INTRODUCTIONThe nose and paranasal sinuses cystic adenoid carcinoma represents a great defiance for the early diagnosis and precise treatment. They correspond to 1% of the head and neck region malignant tumors (2,6,8), and are uncommon in the sphenoid sinus (2%) (9). The tumor has a low growth, however the neural invasion, remote metastases and multiple recurrences are common (1,7,8). The female sex is the most affected and its peak of incidence occurs in the fifth decade (1,3,6,8). The choice treatment is the radical surgery and post-operative radiotherapy (8). This is a report of a case of sphenoid sinus cystic adenoid carcinoma in a black, 6-year-old man.
CASE REPORTNLB, a male, black, 62-year-old patient sought the otorhinolaryngology service with a six-month history of self-limited and of slight quantity bloody rhinorrhea. Associated with the case, he mentioned bilateral sporadic nasal obstruction which worsened with the exposure of environmental allergens, as well as sneezes and coryza. He denied nasal pruritus. The exam presented a septum deviation to the left associated with lower infundibula hypertrophy. The nasofibroscopy confirmed a polypoid aspect tumor in the left nasal cavity with suggestive insertion to the septum and spheno-ethmoidal recess. The face sinuses computerized tomography showed an image of soft parts density that occupied a large part of the left nasal cavity, septum back wall, ethmoid sinus, and invading the frontal wall of the left sphenoid with bone erosion signals (Picture 1). The patient was submitted to intranasal endoscopic biopsy. We could observe the left sphenoid front wall invasion, which was friable and the tumor invading the sphenoid floor with approximately 0.3 cm away from the left internal carotid impression. The patient evolves without intercurrences with hospital discharge.
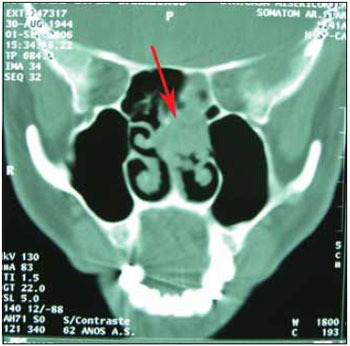
Picture 1. Coronal cut face TC - Image of soft parts density that occupies a large part of the left nasal cavity, septum back wall, ethmoid sinus, and invading the frontal wall of the left sphenoid with bone erosion signals.
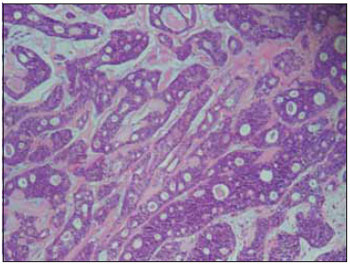
Picture 2. Blade picture - Histological cut showing: the hyalinized conjunctive tissue stroma, with tubular aspect. (HE x 100).
The anatomopathologic exam revealed cystic adenoid carcinoma.
The patient was forwarded to the oncology service.
DISCUSSIONIn the course of this century, three histopathologic variants of the Cystic Adenoid Carcinoma were found, and the solid pattern has a more aggressive clinical evolution (1,3,5,6).
It occurs more frequently between the fourth and the seventh decade of live with a peak in the fifth decade, which coincides with the age of our patient, and the female sex is the most affected in the proportion (2,5: 1) (5), diverging from the sex of our case. The most affected parts are the minor salivary glands and the submandibular glands (1,3). The cystic adenoid carcinoma is an uncommon tumor on the sphenoid (9).
Some important factors for the prognosis of the Cystic adenoid carcinoma are: anatomic location, size, involvement or not of adjacent structures, cellular atypia grade, surgical margins and the presence of metastasized ganglions (1,2,4,6).
The diagnosis delay has been ascribed to the disease's symptoms that frequently take the aspects of chronic sinusitis (2,4).
In the diagnosis, the preoperative and postoperative staying and evaluation, the magnetic resonance and the computerized tomography of these lesions play a basic role, and define the neoplasm anatomic extension and the adjacent structures integrity (2,4,5).
The Cystic adenoid carcinoma treatment consists of four distinct modalities: surgery, radiotherapy, chemotherapy and combined therapy (5). The treatment with surgery and postoperative radiotherapy (4,7), compared to those only treated with surgery, has been presenting better results (1). The benefit with the use of chemotherapy is not yet defined (4).
In this case, there was large tumor lesion, whose surgical exeresis was impracticable due to the oncologic safety margins, then lesion biopsy was carried out and the patient was forwarded for radiotherapy. After 2 years of treatment the patient presented no recurrence.
As far as our case is concerned, we considered the importance to perform the differential diagnosis between nasosinusal chronic infection and nasosinusal tumors.
FINAL CONSIDERATIONSThe cystic sphenoid carcinoma is an uncommon tumor. Therefore, patients older than 50 years, with chronic sinusitis symptoms and paranasal sinuses tumor must recall the cystic adenoid carcinoma as a diagnostic possibility.
BIBLIOGRAPHICAL REFERENCES1. Gonçalves J, Fonseca G, Serafim P, Costa MA, Aires M, Fernandes T. Carcinoma Adenóide Cístico dos Seios Paranasais. Rev Bras Otorrinolaringol. 1998, 64(3):291-293.
2. Baptista AC, Marchiori E, Boasquevisque E, Lassance CE. Comprometimento Óbito-Craniano por Tumores Malignos Sinonasais: Estudo por Tomografia Computadorizada. Radiol Bras. 2002, 35(5):277-285.
3. Brunori A, Scarano P, Iannetti G, Chiappetta F. Dumbbell Tumor of the Anterior Skull Base: Meningioma? No, Adenoid Cystic Carcinoma! Surg Neurol. 1998, 50:470-474.
4. Chagas JFS, Rapoport A. Resultados do Tratamento Cirúrgicos dos Tumores da Base do Crânio. Estudo de 43 Casos. Rev Bras Otorrinolaringol. 1995, 61(6): 453-476.
5. Santos MESM, Ibrahim D, Silva Neto JC, Silva UH, Sobral APV. Adenoid Cystic Carcinoma: A Case Report. Rev. Cir. Traumatol. Buço-Maxilo-Fac, Camaragipe. 2005, 5(2):49-54.
6. Alves ATNN, Soares FD, Silva Junior A, Medeiros N, Milagres A. Carcinoma Adenóide Cístico: Revisão da Literatura e Relato de Caso. J Brás Patol Méd lab. 2004, 40(6):421-424.
7. Pommier P, Liebsch NJ, Deschler DG, Lin DT, McIntyre JF, Barker FG, Adams JA, Lopes VV, Varvares M,Loeffler JS, Chan AW. Proton Bean Radiation Therapy For Skull Base Adenoid Cystic Carcinoma. Arch Otolaryngol Head Neck Surg. 2006, 132:1242-1249.
8. Amorim RFB, Silva LYC, Freitas RA. Aggresssive Clinica lCourse of Adenoid Cystic Carcinoma. Amorim et al. Revista Brasileira de Patologia Ora. 2003, 2(2):17-20.
9. DeMonte F, Ginsberg LE, Clayman Gl. Primary Malignant Tumors of the Sphenoid Sinus. Neurosurgery. 2000, 46(5):1084-91.
1. Training Coordinator of Otorhinolaryngology for INOOA Professor of the Otorhinolaryngology Discipline of EBMSP - Escola Bahiana de Medicina e Saúde Pública Head of the Clinical Personnel of Hospital Santa Izabel - Santa Casa de Misericórdia de Salvador - Bahia. Preceptor of the INOOA's Otorhinolaryngology Service Preceptor of the INOOA's Otorhinolaryngology Service
2. Otorhinolaryngologist - SBORL. Preceptor of the INOOA's Otorhinolaryngology Service
3. Otorhinolaryngologist - SBORL. Assistant Doctor - INOOA.
4. Master's Degree in Internal Medicine at the Federal University of Bahia - UFBA. Preceptor of Scientific Methodology of INOOA.
5. Medicine Resident Doctor.
Institution: INOOA - Instituto de Otorrinolaringologia Otorrinos Associados. Salvador / BA - Brazil.
Mail address:
Fabio Siqueira Costa Almeida
Avenida ACM, 2603 - Ed. Ventura de Matos
Salvador / BA - Brazil - Zip code: 40280-000
Telephone: (+55 71) 3270-8000 - Fax: (+55 71) 3270-8020
E-mail: fabioscalmeida@yahoo.com.br
Article received on September 23, 2007.
Approved on September 25, 2008.

