INTRODUCTIONThe nasoalveolar cyst is a rare benign lesion, located in topography of nasolabial folds, anteroinferior of the piriform rim of nasal cavity. It´s a lesion that is usually unilateral (90% of the cases) (1,2), affecting mainly people of black race, of feminine gender, in the age group which comprises between the 4th and 5th decades of life (1,2).
The first to describe this pathology was ZUCKERKANDL in 1882 (3). This embryonic, non-odontogenic, usually asymptomatic, being diagnosed late, due to the facial aesthetics changes and breathing. Although diverse synonymy (nasoalveolar cyst, KLESTADT cyst, congenital mucoid cyst of the nasal edge), the term considered most appropriate, at the moment, is nasolabial cyst (4).
Besides literature review, this study has as objective, report the case of a patient with bilateral nasoalveolar cyst, presenting clinical aspects, surgical, histopathological and radiographic.
CASE REPORTPatient AWV, feminine gender, 24 year-old, mulatto, coming and natural of São Paulo, housewife, sought for treatment at Otorhinolaringoloy Paulista Hospital, SP, Brazil, complaining about bulge region of bilateral nasolabial, of progressive evolution for about 06 months, associated to the nasal obstruction in the last 02 months. Patient denied pain, rhinorrhea, nasal itching, sternutatory, epistaxis or other nasal complaints.
At the otorhinolaryngological examination, it was observed bulging without signs of inflammation at bilateral nasolabial region and superior gingivolabial sulcus, especially on the right, raising the nasal floor and erasing the bilateral nasolabial folds. The computerized tomography of paranasal sinuses showed two cystic lesions parallel to the bilateral nasal spine (Figure 1), nasal floor bulging, depression in the anterior maxillary bone bilateral and displacement of the anterior portion of inferior turbinate left up (Figure 2).
For this case, we had chosen to perform the surgical excision of the lesion, at surgical room , under general anesthesia. After local infiltration of anesthetic solution (Lidocaine at 2% with epinephrine 1:100.000), central incision was made (approximately 6,0 cm) in the superior gingivolabial sulcus, below the cystic lesions, between the lateral incisors of both sides, followed by detachment of the anterior region of cysts, with visualization of these two lesions separated by a bony septum, the left side measuring, approximately 2,0cm and the right side, around 3,0cm (Figure 3). It was performed a dissection of the right cyst, initially, preserving its contents, being possible the detachment of the lateral walls. It was located the nasal floor plane (nasal mucosa) at the superior region of the cyst; at this point, for better detachment, it was chosen by emptying the contents serous, with yellowish color, of the cyst by needle and syringe. After emptying the cyst, it was performed a careful dissection in its upper portion, which kept contact with nasal mucosa, region where it presented greater adherence. The displacement was performed without lesion of the nasal mucosa. At the back region of the cyst, the displacement showed planes less adhered, facilitating the removal. The same surgical technique was performed at the left side of the cyst, being possible to indentify the nasal floor mucosa and perform the removal without lesion (Figure 4). Synthesis was performed at plans dissected, with absorbable lines (Catgut 2-0, simple).
At immediate postoperative, patient complained of paresthesia at anterior region of the upper lip and nasal vestibule, which remained for 03 months.
Patient is at ambulatory accompaniment of postoperative for 06 months, without evidences of recurrence or other changes, presenting improvement of nasal obstruction.
Anatomopathology
It was sent for histological study, two cystic structures previously sectioned, conserved in formaldehyde, and represented wall studs, smooth and bright, with shades of brown color. The larger structure measured 3 x 2,5 x 1 cm and the smallest, 2,5 x 1,5 x 0,5cm.
The sample was submitted to the processing chemical pradronized, obtaining a block of paraffin to each cystic structures, being made the respective histological concoction, with thickness of 5 (five) micra and color by the technique of hematoxylin-eosin and PAS (Schiff periodic acid).
The histological study revealed identical aspect in both lesions, being identified of cystic wall constituted by loose connective tissue showing moderate edema, covered by two different types of epithelium: the predominant was of the type stratified squamous, with preservation of the polarity and absence of nuclear atypia, removing away the suspicion of malignancy.
The other type of epithelium was constituted by one or two layers of cylindrical cells sometimes massive clear vacuoles in the cytoplasm (Figure 5), that special color by the technique of PAS revealed weak positivity to the mucopolysaccharide substances (Figure 6). At the connective tissue wall, the histological sections revealed nerve fibers and blood capillaries of ecstatic lights, alongside to the moderate interstitial edema. Some muscle striated fibers was also indentified at the region of surgical region.
The anatomopathological diagnosis was of bilateral nasolabial cyst.

Figure 1. Computerize Tomography shows bilateral nasolabial cyst, obstructing the nasal cavity and forming bone erosion.
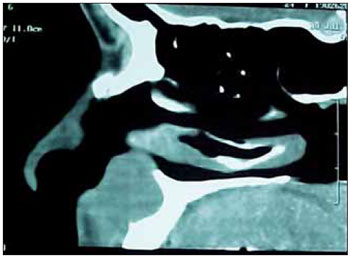
Figure 2. Nasolabial cyst moving the anterior portion of the inferior nasal turbinate upwards.
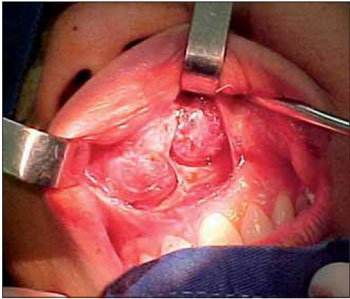
Figure 3. Intraoperative showing bilateral nasolabial cysts. Vision through the Denker incision.
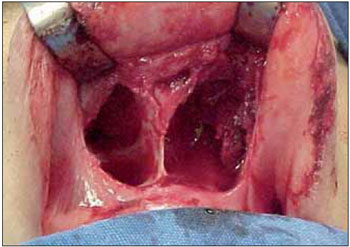
Figure 4. The operative field after removal of nasolabial cysts, presenting bone erosion.
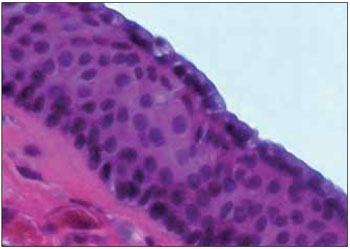
Figure 5. 400X - nasolabial cyst - hematoxylin-eosin. Observe the pluri squamous epithelium formed by the poligonal cells, abundant cytoplasm and acidophilic around the round nuclei, isochromatic. Superficially, single layer of cylindrical cells showing vacuolated and clear cytoplasm.
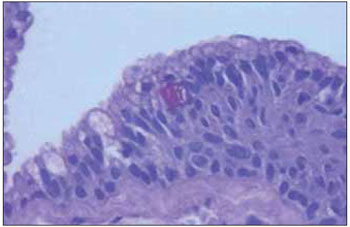
Figure 6. 400X - nasolabial cyst - PAS. Note accumulation of PAS-positive granules in the cytoplasm of the cell located in the center of the microscopic field.
The nasoalveolar cyst is an embryonic cyst, non-odontogenic, which has its controversial origin , being the theories based on:
1) cyst originated from the invagination of ectodermal debris among the processes nasal side and media being for that reason, considered as fissural cyst (Klestadt Theory, 1913) (1,5,6);
2) cyst derived from the epithelium of the nasolacrimal duct during the embryonic period (Bruggemann Theory, 1920) (5,7).
For reason of its poor symptomatology, this disease is underdiagnosed (8), showing in the literature, an incidence of 0,7% of all maxillofacial cysts and 2,5% of non-odontogenic cysts. In the presented case, we observed a mulatto patient, even being more common at black race, according to the literature. Epidemiological data shows that this cyst is more frequent in persons of feminine gender, in the proportion of 4:1 (when unilateral) and 5,5:1 (when bilateral) (9). The age group most affected includes the 4th an 5th life decades (2,3,7). The cysts presentation is most unilateral (90%), being only10% bilateral (1, 2, 8).
Clinically, this lesion presents as a bulging of slow growing located at the portion ventral inferior of piriform fossa region. In the course of time, the cyst leads to a facial deformity with a deletion of nasolabial folds, nasal obstruction by the elevation of nasal floor and superior displacement of the anterior portion of the inferior turbinate. It is worth to highlight that the dentition remains intact (6). Eventually, it may occur cyst infection (50% of the cases), presenting signs of inflammation. In this infection cases, it can occur the cyst drainage to the oral cavity and /or to the nasal vestibule (3,6).
The diagnosis of nasoalveolar cyst is clinical and topographic, with visual and palpation of the affected area (6). The workup done by the imaging examination confirms the suspicion and the clinical examination, being the Computerized Tomography the examination of choice, which may show, in some cases, jawbone erosion (10,11, 12). The nasolabial cyst consists of lesion in the soft parts, and for this reason, the x-ray being considered an obsolete examination, capable to show few details; except in the cases in which the cyst presents gigantic dimensions leading to the significant erosion of the jawbone.
The differential diagnosis which must be done with the nasolabial cyst include the dermoid , nasopalatine, median palatal, median alveolar, globulomaxilar cysts (which origin in the interior of the bone), besides of furuncles at nasal floor, which resembles to infected nasolabial cyst (13).
in the literature, it has been reported Just one case (Arnold, 1929) of nasolabial cyst which evolves to carcinoma (9,14).
Although there are reports of treatment of nasolabial cyst by sclerosing substances or marsupialization (15), the most indicated therapy found in the literature is surgical removal. Enucleation can be performed with local anesthesia or general, being the best way to access the Denker incision ( intra-oral incision, sublabial next to the incisive fossa) which offers an ample exposition. During the surgery, should take in account the cyst intimate adherence with the nasal floor (3,16), detail that, constantly, leads to the laceration of the mucosa in this region of the nose. This was possible to avoid in this case, in which we had chosen to empty the cystic contents to obtain a better dissection of the cyst in relation to this region of nasal floor. The closing of the planes should be complete, in order to avoid possible oronasal fistulas. By the reason the extension of the cysts related did not affected the region of nasal wing, it was not necessary apply any technique to avoid retraction. The surgery aims the facial esthetic restoration, the nasal function (in case it is affected) and the prevention of recurrent infections, which can be associated, and minimize the patient anxiety
The surgical treatment present few complications, among them may recede with deformity of the nasal ala, mainly in Blacks and still, oronasal fistula. Recurrence of the cyst is rare and the prognosis is very good (5,7).
The description of the surgical technique in this case, aims to provide a foundation to help similar cases in order to obtain surgical success, without submit the patient to complications and disease recurrence.
BIBLIOGRAPHICAL REFERENCES1. Barzilai M. Bilateral nasoalveolar cysts: case report. Clin Radiol. 1994, 49(2):140-141.
2. Cohen MA, Hertzanu Y. Huge growth potential of the nasolabial cyst. Oral Surg. 1985, 59:441-5.
3. Allard RHB. Nasolabial cyst. A review of the literature and report of cases. Int J Oral Surg. 1982, 11:351-359.
4. Fanibunda KB. Bilateral nasolabial cysts: a case report. Dent Pract. 1970, 20:249-250.
5. Graamans K. Nasolabial cysts: diagnosis mainly based on topography?. Rhinology. 1983, 21:239-249.
6. Kuriloff DB. The nasolabial cyst-nasal hamartoma. Otolaryngol Head Neck Surg. 1987, 96:268-272.
7. David VC, O´Connell JE. Nasolabial cyst. Clin Otolaryngol. 1986, 11:5-8.
8. Smith RA, Katibah RN, Merrell P. Nasolabial cyst: report of a case. J Canad Dent Assoc. 1982, 11:727-729.
9. Roed-Peterson B. Nasolabial cysts: a presentation of five patients with a review of literature. Br J Oral Surg. 1969, 7:84-95.
10. Adams A. Roentgeno-Oddities. Oral Surg. 1985, 60:118-119.
11. Balfour RS. Nasoalveolar cyst. J MD State Dent Assoc. 1977, 20:92-94.
12. Seward GR. Nasolabial cysts and their radiology. Dent Pract. 1962, 12:154-161.
13. Karmody CS, Gallagher JC. Nasoalveolar cysts. Ann Otol. 1972, 81:278-283.
14. Egervary G, Csiba A. Bilateral nasolabial cyst. Dental Digest. 1969, 75:504-7.
15. Crowford W, Korchin L, Greskovich FJ. Nasolabial cysts: report of two cases. J Oral Surg. 1968, 26:582-588.
16. Brandão GS, Ebling H, Souza IF. Bilateral nasolabial cyst. Oral Surg. 1974, 37:480-484.
1) Fellow in Pharyngology at Clínicas Hospital of Medicine College at São Paulo University. Otorhinolaryngologist.
2) PhD in Otorhinolaryngology by Paulista School of Medicine. Preceptor of medical residency in Otorhinolaryngology at Paulista Hospital, São Paulo - Brazil.
3) Fellow in Plastic Surgery of the Face at Clínicas Hospital of Medicine College of São Paulo University. Otorhinolaryngologist.
4) Otorhinolaryngologist.
5) Master in Pathological Anatomy. Pathologist
Institution: Paulista Hospital of Otorhinolaryngology. São Paulo / SP - Brazil. Mailing address: Alexandre Minoru Enoki - 369 Jaú, Alameda - Apto 610 - Jardim Paulista - São Paulo / SP - Brazil - Zip-code: 01420-000 - Telephones: (+55 11) 3262-2328, (+55 11) 7159-2131 - E-mail: enoki@terra.com.br
Article received in 2009 November 26th. Article approved in 2010 April 25th.