|
564 |
|
| Year: 2008 Vol. 12 Num. 4 - Out/Dez - (5º)
|
|
 |
| Section:
Original Article
|
|
|
|
|
| Microbiology of Middle Meatus in Healthy Individuals |
|
| Author(s): |
| Afonso Ravanello Mariante1, Elisabeth Araújo2, Celso Dall'Igna3, Vladmir Cantarelli4, Bruno C. Palombini5, José da Silva Moreira6
|
|
|
| Key words: |
| microbiology, middle meatus, healthy |
|
|
 |
| Abstract: |
Introduction: The nasosinusal microbiology of healthy individuals is not much documented. Its knowledge allows to determine the nasosinusal colonizing agents and to monitor the patterns of bacterial resistance. Objective: To evaluate the microbiology of the middle meatus in healthy individuals and to compare it with that of patients with chronic rhinosinusitis. Method: 61 healthy individuals were included. The samples were collected under endoscopic view and Gram stained with leucocytes count and aerobic, anaerobic and fungus cultures. 114 patients with chronic rhinosinusitis formed the control group. Results: In healthy individuals 58 microorganisms were isolated. The most frequent ones were coagulase-negative Staphylococcus, Staphylococcus and Corynebacterium. Fungi were cultivated in 10%. There were rare or no white blood cells in all samples. There was penicillin resistance in 75% of the Staphylococcus aureus and 69% of the coagulase-negative Staphylococcus. As for oxacillin, 100% of Staphylococcus aureus and 92% of coagulase-negative Staphylococcus were sensitive. In the control group 158 microorganisms were cultivated. The most common ones were Staphylococcus aureus and coagulase-negative Staphylococcus. Gram-negatives represented 26% of the aerobics. 73% of the samples with positive cultures presented a few or many white blood cells. Conclusion: Rare or no white blood cell, coagulase-negative Staphylococcus and Corynebacterium were more frequent in healthy individuals and Streptococcus pneumoniae, anaerobics and oxacillin resistant coagulase-negative Staphylococcus and Gram-negative were more frequent in the control group.
|
|
|
INTRODUCTION
The nasosinusal microbiology of healthy individuals is not much documented (1, 2, 3, 4), specially in the middle meatus (5, 6, 6), a region where the frontal ethmoidal maxillary sinuses draining holes are located. Its knowledge enables the determination of the nasosinusal colonizing agents, something crucial for a better understanding of rhinosinusitis and the monitoring of the bacterial resistance trends.
Nasal endoscopy revolutionized the nasal culture by allowing the obtainment of secretions samples directly from the draining place with a minimal risk or discomfort (8). Araújo et al. (9) revealed the validity of the middle meatus samples collection under endoscopic control to determine the nasosinusal microbiology.
The bacterial resistance is a worldwide phenomenon, but there are variations in the bacteria sensitivity to antibiotics between countries and continents. In Brazil, with its continental dimensions, such variation must exist between regions. The semiquantitative leucocytes count helps the differentiation between colonizing and pathogenic microorganisms. The obtainment of middle meatus samples allows the guided treatment through the culture and sensitivity to antimicrobials.
In spite of its great importance, the literature still has a gap about the nasosinusal microbiology of healthy individuals, as well as concerning the colonizing or pathogenic behavior of such microorganisms.
Taking all these questions into account, we idealized this study to identify the middle meatus bacterial flora, determine the antimicrobial sensitivity in healthy individuals, and compare it with that of patients with chronic rhinosinusitis.
METHOD
We performed a contemporary cohort study with transversal cut, in which 61 healthy volunteers and 114 patients with chronic rhinosinusitis, who formed the control group, were evaluated in the period comprised from March 1999 and January 2007, in Porto Alegre.
We considered to be healthy the individuals without nasosinusal complaints and who didn't present with secretion or polyps in the middle meatus during the nasal endoscopic exam. No radiologic exams were performed in the paranasal sinuses in this group. We included individuals who hadn't used antimicrobials, corticosteroids, nasal atomizers or illicit drugs in the period of 21 days prior to the study accomplishment (6, 7). We left out carriers of septum deviation that prevented us from viewing the middle meatus (10).
The inclusion criteria for the control group were: presence of signs and symptoms of rhinosinusitis with duration of at least three months, without response to medication treatment with amoxicillin associated to clavulanate and/or second generation cephalosporin, for four weeks (11); rhinosinusal commitment confirmed by computerized tomography of the paranasal sinuses and middle meatus secretion at the moment of the nasal endoscopy (12, 13, 14, 15). We excluded from the control group the individuals who had used antibiotics in the 21 days prior to the sample collection and/or presented with septum deviation that prevented us from viewing the middle meatus (5, 10).
The samples were collected under endoscopic view (rigid endoscopes Storz of 4 mm or 2.7 mm, with angulation of 30º or 0º). The equipment were previously sterilized with immersion in glutaraldehyde at 2% during 20 minutes. Then, sterile cottons wetted in neotutocaine (4%) were inserted into the nasal cavity for 5 minutes (10, 16) and the endoscope was used to lateralize the nasal wing, avoiding its contact with the swab, placed in the middle meatus for the material collection (6,7).
The samples were forwarded to the laboratory at most 1 hour after collection, in Stuart transportation means (Starplex Scientific, Ontario, Canada) for cultivation of aerobic microorganisms and in thioglycolate broth for anaerobes cultivation.
In the laboratory, the bacterioscopic exam was performed by using the Gram coloration. The presence of leucocytes was determined by semiquantitative technique, with classification into four groups: absent; uncommon from 1 to 5; a few from 5 to 25; and numerous, above 25 leucocytes per field of a thousand increases. (6, 17, 18).
For the aerobic culture, the material was sowed in plates containing the middle of agar McConkey (Difco, Detroit, USA or Becton Dickinson, Maryland, USA) and agar Tripticase Soy (Difco, Detroit, USA) enriched with 10% of sheep blood (blood agar) and incubated at 37o C for 24 hours. Where there was no bacterial growth, the middles were reincubated for 24 more hours before they were released as negatives.
The cultivation for anaerobic germs was performed through sheep blood agar sowing based on brucella blood agar (Difco, Detroit, USA) and the bacteroide bile esculine agar, with incubation for up to 72 hours in the anaerobiosis atmosphere provided by the Gaspak systems (Becton Dickinson, Maryland, USA), Anaerocult (Merck SA, Brazil) or Anaerobic (Probac, São Paulo, Brazil). The thyoglycalate broth was used as a backup for anaerobes sowing in case of suspicion of the presence of germ cells in the sample (calculated by the Gram method) and the absence of growth in the plates. After the isolation and confirmation it was anaerobic germ, the microorganism identification was made with the use of the API system for anaerobic germs (Bio Merieux, France).
The mycological analysis was carried out through the material direct exam, between lamina and glass slide, and culture of the material in the middle of Sabouraud with or without chloramphenicol and cycloheximide (BBL). The incubation was made at 25o-35o C and the cultures were observed up to 20 days for release as negatives for fungi. The fungi and yeasts identification was made from the microscopic morphology and the use of a commercial kit for identification of yeasts (API system, Bio-Mereux, France), respectively.
The determination of the (MIC) minimum inhibitory concentration and the bacterial identification were made by automation (MicroScan, AutoScan-4) through isolation of the bacterium in (BHI) Brain Heart Infusion Broth, incubated at 35o-37o for 6-12 hours and inoculated in proper panels for Gram-positives or Gram-negatives.
The lab procedures and the antibiogram results complied with determination by the (NCCLS) National Committee for Clinical Laboratory Standards, and took into account the bacterial species and the infection location (19). The statistical package employed was the (SPSS) Statistical Package for Social Sciences 8.0. For proportions comparison we used the Chi-square test with Yates correction. The acceptable error was of 5% (p < 0.05). The Fischer's exact test was applied when the number expected for a given characteristic was lower than 5 patients (17).
The project was approved by the institution ethics committee. The healthy individuals were informed about the study and gave oral consent and the control group members signed a free and clear consent term. No patient included in the study was remunerated.
RESULTS
Out of a number of 61 samples cultivated in healthy individuals, 82% were positive and 58 microorganism were isolated (Table 1). From which the most prominent were the negative Staphylococcus coagulase, Staphylococcus aureus and Corynebacterium sp., respectively, in 44%, 20% and 16% of the samples. We observed mixed flora in 13% and sterile samples in 18% of the individuals. No anaerobic germ was isolated.
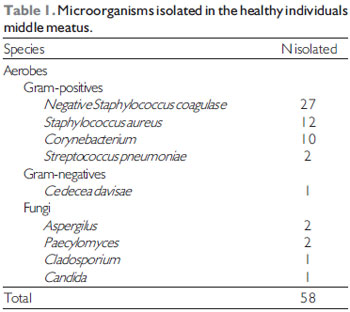
The mycological culture was positive in 6 samples, and 2 Paelomyces, 2 Aspergillus sp., 1 Cladosporium and 1 Candida sp. were identified. There was no growth at the direct exam, which characterized colonization.
All patients presented with rare or no leucocytes in semiquantitative count. As for the bacterial resistance standards, we identified within the isolated Staphylococcus aureus resistance to penicillin and erythromycin, respectively, in 75% and 33%; and 100% of sensitivity to oxacillin. Within the negative Staphylococcus coagulase, 69%, 74% and 8% presented resistance to penicillin, erythromycin and oxacillin respectively. The Corynebacterium presented 30% and 40% of resistance to erythromycin and sulphamethoxazole/trimethoprim and 100% of sensitivity to penicillin.
The control group was composed by 114 patients with chronic rhinosinusitis. One or more samples were collected from all of these patients. Eight per cent of the samples were sterile and 15% had mixed flora.
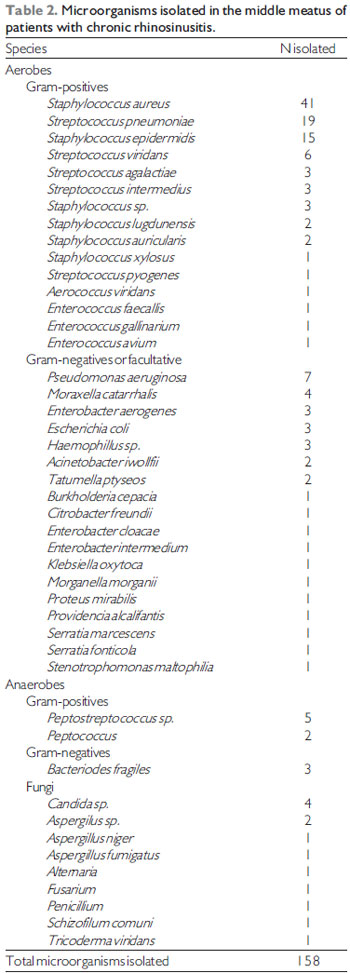
A total of 158 microorganisms were cultivated (Table 2): The Staphylococcus aureus was present in 26% of the samples, negative Staphylococcus coagulase in 14% and Streptococcus pneumoniae in 12%. Gram-negatives or facultative were identified in 26% of the aerobes. The anaerobe germs were isolated in 8% of the samples.
Fungi were cultivated in 14% of the control group samples. The fungal rhinosinusitis was classified as allergic in four cases, and as fungal boll in three cases. In six patients the fungi were deemed to be colonizing for the direct exam was negative and for there was no evidences of fungal rhinosinusitis.
In the leucocytes count analysis by the Gram method, 46% of the samples presented with numerous leucocytes, 29% a few, 9% rare and 16% absent. Among the samples with positive culture, 73% showed numerous or a few leucocytes.
As for the bacterial resistance standards in the control group, the negative Staphylococcus coagulase were resistant to penicillin in 90% of the samples, erythromycin in 75%, clyndamicin in 66%, oxacillin in 53% and gentamicin in 43% of the samples. As for the Staphylococcus aureus, 78% of the samples presented resistance to penicillin, 44% to erythromycin, 24% to clyndamicin, 17% to gentamicin and 16% to oxacillin, and all of these were sensitive to levofloxacin.
In the leucocytes count comparative study by the Gram's method, the control group presented with a statistically significant difference, with 100% of rare and absent cases against 25% in the patients with chronic rhinosinusitis (p <0.001).
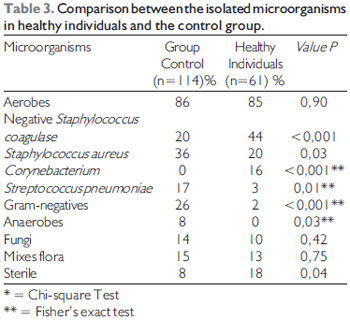
Sterile samples, negative Staphylococcus coagulase and Corynebacterium were statistically more frequent in the healthy individuals, while Staphylococcus aureus, Streptococcus pneumoniae, the Gram-negatives and the anaerobes were statistically more frequent in the control group (Table 3).
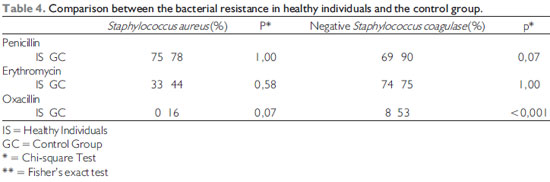
When it comes to the comparison of the bacterial resistance patterns between the healthy individuals and the control group, only the negative Staphylococcus coagulase resistance to oxacillin was statistically higher in the control group (Table 4).
DISCUSSION
The works published so far on the nasosinusal microbiology in healthy persons present significant aspects, observed in the patients selection, the nasal mucosa sterilization methods or the evaluation of bacterial resistance patterns.
The techniques have already been described for the obtainment of nasosinusal samples for the microbiological study. Out of which we found the nasal swab and the swab of nasopharynx, the aspiration of the maxillary sinus secretion, through biopsy via canine cavity, and the swab of the middle meatus under direct or endoscopic view.
The culture obtained through the placement of a swab in these nasal secretions allows the identification of microorganisms with a minimal risk or discomfort to the patient. However, this technique has been criticized for its high bacterial contamination potential present in the nasal vestibule.
The maxillary sinus direct biopsy method was during a long time taken as a golden-standard to determine the nasosinusal cavity microorganisms, but it's not free from controversies. In addition to being an uncomfortable procedure, it requires sedation or general anesthesia. The biopsy is also related to infra-orbital nerve lesions and, in children, to lesions in the dental germs (20). Nevertheless, its major restriction is the fact of providing the maxillary sinus with restrict information.
The nasal endoscopy brought a new perspective to the nasal culture, because it allows the collection of secretion directly from its draining locations, and reduces the contamination risk. In 1992, Poole (21) revealed cultures of samples obtained closely but not directly from mucopurulent secretions were failures in the attempt to identify the pathogenic agents.
The parameters used for selection of the healthy individuals and the sample collection methods were similar to those proposed by Nadel et al. (6) and by Klossek et al. (7). The inadequate selection of the groups is reflected in the results interpretation and makes one object works such as the one by Gordts et al. (22, 23), who consider the children submitted to variable surgical procedures to be healthy.
The main studies (6, 7) about the middle meatus microbiology in healthy individuals published so far have not performed the disinfection of the nasosinusal mucosa. In our study, we adopted as a mucosa sterilization method the placement of cotton turundas wetted in neotutocaine at 4% in the nasal cavity, with as asserted by some authors (16, 17).
In the microbiology study of the healthy individuals, Savolainen et al. (2) and Gordts et al. (22) reported on 100% and 75% of positive cultures in samples collected under direct view. Klossek et al. (6) and Nadel et al. (7) found, respectively, 80% and 82% of positive cultures in samples collected under endoscopic control, findings similar to those of our study.
In our study, the SCN, Staphylococcus aureus and Corynebacterium were the most frequent microorganisms in the middle meatus of the healthy individuals. Such germs were considered to be saprophyte for the absence or rarity of leucocytes in the Gram's method and configure a finding similar to those of Klossek et al. (6) and Nadel et al. (7).
As far as anaerobe microorganisms are concerned, all the cultures were negative, differently from the abovementioned authors, who identified them in, respectively, 15% and 20% of the healthy individuals.
Fungi were cultivated in 10% of the healthy individuals, however, they were not identified in the direct exam, and were deemed to be colonizing. Ponikau et al. (24) isolated fungi by PCR in 100% of the healthy individuals. Other authors (25) also found their high prevalence in the healthy nasal cavity, while Rao et al. (26) didn't identify fungi in healthy individuals. We believe fungi may be frequently isolated in the nasal cavity, but such results should not be overestimated. The positive culture must be relating to the clinical picture and the direct exam.
In a comparative study between the middle meatus microbiology of healthy individuals and patients with chronic rhinosinusitis, we identified Staphylococcus aureus and negative Staphylococcus coagulase as microorganisms with high prevalence in both groups. However, like Klossek et al. (15), we found SCN with major frequency in healthy individuals. Our findings reinforce the concept that negative Staphylococcus coagulase are predominantly saprophytes, but, when found with numerous leucocytes, they may represent a true infection.
As for the bacterial resistance indexes, the main studies published (6, 7, 22) don't make any comment on the healthy individuals bacteria patterns. As far as the Staphylococcus aureus resistance to penicillin is concerned, our results were similar to those by Tewodros (27), who identified 74% of resisting microorganisms, and lower than those by Ali et al. (28) and Paul et al. (29) who reported, respectively, 93% and 98%.
Our results regarding the occurrence of oxacillin resistant Staphylococcus aureus in the nasal cavity of healthy individuals were very divergent from Alghaithy et al. (30), who confirmed an incidence of 11%, too much higher than that reported in the literature (28, 29). The high level of resistance identified by these authors may be explained by the indiscriminate use of antibiotics in some regions.
Upon comparison of the resistance patterns in healthy individuals with that of the control group, we identified a higher frequency of resistant Staphylococcus aureus and negative coagulase. However, such difference was statistically significant only for negative Staphylococcus coagulase.
This study results analysis confirms the presence of a commensal flora in the middle meatus, similar to that identified in patients with chronic rhinosinusitis, as well as the extreme need for use of technique to determine the pathogenicity or not of the microorganisms, such as, the semiquantitative leucocytes count.
The bacterial resistance is an emerging problem in all medicine areas. Prolonged and repeated treatments are surely implied with the mitigation of the sensitivity to the antimicrobials. The correct knowledge of the healthy individuals microbiology, as well as their patterns of resistance to antimicrobial may be used in the prevention of the resisting origins appearing and in the promotion of a long-lasting efficiency for the high spectrum antibiotics.
CONCLUSIONS
The negative Staphylococcus coagulase, Corynebacterium and Staphylococcus aureus were the most prevalent microorganisms in the middle meatus of the healthy individuals. Fungi were present in 10% of the individuals. No anaerobic germs were identified.
In the comparative study between the healthy individuals and the control group, absence or rarity of leucocytes, sterile samples of negative Staphylococcus coagulase were more frequent in healthy individuals, while Staphylococcus aureus, Gram-negatives, anaerobes and Streptococcus pneumoniae were more frequent in the control group.
The susceptibility to penicillin was observed in 25% of the Staphylococcus aureus, in 31% of the negative Staphylococcus coagulase and in 100% of the Corynebacterium. In the comparison of the bacterial resistance of the healthy individuals with the control group, we identified in the latter a higher frequency of oxacillin resistant negative Staphylococcus coagulase.
BIBLIOGRAPHICAL REFERENCES
1. Brook I. Aerobic and anaerobic bacterial flora of normal maxillary sinuses. Laryngoscope. 1981, 91:372-5.
2. Savolainen S, Ylikoski J, Jousimies-Somer H. The bacterial flora of the nasal cavity in healthy young men. Rhinology. 1986, 24:249-55.
3. Jousimies-Somer HR, Savolainen S, Ylikoski JS. Comparison of the nasal bacterial floras in two groups of healthy subjects and in patients with acute maxillary sinusitis. J Clin Microb. 1989, 27:2736-43.
4. Ylikoski, J. Savolainen, S., Jousimies-Sommer, H. Bacterial Flora in the nsafarynx and nasal cavity of healthy young men. Oto Rhino Laryngolgy. 1989, 51:50-55
5. Axelsson A, Brorson JE. The correlation between bacteriological findings in the nose and maxillary sinus in acute maxillary sinusitis. Laryngoscope. 1973, 83:2003-11.
6. Klossek JM, Dubreuil L, Richet B, Sedaillan A, Beutter P. Bacteriology of the adult middle meatus. J Laryngol Otol. 1996, 110:847-9.
7. Nadel DM, Lanza DC, Kennedy DW. Endoscopically guided sinus cultures in normal subjects. Am J Rhinol. 1999, 13(2):87-90.
8. Araújo E, Dall C, Cantarelli V, Pereira A, Mariante AR. Microbiology of middle meatus in chronic rhinosinusitis. Rev Bras Otorrinolaringol (Eng Ed). 2007, 73(4):549-55.
9. Araujo E, Palombini BC, Cantarelli V, Pereira A, Mariante A. Microbiology of middle meatus in chronic rhinosinusitis. Am J Rhinol. 2003, 17(1):9-15
10. Erkan M, Aslan T, Ozcan M, Koç N. Bacteriology of antrum in adults with chronic maxillary sinusitis. Laryngoscope. 1994, 104:321-4.
11. International Rhinosinusitis Advisory Board. Infectious rhinosinusitis in adults: classification, etiology and management. Ear Nose Throat J. 1997, 76 Suppl 72:1-19.
12. Araujo E, Sakano E; Weckx L. I Consenso Brasileiro sobre Rinossinusite. Rev Bras Otorrinol. 1999, 65(3) Suppl 9.
13. Bhattacharyya N, Kepnes RNP. The microbiology of recurrent rhinosinusitis after endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg. 1999, 125:1117-20.
14. Gold SM, Tami TA. Role of middle meatus aspiration culture in the diagnosis of chronic sinusitis. Laryngoscope. 1997, 107:1586-9.
15. Klossek JM, Dubreuil L, Richet B, Sedaillan A, Beutter P. Bacterioloy of chronic purulent secretions in chronic rhinosinusitis. J Laryngol Otol. 1998, 112:1162-6.
16. Orobello PW Jr, Park RI, Belcher LJ et al. Microbiology of chronic sinusitis in children. Arch Otolaryngol Head Neck Surg. 1991, 117:980-3.
17. Nadel DM, Lanza DC, Kennedy DW. Endoscopically guided cultures in chronic sinusitis. Am J Rhinol. 1998, 12:233-41.
18. Wald ER. Chronic sinusitis in children. J Pediatr. 1995, 127:339-47.
19. Performance Standards for Antimicrobial Susceptibility Testing; Ninth Informational Supplement M100-S9. Wayne, PA, National Committee for Clinical Laboratory Standards (NCCLS), 1999.
1. In course for Medicine Master's Degree. Otorhinolaryngologist doctor.
2. Otorhinolaryngologist Master and Doctoral Degree in Medicine Professor of the Post-Graduation Program in Medical Sciences at UFRGS.
3. Otorhinolaryngology Medicine Doctor's Degree. Head of the Otorhinolaryngology and Head and Neck Surgery Department of the Clinics Hospital of Porto Alegre.
4. Doctor's Degree in Mycology. Assistant Professor at Fevale.
5. Medicine Doctor's Degree. Head Professor at UFGRS.
6. Medicine Doctor's Degree. Assistant Professor of the Medicine College of UFRGS.
Institution: Hospital Minhos de Vento de Porto Alegre. Porto Alegre / RS - Brazil.
Mail address:
Afonso Ravanello Mariante
Rua Desembargador José Bernardo de Medeiros, 29 - Bairro Boa Vista
Porto Alegre / RS - Brazil - Zip code: 91340-170
Telephone: (+55 51) 9244-7509 - (+55 51) 3327-7030 - Fax: (+55 51) 3327-7074
E-mail: afmariante@hotmail.com
Article received on October 12, 2008.
Approved on November 27, 2008.
|
|
 |
|
|