INTRODUCTION Since the life expectancy of the world population is growing, numerous studies have been developed in order to contribute to improving the quality of life in old age.
Among these studies are those related to hypertension, due to its high prevalence in this population.
Because hypertension can cause vestibular disorders due to peripheral and / or central vestibular system, causing dizziness, a portion of data related to elderly people has been conducted to verify both the relationship between hypertension and vertigo, as attitudes to be taken to minimize or counteract this symptom.
There is dysfunction of balance dizziness called whenever there is conflict in the integration of sensory information responsible for impairing postural control support the individual in space (1). Dizziness that when the roundabout is called vertigo is a sensation of loss of balance, present a multitude of diseases, affecting mainly the elderly. Its origin is correlated in 85% of cases with vestibular system disorders, their symptoms occurring generally during head motion or position changes (2.3).
The high incidence of labyrinthine disorders is partly due to hypersensitivity to various disorders of the labyrinth as hormonal, metabolic, circulatory and neck. Studies show that hearing and vestibular alterations may be secondary to hypertension (3,4).
All living cells need an adequate supply of oxygen and nutrients to maintain their functions properly, this provision depends on the functional and structural integrity of the heart and blood vessels (5). Hypertension may facilitate structural changes of the heart and blood vessels (6).
The impairment of the circulatory system can affect the inner ear that is one of the pathophysiological mechanisms described is the increase in blood viscosity, which causes a decrease in capillary blood flow and hence oxygen transport (7).
From these settings solved in this work to compare the frequency of vertigo in elderly patients with and without hypertension.
METHOD The survey was conducted by cross-sectional study, after examining and approving the project, PP/0063/09 as well as the consent by resolution 196/96-CNS.
We included 238 individuals aged over 60 years. The population was selected following the calls of the Speech Clinic at the University of Northern Parana between the years 2008 and 2009.
Were excluded from this study, patients with history of metabolic disorders such as diabetes and vascular disorders such as stroke. Also excluded were individuals with chronic renal failure.
Patients were interviewed by student volunteers and supervised undergraduate research scholars from the speech therapists responsible for the research.
We administered a questionnaire to fill in systematic clinical data such as name, age, gender and the following questions: do you have high blood pressure? Has measured your blood pressure lately? When measuring the pressure last? What has been your blood pressure? The doctor's name? Or Health Unit where he control? Takes medicine for blood pressure, which or what medications you take?. We comply with the standards established by the III Brazilian Consensus on Hypertension 1998. Were considered hypertensive those who answered affirmatively the questions related to the pathology and identified (s) drug (s) who drank. Interview was conducted with clinical data for verification of vertigo based on the protocol used in routine clinical care of the school.
The association between vertigo and hypertension was analyzed by the estimates of odds ratios (OR), point and interval and value of statistics for the Chi-square Mantel-Haenszel.
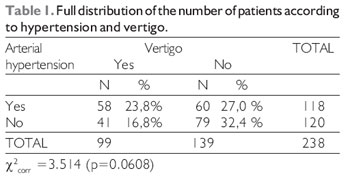
RESULTS There was a higher proportion of women in both groups, 123 (51.68%) of females and 115 (48.31%) were male. Regarding age, there was a similar mean age between the group with hypertension and normotensive patients.
Regarding the use of medicines, all subjects were taking any medication continuously as antihypertensive drugs, nonsteroidal anti-inflammatory drugs, herbal medicines, diuretics, vasodilators, antiarrhythmic, cardiotonic, benzodiazepines, oral hypoglycemics, antidepressants, antiulcer and vitamin complexes. The antihypertensive drugs were most often cited, followed by diuretics.
In this population with hypertension, 106 (90%) were using antihypertensive drugs at the time of questionnaire administration, whichever is the use of beta blockers, followed by antagonists of angiotensin II receptor, the calcium channel blockers and alpha- blockers. Of these patients, using drugs, 22 (21%) subjects were using more than one antihypertensive drug, and the association between diuretics and angiotensin-converting enzyme inhibitors, the most reported.
Of the 99 individuals who reported dizziness, 15 (15.15%) subjects were taking anti-vertigo at the time of the survey, whichever is the use of flunarizine dihydrochloride.
No significance was complaining of dizziness and hypertension in the study group (Table 1).
DISCUSSION Hypertension and heart failure can cause hearing loss and vestibular due to peripheral and / or central auditory systems and / or vestibular, and the use of drugs for metabolic and cardiovascular diseases, reported by patients, can also affect the inner ear and cause dizziness (8,9,10,11). Thus, patients with disorders associated with (a situation common in the elderly) that potentially can cause dizziness, have a higher prevalence of vertigo and an even greater loss of quality of life. This can be seen in this study show that although no association between hypertension and vertigo in this population, found that there is a high frequency of dizziness as much of hypertension in this population.
As regards the methodology of this study, despite the careful delineation of age, focusing on individuals aged over 60, some criteria as to exclude individuals with diseases and medications capable of producing dizziness certainly could not be avoided during the implementation, since the vast majority of patients had associated disorders, common in the elderly, because they can potentially cause dizziness, could have caused bias, which is not reflected in the significance of the variables.
Increasingly it has addressed the aging population in all areas of study especially in health, because he is currently on a worldwide reality. In Brazil, the absolute number of people over 60 has risen nine times in the last six decades. In 1940 was 1.7 million and in 2000 jumped to 14.5 million, projecting for 2020 a contingent of about 30.9 million people over 60 years (12).
Keeping in view the life expectancy getting louder, several studies have been conducted in order to contribute to improving the quality of life in old age, considering the magnitude and differences in each group about what they themselves value in pursuit of their welfare, and check their habits and health care, including approaches to drug use, chronic disease and physical activity (13,14,15,16).
Most notable is the large percentage of vertigo, both in the hypertensive group and 23.8% in non-hypertensive group 16%, which is in line with the literature on assunto17, 18 with a view to mention that attitudes toward check and treat vertigo in the elderly should certainly be taken. Such attitudes surely will help many patients who deliberately restrict physical activities, trips and social gatherings, with the intention to reduce the risk of such symptoms unpleasant and scary, and to avoid social stigma and embarrassment they can cause (15,16,17,18).
There is also need for all health professionals, especially those involved with older people, have much knowledge about the etiology and symptoms of vertigo, as on the treatment and consequences of it, informing the population of vertigo in general and more specifically on the approach to be taken against a framework of vertigo (19,20,21,22).
CONCLUSION Observed in this study in elderly people with and without hypertension, high frequency of vertigo, although we have not achieved significant relationship between vertigo and hypertension in this population. This is the basis for this symptom should be investigated and dealt not only the population of hypertension in the elderly but generally for better quality of life in this population.
BIBLIOGRAPHIC REFERENCES1. Ganança FF, Castro ASO, Branco FC, Natour J. Interferência da tontura na qualidade de vida de pacientes com síndrome vestibular periférica. Rev Bras Otorrinolaringol. 2004, 70(1):97-101.
2. Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG. Alterações da audição e do equilíbrio corporal no idoso. Rev Bras Med. 1999, 56(10):995-1011.
3. Teixeira LJ, Machado JNP. Manobras para o tratamento da vertigem posicional paroxística benigna: revisão sistemática da literatura. Rev Bras Otorrinolaringol. 2006, 72(1):130-9.
4. Mor R, Fragoso M, Figueiredo JF, Taguchi CK. Vestibulometria e fonoaudiologia. São Paulo: Lovise; 2001.
5. Maia RA, Diniz FL, Carlesse A. Manobras de reposicionamento no tratamento da vertigem paroxística posicional benigna. Rev Bras Otorrinolaringol. 2001, 67(5):612-6.
6. Marková M. The cochleovestibular syndrome in hypertension. Cesk Otolaryngol. 1990, 39(2):89-97.
7. Bachor E, Selig YK, Jahnke K, Rettinger G, Karmody CS. Vascular variations of the inner ear. Acta Otolaryngol. 2001, 121(1):35-41.
8. Katz, J. Tratado de audiologia clínica. São Paulo: Manole; 1989.
9. Murray KJ, Hill K, Phillips B, Waterston J. A pilot study of falls risk and vestibular dysfunction in older fallers presenting to hospital emergency departments. Disabil Rehabil. 2005, 2(9):499-506.
10. Tiensoli LO, Couto ER, Mitre EI. Fatores associados à vertigem ou tontura em indivíduos com exame vestibular normal. Rev CEFAC. 2004, 6(1):94-100.
11. Marchiori LLM, Rego Filho EA, Matsuo T. Hipertensão como fator associado à perda auditiva. Rev Bras Otorrinolaringol. 2006, 72(4):533-40.
12. Santos MRDR. Caracterização nutricional de idosos com hipertensão arterial em Teresina-PI. Rev. Bras. Geriatr. Gerontol. 2007, 10(1):1-11.
13. Vecchia R, Riuz T, Bocchi S, Corrente J. Qualidade de vida na terceira idade: um conceito subjetivo. Rev Bras Epidemiol. 2005, 8(3):246-53.
14. Marchiori LLM, Zumbido e hipertensão arterial no processo de envelhecimento. Revista Brasileira de Hipertensão. 2009, 16(1):5-8.
15. Ganança FF, Castro ASO, Branco FC, Natour J. Interferência da tontura na qualidade de vida de pacientes com síndrome vestibular periférica. Rev Bras Otorrinolaringol. 2004, 70(1):97-104.
16. Levandowski A, Bueno VK, Marchiori LLM, Melo JJ. Vertigem no idoso: relato de caso. Rev. CEFAC. 2008, 10(4):588-591.
17. Marchiori LLM Rego Filho EA. Queixa de vertigem e hipertensão arterial. Rev. CEFAC. 2007, 9(1):116-121.
18. Chung KW, et al. Incidence of horizontal canal benign paroxysmal positional vertigo as a function of the duration of symptoms. Otol Neurotol. 2009, 30(2):202-5.
19. Marchiori, L.L.M. Zumbido e hipertensão arterial no processo de envelhecimento. Rev Bras Hiperten. 2009, 16:5-8.
20. Judd O. What do patients understand by the term "Vertigo": a cross-sectional study. Clin Otolaryngol. 2009, 54:4.
21. Jolobe O. Potential causes of delayed diagnosis include convulsive syncope and cardiogenic vertigo. Q J Med. 2009.
22. Zingler VC, et al. Causative factors, epidemiology, and follow-up of bilateral vestibulopathy Ann N Y Acad Sci. 2009, 1:505-8.
22. Warninghoff JC, et al. Co-morbidities of vertiginous diseases. BMC Neurol. 2009, 9(1):29.
1 Doctorate in Medicine and Health Sciences - UEL. Research Professor.
2 MA in speech pathology. Associate Professor I.
3 Graduation Speech. Scholarship for scientific initiation UNOPAR Speech Therapy Course, Londrina, Parana, Brazil in 2009. Clinical audiologist.
4 Graduation Speech. Speech Clinic.
Institution: University of Northern Parana - UNOPAR. Londrina - Brazil. Mail Address: Luciana Lozza de Moraes Marchiori - University Campus London - Speech Therapy Clinic - Avenida Paris, 675 - Jardim Piza - Londrina - Brazil -Zip code: 86041-140 - PO Box: 401 - Telephone: (+55 43 ) - 3371-7775 - E-mail: luciana.marchiori@unopar.br
Article received on August 6, 2010. Article accepted on September 4, 2010.