoppage takes. The acceptance increases when excessive day somnolence is present (14,15).
By means of nasal mask during the night, the use of CPAP allows for air injection into the pharynx that unblocks and maintains the VAS permeable. The CPAP improves the day somnolence and the cardiopulmonary sequels. It represents the first treatment choice in the OSAS, mainly in the most severe forms, but its long-term use causes an inconvenience because it's uncomfortable, is not curative and leads to nasopharyngeal changes (1). Many patients do not adhere to the treatment with CPAP for many reasons: discomfort with the mask, with the air pressure in the nose and the noise of the device (9).
The CPAP high volumetric pressure in the sinuses of the face may reduce the draining and cause problems in patients with preexisting pathologies. Volumetric pressure higher that 10 cmH2O is related to the decrease in the cardiac frequency and renal function (5).
The minor complications of the CPAP are: skin irritation, dryness of the nasal and oropharyngeal mucosa, nasal congestion and secretion and ocular irritation. The major are: Pneumoencephalus, bacterial meningitis, severe epistaxis and atrial arrhythmia. The success of the CPAP therapy requires a patent airway (8).
Frequent reports from patients who use CPAP include: rhinorrhea and nasal irritation, epistaxis, headache, eyes irritation and inflammation, claustrophobia, irritation and perforation of the nasal septum due to the pressure in the mask (16).
The nasal surgery has a limited efficiency in the treatment of adults with OSAS, but improves the tolerance for the use of CPAP (3, 14).
The level of pressure of CPAP has a significant reduction after surgery for nasal obstruction correction, and increases the use of CPAP (9).
The nasal maximum resistance is located in the area of the valve that comprises the anterior part of the inferior turbinate (15).
In patients with sleep apnea-hypopnea syndrome, Schonhofer et al (2000) researched the effect of a plastic device to dilate the nasal valve (Nozovent), by introducing it in the nostril during the sleep so as to exert a forced dilation of the nasal valve. They carried out polissonography before and after one month of treatment and the research confirmed that the nasal dilator did not have any effect in patients with sleep apnea syndrome.
Rombaux et al. (2005) stated that the use of nasal dilator is an attractive method for the reduction of resistance in the nasal valve area, and has a positive impact on snoring and/or apnea. The nasal valve dimension is increased in approximately 30%. Two devices are commercialized with nasal dilators: Nozovent (internal) and Breathe Right (external). Most studies have concluded the nasal dilator may reduce the snoring subjective sensation, but without effect on the objective measure of the snoring and on the index of apnea-hypopnea in most patients with sleep respiratory disorders. Based on such information, the nasal dilator has no effect on most patients with apnea, but may be recommended as a test for patients with snoring and without apnea.
As the CPAP volumetric pressure is an important factor for acceptance and use by the patient, because high pressures (above 15 cm H2O) tend to bring collateral effects, any procedure able to diminish the pressure will be very helpful for the treatment of OSAS (10,12).
In this study, as a way to attenuate the CPAP pressure collateral effects and able to improve the adhesion to the treatment (since pressure is equal to force on surface), 15 patients were submitted to the new pressure volumetric analysis by means of polissonography performed with the use of an intranasal metallic dilator (Rinostent), previously adapted to each patient examined for inclusion in the study, by considering that an increase on the surface diminishes the pressure.
In this group, ten patients presented with some problem for the use of the CPAP (Group 1) and five had no complaint (Group 2). The pressure reduction was the only parameter to be analyzed as a means to evaluate before and after the use of the intranasal dilator. Data such as weight before and after were taken note of and showed that, in patients with adhesion problems and possible discontinuity of the CPAP treatment, it had no important variation while in the group without problems we noted a tendency for diminishing.
In the group with adhesion problem, all had a volumetric pressure diminishing with the use of the dilator; in the other group, without adhesion problems, two patients had no pressure change, but they reported major comfort in the use of the mask with the intranasal dilator; two patients had an increase on the pressure and in a prior evaluation we concluded there was a problem in the placing of the dilator on the day of exam; one patient presented a reduction to the pressure level.
CONCLUSIONThe use of the intranasal metallic dilator in patients with sleep apnea-hypopnea syndrome, under treatment and with adhesion problems, the CPAP volumetric pressure decreases.
BIBLIOGRAPHICAL REFERENCES1. Pinto JA. Síndrome da apnéia obstrutiva do sono: uma tarefa multidisciplinar. In: Pinto JA. Ronco e apnéia do sono. Rio de Janeiro: Revinter; 2000, pp.1-2.
2. Aloe F. Distúrbio respiratório sono-dependente. In: Pinto JA. Ronco e apnéia do sono. Revinter; 2000, 5:21-32.
3. Sériès F, Pierre S ST, Carrier G. Effects of surgical correction of nasal obstruction in the treatment of obstructive sleep apnea. Am Rev Respir Dis. 1992, 146:1261-5.
4. Mekhitarian L, Fava AS, Lopes HC, Stamm A. Estudo epidemiolócico das alterações estruturais da cavidade nasal associadas à síndrome da apnéia e hipopnéia obstrutiva do sono (SAHOS). Rev Bras Otorrinolaringol. 2005, 71:464-6.
5. Sullivan CE, Issa FG, Jones MB, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981, 18:862-5.
6. Wigand L, Zwillich CW. Disease a Month - Obstructive Sleep Apnea. Mosby - Year Book Inc. 1994, 40:199-252.
7. Silva AB, Lopes EA. Distúrbios do sono. Rev Bras Med. 2001, 58:225-35.
8. Man GCW. Obstructive sleep apnea - diagnosis and treatment. Med Clin North Am. 1996, 80:803-21.
9. Friedman M, Tanyeri H, Lim JW, Landsberg R, Vaidyanathan K, Caldarelli D. Effect of improved nasal breathing on obstructive sleep apnea. Otolaryngol Head Neck Surg. 2000, 122:71-4.
10. Hoffstein V, Viner S, Mateika S,Conway J. Treatment of obstructive sleep apnea with nasal continuous positive airway pressure. Am Rev Resp Dis. 1992, 145:841-5.
11. Petruson B. Snoring can be reduced when the nasal airflow is increased by the nasal dilatador Nozovent. Arch Otolaryngol Head Neck Surg. 1990, 116:462-4.
12. Hoffstein V, Mateika S, Metes A. Effect of nasal dilation on snoring and apneas during different stages of sleep. Sleep. 1993, 16:360-5.
13. Schonhofer B, Franklin KA, Brunig H, Wehde H, Kohler D. Effect of nasal-valve dilation on obstructive sleep apnea. Chest. 2000, 118:587-90.
14. Rauscher H, Popp W, Wanke T, Zwick H. Acceptance of CPAP therapy for sleep apnea. Chest. 1991, 100:1019-23.
15. Rolfe I, Olson LG, Saunders NA. Long-term acceptance of continuous positive airway pressure in obstructive sleep apnea. Am Rev Respir Dis. 1991, 144:1130-3.
16. Erman MK. Conservative treatment modalities for obstructive sleep apnea. Otolaryngol Head Neck Surg. 1991, 2:120-6.
17. Rombaux PH, Listro RG, Hamoir M, Bertrand B, Aubert G, Verse T, Rodenstein D. Nasal obstruction and its impact on sleep-related breathing disorders. Rhinology. 2005, 43:242-50.
1. Master's Degree in Health Sciences. Responsible for the ORL Service of the Head and Neck Surgery Department of the Hospital Heliópolis. Responsible for the Sleep Medicine Service of Hospital Ruben Berta.
2. Doctoral Degree in Medicine at the Post-Graduation Course in Otorhinolaryngology and Head and Neck Surgery of the Federal University of São Paulo - Escola Paulista de Medicina. Professor of the Post-Graduation Course in Health Sciences of Hospital Heliópolis, São Paulo.
3. Doctoral Degree in Medicine at the Post-Graduation Course in Otorhinolaryngology and Head and Neck Surgery of UNIFESP - Escola Paulista de Medicina. Doctor
4. Free Professor at the Department of Surgery of the Medicine College of the University of São Paulo Coordinator of the Post-Graduation Course in Health Sciences of Hospital Heliópolis, São Paulo.
5. Doctoral Degree in Medicine of the Post-Graduation Course in Neurosurgery at the Medicine College of the University of São Paulo. Professor of the Post-Graduation Course in Health Sciences of Hospital Heliópolis, São Paulo.
Institution: Curso de Pós-Graduação em Ciências da Saúde do Hospital Heliópolis. São Paulo / SP - Brazil
Mail address:
Levon Mekhitarian
Neto Rua Cônego Xavier, 276 - Sacomã
São Paulo / SP - Brazil - CEP: 04231-030
Telephone: (+55 11) 5594-1227 / 8473-5521
E-mail: levonvera@uol.com.br
Article received on April 07 2009.
Accepted on May 16 2009.