 DISCUSSION
DISCUSSION At first, we must remark that the parents completed and returned less than 50% of the questionnaires, which may be understood as lack of concern of the parents regarding the possible vocal alterations of their child, lack of knowledge pursuant to the voice problems in children, lack of interest in taking part of the study, or otherwise, only parents concerned with the existence of vocal disorders in their children have preferably opted to complete the questionnaire. However, most parents (66.7%) classified the voice of their child as normal, which makes this last possibility mentioned less feasible.
Methodologically, the study was developed by creating the same opportunities so that the 75 parents invited completed the questionnaire, and according to the free authorization of the participant in taking part of the research.
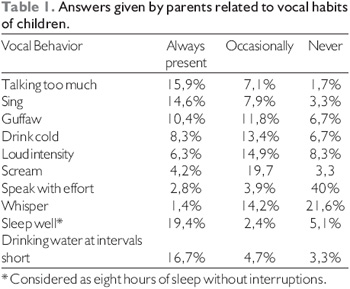
As for the results obtained in this work, we could observe abusive vocal habits in 39.6%, such as shouting, speaking excessively, speaking with strong intensity, speaking with effort and laughing loud. Vocal production in strong intensity and in a forced manner was also observed in children with chronic hoarseness (6). Children with vocal alterations maintain the strong intensity in several conversation situations, and they do not worry to fit it to the environment or with the intention of the message (2).
We also remark that vocal abuses, such as speech with too much effort or excessive speech, contribute for the setting of a hyperfunctional standard that in some moment may result in additional lesions in the vocal cords (10). It is known that primary abuse or bad use of the voice may cause, relatively early, tissue reactions in the children's vocal cords, due to the histological and behavioral plasticity they present (11).
Therefore, chronic dysphonia in the childhood is caused by the excessive use of the voice, in which children exceed the maximum and minimum limits of the vocal intensity reach as for their age (12). In this study, the answers by the parents who state there is some type of vocal alteration in the child are according to the literature, which shows such attitudes are very common in children with dysphonia (11).
In addition to the already mentioned abusive vocal factors, other habits were observed in this study, but with less occurrence, such as laughing loud and whispering. Likewise, there are findings (9) about practices taken as abusive and strongly present during the childhood, including crying, laughing (loud), imitating noises or other voices, coughing and clearing the throat (1-12), that may also contribute for vocal alteration of the child.
Before the result obtained about the abusive vocal behavior recognized by the parents, there occurs questionings involving those who did not verify the occurrence of such habits in their children. We question whether this type of vocal behavior actually does not occur or these parents only do not recognize it to be abusive and thus a professional guidance is need for consciousness of vocal habits harmful for the natural production of the voice.
In the other hand, we have to consider about the parents who answered their children commit some kind of bad use of the voice, that is, whether it is enough clear for them what the vocal habit with abusive nature is. In addition to this, the conditions of a daily accelerated live promote a more stressing behavior in the parents, which makes the dialog and the closer contact with their children more difficult and diminishes the possibility of evaluating better and becoming attentive to their vocal habits.
We need to remark that the data relating to the children's vocal habits obtained in this work shows only the perception of the parents about the vocal behavior of their children in a determined school unit, and it is not possible to infer it for the population in a general manner. However, it may contribute for a better reflection about the vocal welfare in preschool children, by associating it to other existing studies that present the same concern.
The child may develop voice problems due to vocal imitation because during the language development, he/ she learns both the meaning of the words and the manner how they are produced in auditory terms. Moreover, vocal nodes may be found in children prone to speak in strong intensity, shout constantly or produce harmful sounds by imitating animals, vehicles or heroes and monsters of cartoons (13).
Such abusive vocal behaviors may generate dysphonia and commit the communicative performance, since the voice is not only a sound produced by the vocal cords; it is also responsible for the communicative competence that depends upon the sound modulation, intensity adjustments, resonance and even the type of voice that transmits the emotional aspects and enables the characterization of the child's personality.
In this study, we confirmed that 33.3% of the participating parents perceived and considered the child's voice to be altered, and that 27.3% classified it as hoarse, according to other studies (5-6), that also confirmed hoarseness as the most common vocal alteration in children, prevailing in more early school children. In spite of the agreement with the literature concerning hoarseness, it is worth remarking that the findings relating to the normal or altered voice qualitative characterization are based on the perception by the parents pursuant to their child's voice, and are susceptible to direct influences of their auditory subjectivity, and, once added to a phonoaudiological vocal evaluation, they would have a major reliability as for this fact. However, such findings, together with what is approved by the literature, allow us to alert about the school children vocal behavior along with their parents and educators, by favoring a joint work aiming to prevent harmful vocal habits and promote the vocal welfare.
Once hoarseness followed by the vocal use in strong intensity prevailed according to the perceptions of the parents, and that in 9.1% of the altered voices, hoarseness occurred associated to strong intensity, we compose the questioning that such vocal qualities may relate or not as a cause and as a consequence.
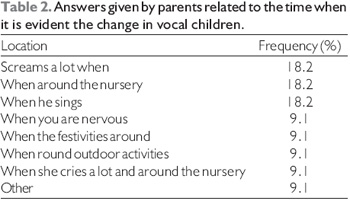
In terms of the moment in which the child's vocal alteration was mostly confirmed, according to the parents who answered there is some type of vocal disorder in their child, most of them opted for the moments at which the child returns from the day nursery school, shouts a lot and sings, each one corresponding to 18.2% of these parents. The fact the vocal alteration occurs in the return from the day nursery may be related to the opportunities to commit vocal abuses that the very educational institution offers such as the exposure to noises that lead to vocal competition and inadequate standard, that configures a negative vocal model, among others (5). According to the results found we must consider that actions promoting the vocal welfare would be healthy, such as lectures for guidance of parents, teachers and children so as to favor the occurrence of more healthy vocal habits and plays less harmful to the phonation apparatus.
It is important that the environmental question is taken into account, mainly when some moments or activities of the child favors his/her vocal worsening. This makes the health area professionals alert the parents to pay special attention to such occasions, by verifying the possible factors that lead to the worsening and thus taking care regarding the vocal health.
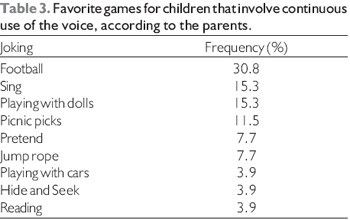
Likewise, it is worth remarking that 55.3% of the children, according to their parents, presented as favorite plays those that involve the continuous use of the voice, which also suggests an alert to the parents so as to make them understand the risks related to such plays, but considering between the child's precaution and entertainment. This is valid once these represent their favorite plays that occurs constantly. Specially for those that involve the body movement associated to vocal use, new strategies must be created corresponding to the vocal use, such as gestures and signs that favor the minor wear of the voice during the plays. Such cares are needed due to the association of physical effort and vocalization, that is, the child may present an overload on the cervical region in many activities, which favors a more compressed and tense vocalization and may damage the phonatory apparatus.
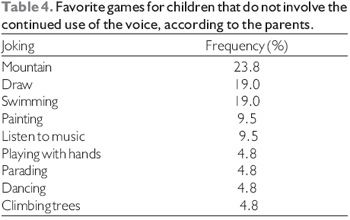
Those plays that involve the voice, but without association to any type of body effort must also be considered because, in spite of this, they are frequent plays, once frequent and favorite, and may cause vocalizations in an inadequate manner that, many times may prejudice the voice of the child, which justifies the parents' attention.
The vocal health could be observed in most present answers, and they include drinking water frequently (16.7%) and sleeping suitably (19.4%). We recommend a suitable corporeal resting for the child after the intensive use of the voice because phonation demand a large quantity of energy that needs to be daily recovered. Therefore, concomitant to the corporeal rest, the vocal rest may also be established.
Before a vocal alteration, 36.4% of the parents acted by means of dialog about the subject (vocal alteration) with the child and only 18.2% sought professional service (medical or phonoaudiological). In the other hand, only 9.1% stated they were indifferent to the child's vocal alteration.
When we treat isolated vocal disorders, the due care is not always taken, specially by the families that, many times, still consider childhood hoarseness as a temporary and unimportant symptom (9). The vocal disorders are always related to a change in the structure, function or development of phonation, they must then be suitably researched and the voice may be considered as a valuable index of health or disease of the child. The results found in this study differed from the content in the literature concerning the attention of the parents as for the vocal alterations of their children, which confirmed a concern with the vocal disorder. This result may relate to the population selected for this research, because they include parents with a high level of education.
Still according to the study, we confirmed, in the environmental question, that the habit of shouting or speaking with strong intensity at home occurred in 39.4% of the questionnaires, and the sound of the voice or style of vocal interaction of a child is normally similar to that of an adult person in his/her environment, and the child may not be conscious of it (10), which may lead us to infer that the children in these families are more prone to develop phonatory standards similar to that of their environment, that is, to the vocal model offered by their parents and educators.
The parents mention the times for meal, shower, tooth brushing and time to sleep, that are carried out by means of their order shouts, such as the moments of major vocal competition at their homes. Before such answers, we suggest strategies for placement of limits and then limit the vocal abuses. We reinforce that vocal competition among the members of the family is very evident in the dysphonic child environment (13).
In addition, the genetic, cultural and environmental characteristics bound to the personality or mood particularities are mixed in the first years of life to constitute and form the voice of a new human being (9). A study involving a large number of children of the United Kingdom, aged eight years, did not identify a significant difference between the environmental noise and the occurrence of childhood dysphonia (14).
When it comes to respiratory allergies and infection of the upper airways, the children frequently present them at the day nurseries, which makes the voice to be produced under unfavorable conditions, with dry mucosa, edemas and irritation on the vocal tract (5). In order to confirm the relation between voice and allergy, we verified in this study that the percentage of children considered to be allergic represented 63.6% of the sample, and 40.9% of these children had some type of vocal alteration.
According to the literature it is known that both allergic rhinitis and inadequate vocal habits contribute for the development of dysphonia. Before such results, it is possible to understand the association between allergic rhinitis and abusive vocal habits may significantly contribute for the development of vocal disorder and damage the communicative performance. This correlation voice-rhinitis was also observed in the literature (13), which showed about 25% of the children with vocal nodes presented with allergy. Another study involving 71 children between 3 and 13 years old and complaints of dysphonia confirmed allergic rhinitis in only 8 of these children (7). The influence of these allergic factors onto vocal production occurs mainly when associated to activities that demand vocalizations and these children may present risk of developing hyperfunctional standards of vocal behavior (10).
We may emphasize that this study contributes for the understanding of the vocal behavior in preschool children, by means of answers from their parents, which allows comparisons and enables the performance of new researches in this area, since, according to the literature, there is no specific program for prevention in preschools and therefore we find the need for more work in the promotion of healthier vocal habits (15).
We may also stand out the importance of the early detection of the childhood vocal alteration, since it is taken as a very common disorder in preschool children (6-16), and may reflect on the development of the suitable communication capacity for the adult life (2). Before the difficulties of perception of vocal alteration of the child, who hardly complains of weariness, pain or effort to speak (9) or do not believe that their hoarse voice is abnormal (17), we must stand out the importance of the family and educational guidance to provide more favorable environment and situations and contribute, when required, for the therapeutic success (10). In addition to this, we also need to consider the importance of education and clarification for the children concerning the damages they may cause to the voice, but, by demonstrating understanding because many of such behaviors are part of the child's day-by-day.
The characterization of vocal habits present in the childhood contributes for the analysis of the possible maintaining causes and factors that may relate to vocal alterations in the children.
The sample studied is brief and this research must expand by bringing other populations of different schools and day nurseries. However, based on what was mentioned from the literature and in the findings of this research, we realize the need for a work of education to the parents concerning the vocal welfare so that we may prevent childhood dysphonia. Hoarseness should not be identified as part of the normal development of the child; the plays and habits, in turn, must be reviewed for maintenance of the normal voice, the full development of communication and social and emotional adjustment of the child's discourse.
CONCLUSION For data exploitation, we conclude that most parents evaluated in this sample recognized that their children had abusive vocal behaviors, despite many of them characterized the voice as normal; the children favorite plays, predominantly involved the use of the voice; allergic rhinitis was a factor associated to some type of vocal alteration in almost half of the children; the habit of shouting or speaking with strong intensity at home occurred in less than half of the individuals researched and in some of whom this occurred on a regular basis; the parents' most common attitude faced with vocal alteration was talking to the child about the subject instead of seeking professional service.
ACKNOWLEDGMENTS To Prof. Dr. Edson Zangiacomi Martinez, for the preparation of the descriptive statistic and the Medical Student Fabrício Henrique Monaretti, for the important considerations suggested. The National Scientific and Technological Development (CNPq) for the collaboration and incentive for the beginners of the scientific area.
BIBLIOGRAPHICAL REFERENCES 1. Hirschberg J, Dejonckere PH, Hirano M, Mori K, Schultz-Coulon HJ, Vrticka K. Voice disorders in children. Int J Pediatr Otorhinolaryngol.1995, 32 (Suppl 1):S109-25.
2. Freitas MR, Weckx LLM, Pontes PAL. Disfonia na infância. Rev Bras Otorrinolaringol. 2000, 66:257-65.
3. Freitas MR, Pela S, Gonçalves MIR, Fujita RR, Pontes PAL, Weckx LLM. Disfonia crônica na infância e adolescência: estudo retrospectivo. Rev Bras Otorrinolaringol. 2000, 66:480-4.
4. Melo ECM, Mattioli FM, Brasil OCO, Behlau M, Pitaluga ACA, Melo DM. Disfonia infantil: aspectos epidemiológicos. Rev Bras Otorrinolaringol. 2001, 67:804-7.
5. Simões M, Rosa AHO, Soares JC, Ribeiro LR, Imamura VM, Bitar ML. Alteração vocal em crianças que frequentam creche. Pró-Fono. 2002, 14:343-50.
6. Silverman E, Zimmer C. Incidence of chronic hoarseness among school-age children. J Speech Hear Dis. 1975, 40:211-15.
7. Martins RHG, Trindade SHK. A criança disfônica: diagnóstico, tratamento e evolução clínica. Rev Bras Otorrinolaringol. 2003, 69:801-6.
8. Kiliç MA, Okur E, Yildirim I, Guzelsoy S. The prevalence of vocal fold nodules in school age children. Int J Pediatr Otorhinolaryngol. 2004, 68:409-12.
9. Hersan RC. Disfonia na infância. Abordagem fonoaudiológica. In: Campos CAH, Costa HOO, editores. Tratado de Otorrinolaringologia. São Paulo: Roca; 2003. 546-557.
10. Andrews ML. Terapia vocal para crianças: uma perspectiva clínica. In: Andrews ML. Terapia vocal para crianças: os primeiros anos escolares. Porto Alegre: Artes Médicas; 1998. 11-30.
11.Dejonckere PH. Voice problems in chidren: pathogenesis and diagnosis. Int J Pediatr Otorhinolaryngol.1999;49 (Suppl 1):S311-4.
12. Niedzielska G, Glijer E, Niedzielski A. Acoustic analysis of voice in children with noduli vocales. Int J Pediatr Otorhinolaryngol. 2001, 60:119-22.
13. Behlau M, Madazio G, Pontes P. Disfonias organofuncionais. In: Behlau M. Voz: o livro do especialista. Rio de Janeiro: Revinter; 2001, 295-326.
14. Cardigan PN, Roulstone S, Northstone K. The prevalence of childhood dysphonia: a cross-sectional study. J Voice. 2006, 20:623-30.
15. Hooper CR. Treatment of voice disorders in children. Lang Speech Hear Serv Sch. 2004, 35:320-6.
16. Baynes RA. An incidence study of chronic hoarseness among children. J Speech Hear Dis.1966, 31:172-6.
17. Mori, K. Vocal fold nodules in children: preferable therapy. Int J Pediatr Otorhinolaryngol.1999, 49 (Suppl 1):S303-6.
1. Phonoaudiologist. In course for Post-Graduation of the Medical College of Ribeirão Preto of University of São Paulo.
2. Doctor Professor. Professor of the course Phonoaudiology of the Medical College of Ribeirão Preto of University of São Paulo.
3. Doctor Professor. Professor at the Medical College of Ribeirão Preto of University of São Paulo. **** Associate Professor. Professor at the Medical College of Ribeirão Preto of University of São Paulo.
Institution: Departamento de Oftalmologia, Otorrinolaringologia e Cirurgia de Cabeça e Pescoço da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Ribeirão Preto / SP - Brazil. Mail Address: Prof. Dr. Hilton Ricz - Departamento de Oftalmologia, Otorrinolaringologia e Cirurgia de Cabeça e Pescoço, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo - Av. Bandeirantes, 3900 - Monte Alegre - Ribeirão Preto / SP - Brazil - Zip code: 14048-900 - Telephone: (55 16) 3602-2353 - Fax: (55 16) 3602-2860 - E-mail: hricz@fmrp.usp.br CNPq - National Council of Scientific and Technological Development.
Article received on May 8 2009. Approved on July 4 2009.