INTRODUCTIONDue to a high number of Brazilians with systemic artery hypertension (SAH), health professionals are concerned about researching implication from such disease and prevent its secondary disturbances that might reduce quality of their lives.
SAH is one of the most circulatory problems that causes peripheral and/or central involvement of the hearing and/or vestibular system (1).
For adults over 18 years, the acceptable values are: below 90mmHg of diastolic pressure and below 140mmHg of systolic pressure (2).
SAH can cause secondary injuries that lead to artery muscular hypertrophy with a gradual reduction of oxygenation and a probable increase of vasospasm, transient ischemia, oedema and focal necrosis and microaneurysm development. Such complications can result a reduction of inner ear oxygenation. Hypertension affects around 20% of Brazilian adult population (3).
Dizziness is the sensation of body balance alteration. It can be rotatory (vertigo) or non-rotatory (instability, oscillation, etc.). Both can arise from primary or secondary vestibular disorders, what is easy to be proved by vestibular exam (4).
Vertigo is the main type of dizziness from vestibular system. It can be objective, when patient notices things spinning around him/herself or subjective, when patient feels like they are spinning. 10% of world population suffers from vertigo, and more than one third will feel it sometime, that is why it is the most frequent symptom.
People who suffer from high blood pressure present symptoms. Therefore, symptoms such as headache, tachycardia, dizziness, nystagmus, vertigo and vomit can arise especially from hypertensive crisis (1,2,5).
Otoneurological symptoms of vestibular diseases arising from vascular problems can be mild, moderate or severe, even on patients free from cardiovascular problem. Regarding personal and family history, it can be related with family predisposition (1).
Studies on antihypertension therapy present vertigo as one of the most frequent reactions (6).
Advances of imaging diagnosis have replaced functional tests, what did not occur with otoneurological exam, which is still important on clinical evaluation of patients with hearing functional disturbances and body balance (5).
MATERIAL AND METHODS 17 patients with SAH, under medicine therapy, were examined. 11 females of them were and 6 were males, aging from 22 to 76 year. They were sent from Unidade de Saúde Ouvidor Pardinho and from community to Laboratório de Otoneurologia da Universidade Tuiuti - Paraná (Otoneurology Laboratory).
After authorization from Institutional Ethics Committee and signing a Free and Clear Consent Term, patients were submitted to the following procedures:
AnamnesisA questionnaire focusing otoneurological signs and symptoms, which were personal and family history was applied.
ENT EvaluationIt was performed with the target of eliminating any alteration that might interfere on vestibular exam.
Vestibular ExamPatients were submitted to the following tests:
Without Record- Nystagmus and positional vertigo through Brandt and Daroff´s maneuver were researched (7).
- Spontaneous and semi-spontaneous nystagmus with open eyes, at frontal look and at 30° of deviation to right and left, up and down.
With RecordTo perform vectoelectronistagmography, it was used a Berger thermosensitive device, VN316 model, with three record channels. After cleaning skin of periorbitary areas using alcohol, an active electrode is attached with electrolytic paste to the lateral angle of each eye and frontal medium line, forming an isosceles triangle, which made the identification of oblique, vertical and horizontal eye movements possible. This type of VENG has enabled in obtaining more accurate measurement of slow component speed (vestibular correction) of nystagmus.
It was also used a Ferrante adjustable height pendular swivel chair, a Neurograff visual stimulator, EV VEC model, and a Neurograff air otothermometer, NGR 05 model.
The following eye and labyrinth tests at VENG were performed according to PADOVAN AND PANSINI´S (8) and MANGABEIRA-ALBERNAZ´S et al. (9) criteria.
- Eye movement calibration in order to obtain tracking regularity, what could make researches comparable among themselves.
- Spontaneous nystagmus (eyes open and closed) and semi-spontaneous nystagmus (eyes open) research in order to evaluate occurrence, direction, inhibiting effect of eye fixation, and the value of angular speed of the maximum slow component of the nystagmus.
- Pendular tracking research to evaluate occurrence and type of curve.
- Optokinetic nystagmus research at a speed of 60º per second, at clockwise and anti clockwise rotation in horizontal direction. It was evaluated: occurrence, direction, value of angular speed of the maximum slow component at clockwise and anticlockwise rotation of the nystagmus.
- Pre- and post-rotatory nystagmus research at descending pendular rotatory test, stimulating lateral, anterior and posterior semicircular ducts. In order to stimulate lateral semicircular ducts (horizontal), head was bent 30o to front direction. Next, head was bent 60o back and 45o to right, and then 60o back and 45o to left, respectively to soothe anterior and posterior semicircular (vertical) ducts. It was observed: occurrence, direction, frequencies to clockwise and anti-clockwise rotation of the nystagmus.
- Research of pre and post-caloric nystagmus, performed on patients positioned with head and trunk leaned backwards at 60º, in order to properly stimulate lateral semicircular ducts. The time spent on each ear for air irrigation at 42°C, 20°C and 10°C 80s for each of the temperatures and the responses were recorded with eyes closed and then opened in order to observe EIFO (inhibiting effect of eye fixation). It was observed: direction, accurate values of VACL (value of angular speed of the maximum slow component) and the calculation of relations from directional preponderancy and labyrinth predominance of post-caloric nystagmus.
Statistical AnalysisProportional Difference Test was applied with the purpose of comparing results from caloric test (analyzing absolute and relative values) and results from vestibular exam. The level of rejection on voided hypothesis was established at 0.05% or 5%.
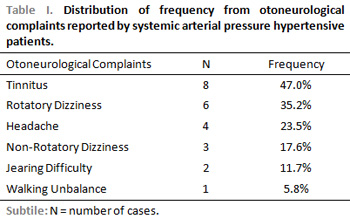
RESULTSThe main otoneurological complaints reported by patients on anamnesis were: tinnitus (47.0%), rotatory dizziness (35.2%) and headache (23.5%), as displayed on Table 1.
All patients reported SAH family history.
Results from research of positional nystagmus, eye movement calibration, spontaneous nystagmus with open and closed yes, semi-spontaneous nystagmus with open eyes, pendular tracking, optokinetic, pre- and post-rotatory nystagmus were normal. Abnormal findings at VENG were essentially on caloric test.
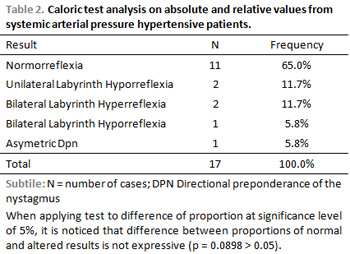
Regarding caloric test, eleven cases (65.0%) presented normorreflexia, two cases (11.7%) presented unilateral labyrinth hyporreflexia, two cases (11.7%) presented bilateral labyrinth hyperreflexia, one case (5.8%) bilateral labyrinth hyporreflexia and one case (5,8%) presented directional preponderance of asymmetric nistagmi according to Table 2. According to Difference of Proportions Test, there was no expressive difference when analyzing caloric test.
Alterations seen in vestibular exam occurred on peripheral vestibular system.
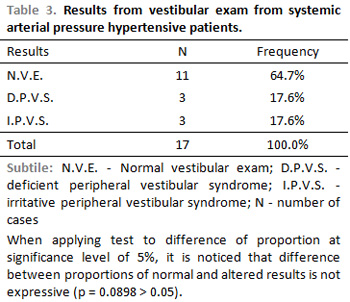
Regarding results from vestibular exam, 11 patients (65.0%) presented normal vestibular exam, three (17.6%) presented deficient peripheral vestibular syndrome and three (17.6%) presented irritative peripheral vestibular syndrome, according to Table 3. According to Difference of Proportions Test, there was no expressive difference when analyzing caloric test.
DISCUSSIONThe main symptoms reported by patients were: tinnitus (47.0%), rotatory dizziness (35.2%) and headache (23.5%), what can be seen on 1. Colafemina and Grellet (10) studied 50 patients and noticed predominance of vertigo in 88.0% of patients, headache in 74.0%, tinnitus in 52.0% and non-rotatory dizziness in 26.0%. Caovilla et al. (11) evaluated 542 patients with cardiovascular problems, 270 from those with SAH. Vestibular symptoms occurred in 186 cases (34.3%). Brohem et al (12) evaluated 50 patients with SAH and noticed vertigo in 40 cases, non-rotatory dizziness in 34 cases, headache in 21 cases and tinnitus in 18 cases. Parfenov (13) evaluated 285 hypertensive patients and reported vertigo as the main symptom. It was noticed that vertigo was the most aggressive symptom. According to Colafemina and Grellet (10) vestibular symptoms usually occur when high level of blood pressure tend to rise.
Regarding labyrinth test, there was alteration in 35.0% of patients only at caloric test and on peripheral vestibular system with occurrence similarities of deficient and irritative peripheral vestibular syndromes, according to Tables 2 and 3.
It was noticed in the researched literature that some test that compose labyrinth test, such as positional vertigo highlighted by Colafemina and Grellet (10), Caovilla et al. (11) and Brohem et al. (12). Irregularity on eye movement calibration and supression of optokinetic nystagmus were observed by Caovilla et al. (11). Research on spontaneous nystagmus (eyes open and closed), semi-spontaneous nystagmus (eyes open), pendular track and perrotatory nystagmus presented normal results agreeing with authors´ findings. Regarding caloric test, it was observed normorreflexia, hyperreflexia, uni and bilateral labyrinth hyporreflexia and directional preponderance of asymmetric nistagmus, according to literature (10-12). Besides these alterations, uni and bilateral arreflexia was also observed.
In the studied literature, only Ohashi et al. (14) found higher prevalence of central findings on the hypertensive group of people, but not referring in which labyrinth tests.
CONCLUSIONSa) The most highlighted otoneurological symptoms were: tinnitus (47.0%), rotatory dizziness (35.2%) and headache (23.5%);
b) Vestibular exam presented alteration in six patients (35.0%) only on caloric test;
c) There was a prevalence of alteration on peripheral vestibular system;
d) There was occurrence similarity of irritative and deficient peripheral vestibular syndrome.
Although an expressive number of alteration on labyrinth test was not found, one might be aware of this disease, which is subtle and has been often arising on young population.
REFERENCES1. Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG, Settanni FAP. Vestibulopatias de origem cardiovascular. In: Silva MLG, Muhoz MSL, Ganança MM, Caovilla HH. Quadros clínicos otoneurológicos mais comuns. São Paulo: Atheneu: 2000. p.55-61.
2. Consenso Brasileiro de Hipertensão Arterial. [Site na Internet] Disponível em: http://www.manuaisdecardiologia.med.br/
has/pag1/shtml. Acessado em 22 de fevereiro de 2005.
3. Nobre F, Mion JRD. Hipertensão arterial: Avaliando a dimensão do problema. In: Nobre F, Mion JR D. Risco cardiovascular. São Paulo: Lemos Editorial: 2001 p.23-6.
4. Ganança MM, Caovilla HH. A múltipla abordagem terapêutica. In: Ganança MM. Vertigem tem cura? São Paulo: Lemos: 1998. p.59-61.
5. Ganança MM, Caovilla HH. A vertigem e sintomas associados. In: Ganança MM, Vieira RM, Caovilla HH. Princípios de otoneurologia. São Paulo: Atheneu: 1998. p.3-6.
6. Israilli ZH. Clinical pharmacokinetics of angiotensin II (AT1) receptor blockers in hypertension. Am J Hypertens., 2000, 14(1):73-86.
7. Brandt T, Daroff RB. Physical therapy for benign paroxysmal positioning vertigo. Arch Otolaryngol Head Neck Surg, 1980, 106:484-5.
8. Padovan I, Pansini M. New possibilities of analysis in electronystagmography. Acta Otolaryngol., 1972, 73:121-5.
9. Mangabeira-Albernaz PL, Ganança MM, Pontes PAL. Modelo operacional do aparelho vestibular. In: Mangabeira- Albernaz PL, Ganança MM. Vertigem. 2.ed. São Paulo: Moderna: 1976. p. 9-36.
10. Colafemina JF, Grellet M. A função do labirinto anterior e posterior no paciente com hipertensão arterial. Rev. Bras. Otorrinolaringol, 1985, 51(1):27-30.
11. Caovilla HH, Ganança MM, Mangabeira-Albernaz PL. Vectonystagmographic findings in acute and chronic cardiovascular disturbances. Vertigo, náusea, tinnitus and hearing loss. Vasc Dis., 1986, 43:105-9.
12. Brohem VMA, Caovilla HH, Ganança, MM. Dos sintomas e achados audiológicos e vestibulares em indivíduos com hipertensão arterial. Acta Awho, 1996, 15(1):4-10.
13. Parfenov VA. Differential diagnosis and treatment of vertigo in hypertensive patients. Ter Arkh., 77(1):56-9, 2005.
14. Ohashi N, Imamura J, Nakagawa H, Mizukoshi K. Blood pressure abnormalities as background roles for vertigo, dizziness and disequilibrium. ORL J Otorhinolaryngol Relat Spec, 1990, 52(6):355-9.
1. PhD in Human Communiaction Disorder by UNIFES/Escola Paulista de Medicina (Coordenator of the Mastering and Doctorate Program in Communiaction Disorder - Universidade Tuiuti - Paraná)
2. PhD in Anatomy by UNIFES/Escola Paulista de Medicina (Adjunt Professor Coordenator of the Mastering and Doctorate Program in Communiaction Disorder - Universidade Tuiuti - Paraná)
3. Master in Communiaction Disorder by Universidade Tuiuti - Paraná
4. Majored in Phonoaudiology by Universidade Tuiuti - Paraná.
Laboratório de Otoneurologia da Universidade Tuiuti - Paraná (UTP)
Bianca Simone Zeigelboim
Address: Rua Gutemberg, nº99 9º and. - CEP 80.420.030 - Curitiba/Pr Tel / Fax: (41) 3331-7807 E-mail: bianca.zeigelboim@utp.br
This article was submitted to SGP - Sistema de Gestão de Publicações (Publication Management System) from RAIO on August 8, 2006 and was approved on September 1, 2006 07:44:13.