INTRODUCTION Choanal atresia (CA) can be defined as a failure to develop the communication between the nasal cavity and nasopharynx (1). The incidence is 1:5.000-8.000 births, with girls being more affected than males by a ratio of 2:1, unilateral defects are more common than bilateral (2.3). It can occur as a board-membranous bone (70%), bone (20%) or membranous (10%). Diagnosis depends on high degree of suspicion, nasal endoscopy and CT of the paranasal sinuses, the treatment is surgical.
CASE REPORT MLSM, 34 year old female with a history of bilateral nasal obstruction, rhinorrhea and hyaline, sometimes mucopurulent since childhood. Reported frequent episodes of sinusitis. Do not know if reports of breathing problems at birth. Physical examination revealed no association with other congenital malformations. In oroscopy dental protrusion features and high palate. Nasal endoscopy: confirmation of bilateral atresia (Figure 1). Prompted CT of the paranasal sinuses showed that bilateral membranous atresia osteo-(Figure 2). Patient underwent a transnasal endoscopic surgical treatment, with production of mucosal flap covering the wound, without stent placement (Figure 3), and used zero-degree rigid endoscope. Uneventful post-operative period, made use of amoxicillin (500 mg orally every 8 / 8 pm for 10 days) and nasal lavage with saline solution. He was discharged after 24 hours and have been reviewed by endoscopic weekly. It was made up CT on the 40th postoperative day, which showed choanae open and broad (Figure 4). Patient recovered well and has normal nasal breathing.
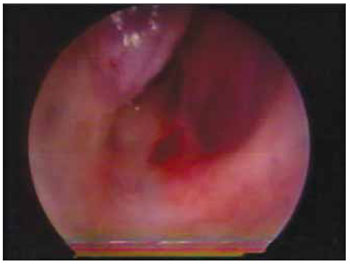
Figure 1. Endoscopic view of atresia in the right nostril.
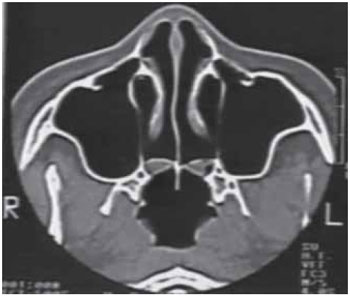
Figure 2. CT of the paranasal sinuses in axial section showing bilateral membranous atresia-bone.
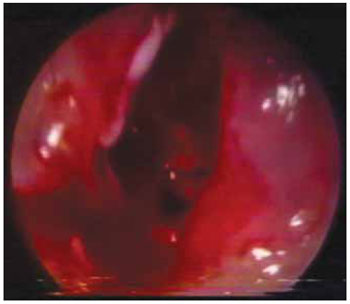
Figure 3. Endoscopic view of right choana opens.

Figure 4. CT of the paranasal sinuses in axial section showing choanae open and broad.
Choanal atresia may present as an isolated malformation or in 20% to 50% of cases, part of a group of congenital malformations, such as coloboma, heart malformation, mental retardation and growth, genital anomalies and ear or deafness (4). Thus, a complete physical examination should be done by the pediatrician and otolaryngologist to identify the possibility of the presence of these anomalies. Some theories have been proposed to explain the embryological origin of this clinical entity. Among the most accepted, four stand out: 1) persistence of oral-pharyngeal membrane, 2) failure to break the physiological oronasal membrane of Hochstetter, 3) adherence of abnormal mesodermal tissue located in the nasal choana and 4) medial growth of vertical and horizontal processes palatine bone (5,6).
Diagnosis depends on high degree of suspicion. The CA evolves with bilateral nasal obstruction, stridor, cyanosis cyclic (improving with newborn's cry), but that can lead to respiratory failure with immediate risk of death by suffocation, as the newborns are obligatory nasal breathers until about 3 weeks of life. Therefore, it is a medical emergency, requiring maintenance of the airway by oral intubation, tracheostomy tube or use of the MCGOVERN nipple, so as to stabilize the patient and schedule the definitive surgical method. Unilateral atresia may go unnoticed for years and present with Late rhinorrhea and unilateral nasal congestion, some patients, however, may remain mildly (7).
Ancillary tests such as CT of the paranasal sinuses and nasal endoscopy are essential in diagnosis and therapeutic plan - the extent, location and distinctness of atresias bone, membrane, and mixed (8). It also serves to make differential diagnosis with other diseases, such as gliomas, hamartomas, chordomas, rhabdomyosarcoma, encephaloceles, enlarged adenoid vegetations, septal deformities, among others.
Initial treatment consists of maintaining the airway, if necessary, until the definitive surgical correction, which should restore nasal airflow, preventing damage to the facial growth using a safe and fast. Currently there are several techniques: microscopic and endoscopic transnasal, transpalatal, transseptal, and dilations transantral intranasal (1,7,9,10). The transnasal endoscopic technique is being increasingly used for surgical correction of choanal atresia by offering a good view of the area, is less traumatic, have lower complication rates and provide a faster recovery after surgery (11), so we chose this technique in our case.
CONCLUSIONBilateral choanal imperforation has its early diagnosed because of symptoms more exuberant and high degree of suspicion on the part of pediatric neonatologists. It is a disease that endangers the child's life, and in most cases corrected in the first weeks. However, in rare cases it can be found during the investigation of adults with bilateral nasal obstruction and rhinorrhea, as reported in the case.
BIBLIOGRAPHIC REFERENCES1. Lazar RH, Younes RT. Transnasal repair of choanal atresia using telescopes. Arch Otolaryngol Head Neck Surg. 1995, 121(5):517-20.
2. Schwartz ML, Savetsky L. Choanal atresia: clinical features, surgical approach, and long-term follow-up. Laryngoscope. 1986, 96:1335-9.
3. Keller JL, Kacker A. Choanal atresia, charge association, and congenital nasal stenosis. Otolaryngol Clin North Am. 2000, 33(6):1343-51.
4. Tellier AL, Daire VC, Abadie V, Amiel JN, Sigaudy S, Bonnet D, Debeney PL, Durand MPM, Hubert P, Michel JL, Jan D, Dollfus H, Baumann C, Labrune P, Lacombe D, Philip N, Lemerrer M, Briard ML, Munnich A, Lyonnet S. Charge Syndrome: Report of 47 Cases and Review. Am Med Genet. 1998, 76(5):402-9.
5. Lorens DC, Casasús JC. Atresia bilateral, ósea, de coanas en adulto. An Otorrinolaringol Ibero Am. 1994, 21(5):487-96.
6. Park AH, Brockenbrough J, Stankiewicz J. Endoscopic versus traditional approaches to choanal atresia. Otolaryngol Clin North Am. 2000, 33(1):77-90.
7. Samadi DS, Shah UK, Handler SD. Choanal atresia: A twenty-year review of medical comorbiditied and surgical outcomes. Laryngoscope. 2003, 113:254-8.
8. Schweinfurth JM. Image guidance-assisted repair of bilateral choanal atresia. Laryngoscope. 2002, 112:2096-8.
9. Vogels RL, Chung D, Lessa MM, Lorenzetti FTM, Goto EY, Butugan O. Bilateral congenital choanal atresia in a 13-year-old patient. Int J Pediatr Otorhinolaryngol. 2002, 65:53-7.
10. Josephson GD, Vickery CL, Giles WC, Gross CW. Transnasal endoscopic repair of congenital choanal atresia. Arch Otolaryngol Head Neck Surg. 1998, 124(5):537-40.
11. Cedin AC, Rocha JrFP, Deppermann MB, Manzano PAM, Murao M, Shimuta AS. Transnasal endoscopic surgery of choanal atresia without the use of stents. Laryngoscope. 2002, 112(4):750-52.
1 Specialist in Otorhinolaryngology. Service Coordinator of Medical Residence in Otorhinolaryngology, Hospital Sao Jose do Avai.
2 Resident of Otorhinolaryngology, HSJA (R3).
3 Resident of Otorhinolaryngology, HSJA.
4 Medical intern at the Department of Otolaryngology HSJA.
5 Academic intern at the ENT Department of HSJA.
Institution: St. Joseph's Hospital Avai. Itaperuna / RJ - Brazil. Mail Adress: José Carlos Oliveira Pereira - Rua Coronel Luiz Ferraz, 397 - Centro - Itaperuna / RJ - Brazil - Zip code: 28300-000 - Telephone: (+55 11) 9251-5451 - E-mail: josecarlosop@hotmail.com
Article received on 21 May, 2009. Approved on August 7, 2009.