INTRODUCTIONThe physical equilibrium is the human ability to maintain him/herself upright or perform movements of body acceleration and rotation without oscillating or falling down. Posture maintenance is guaranteed by the sensorimotor interaction (1) and the relevant information related to the physical equilibrium depends on the visual, somatosensory and vestibular systems (2).
Usually, the control of equilibrium is 'automatically' made without requiring a permanent attention. When automatic equilibrium is broken, it is needed to perform an intense and conscious effort to try to overcome the abnormal sensations and keep the control of equilibrium.
The equilibrium alterations can occur as a result of some failure in one or more systems, taking the individual to complain about physical disequilibrium. These complaints are extremely frequent and have dizziness as their main symptom (3). The etiology of dizziness can be related to a number of causes with or without a vestibular background, like cerebral dysfunctions.
The loss of postural stability can occur due to diseases found in different organs or tissues, which will influence in the normal function and determine the clinical manifestations, evolution and prognosis. The diseases are originated by several reasons, and they can be originated from traumas, predisposition, nutritional, environmental and genetic factors, or even by unknown causes still by medicine (5). The diseases, however, can affect the central nervous system (CNS), the peripheral nervous system (PNS) and the musculoskeletal system, impairing the individual's equilibrium and the posture (6).
Parkinson's disease (PD) is found among SNC's impairments, and it can be one of the multiple causes of alterations in the physical equilibrium, which is defined as a progressive neurological affection and it can be essentially characterized by motor symptoms, and the etiology is still unknown (7). It is known that there is a reduction of dopamine produced by the black matter. Through aging, the speed to conduct the nervous impulses is reduced, and there is a subsequent alteration in the neurotransmitters as well (8). The lack of dopamine (neurotransmitter acting in the nuclei of the base) causes PD, provoking an inefficient control of the movements. The consequent alterations in the motor control become noticeable, resulting in relaxation tremor, rigidity, akinesia, alteration of postural reflexes, instability and disorders of equilibrium and walk, among other symptoms (7). Additionally, it impairs the ability of the central nervous system to process the vestibular, visual and proprioceptive signs responsible for maintaining the physical equilibrium, by reducing the ability to modify the adaptating reflexes (9). A population presenting several vestibular dysfunctions is the one with Parkinson, who can also develop labyrinth symptoms because of its pharmacotherapy (10).
Hence, the close relationship between PD and the vestibular alterations and the physical equilibrium justifies this study, which has the objective to evaluate the physical equilibrium in Parkinson patients.
METHODThe present study is registered in the Ethical and Research Committee under Nº 0200.0.243.000.07. The study group was comprised of patients agreeing to participate in the research after knowing it, by executing a free and clarified agreement term.
12 individuals with a Parkinson diagnosis were evaluated and served in the neurology department of a local university hospital. Firstly, a survey was performed in the files of the neurology department in the period between 01/01/2007 and 05/31/2008, to verify patients diagnosed with the disease, and all of them were invited to participate in the research. Those with secondary Parkinson, other evident neurological or mental alterations, amputation of any member, severe visual deficiency or any other alteration that could impair the understanding and performance of the proposed tasks were excluded. The presence of any kind of alteration in the nose and/or throat, ear or the utilization of drugs and alcohol was also considered an exclusion criterion.
The study group was evaluated according to gender, findings about static and dynamic equilibrium, coordination of movements, dynamic posturography (DP) and vestibular examinations in evaluation. Age group, time of disease and type of treatment were disregarded.
As a result, search was made for healthy people without otoneurological complaints for purposes of composing the control group to control the results of dynamic posturography. The control group was comprised of the same number of individuals, same gender, similar ages to the study group and the same exclusion criteria of the study group were followed.
The performed procedures were otoscopy inspection of external auditive meatus to verify the likely presence of cerumen surplus or alteration in the middle ear, which could interfere with the results of the examinations. In case cerumen surplus was found or alteration in the middle ear was suspected, the patient would be submitted to the otorhinolaryngologist doctor. After removing the cerumen or the treatment, the patient would return to continue evaluations.
Evaluation of the static and dynamic equilibrium and coordination of movements were performed by way of the described evidences, according to MANGABEIRA & GANANCA (11), which were firstly performed with open eyes and then closed eyes, for 20 seconds in each situation. They are: Walking Test, Romberg Test, Romberg-Bare, Unterberger test, Stretched Arm Test, Diadocokinesis Test and Dysmetria Test - index-knee-nose.h
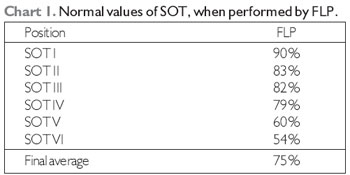
The dynamic posturography developed by Castagno (12), Foam-laser Dynamic Posturography (FLP), was also used to evaluate the equilibrium and its relations with the visual, proprioceptive and vestibular systems. It consists of a simple technique to evaluate the sensorial organization, preformed by way of 06 (six) tests called sensorial organization tests (SOT).
The reference values for FLP in each SOT position separately and its final average were described at Table 1, according to CASTAGNO (12), who carried out his study with young adults.
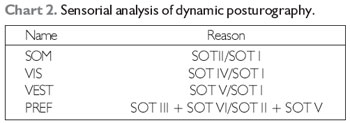
Another way to perform the sensorial analysis through FLP is to demonstrate the individual's ability to use the somatosensory (SOM), visual (VIS), and vestibular (VEST) systems, as well as the visual preference (PREF) to maintain the orthostatic equilibrium, considering normal the values higher than 92% to SOM, 88% to VIS, 67% to VEST and 95% to PREF. The table 2, according to Castagno (12), shows the ways to evaluate SOM, VIS, VEST and PREF.
To perform the vestibular examination, it was used the Computed System of Vectoelectronystagmograph SCV 5.0 proposed by CASTAGNO (12). The evidences performed with the patients in this research were the following, as indicated by MOR (13): Calibration of ocular movements (CAL), spontaneous nystagmus (SN), semi-spontaneous nystagmus (SEN) or directional nystagmus (DN), pendulum trace (PT), optokinetic nystagmus (ON), decreasing pendulum rotary test (DPRT) and caloric proof.
In the evaluation of static, dynamic equilibrium and vectoelectronystagmograph, the results were descriptively analyzed placed into charts and tables.
To verify the possible differences between the study group and the control group in the variations of dynamic posturography, the non-parametric Kruskal-Wallis test was used, in which a significance level of 5%, i.e., p<0.05 was adopted. The statistically significant values were emphasized by using an asterisk.
RESULTS12 individuals were evaluated, out of whom 7 (58.3%) were male and 5 (41.7%) were female. The age group varied between 44 and 79, an average of 65.5 years of age. The time living with the symptoms varied between 1 and 20 years. As to patients' age when PD was discovered, 4 individuals found the disease at an age between 40 and 50, 4 between 50 and 60 and 4 above 60.
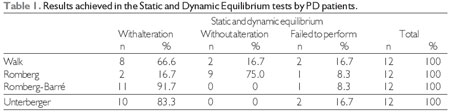
AT Table 1, the results achieved in the static and dynamic equilibrium tests were exposed.
The two patients who did not succeed in performing the static and dynamic tests showed difficulties in locomotion. One showed difficulties in starting the movements and the other one used a wheel chair, due to PD injuries.
Among 8 (66.6%) patients with alteration in the walking test, all of them had deviations; among 11 (91.7%) patients with alteration in Romberg-Bare test, all fell down. Among 10 (83.3%) patients with alteration in Unterberger test, 7 had an improvement and 3 had a deviation.
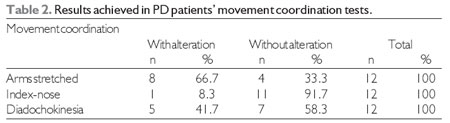
Table 2 shows the results achieved in PD patients' movement coordination tests.
Among 8 (66.7%) patients with alteration in the stretched arm test, 6 lowered both arms and 2 also had deviations of both arms. In the index-nose text, dysmetria occurred and in diadochokinesia the alteration found was dysdiadochokinesia.
As to the results of vectoelectronystagmograph, Parkinson patients did not show an alteration in the horizontal and vertical calibration, and this also occurred in the spontaneous nystagmus test, in which all of them were absent; only 2 patients showed nystagmus with their eyes closed with VACL values=5º/s, what can be regarded as normal. They did not show any alteration in the research of semi-spontaneous nystagmus and optokinetic nystagmus either.
In the research of horizontal pendulum trace, among the 12 evaluated patients, 6 showed trace type I, 3 showed trace type II and three showed trace type III. In the research of vertical pendulum trace, 4 showed trace type I, 4 showed trace type I, 4 type II and 4 and type III.
The pre-surgical nystagmus showed 9 cases of symmetry and 3 cases of directional prevalence.
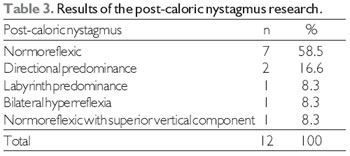
As to the research of post-caloric nystagmus, 7 (58.5%) patients did not show any alteration and 5 (41.5%) showed an altered result. Table 3 shows results of post-caloric nystagmus of PD patients.
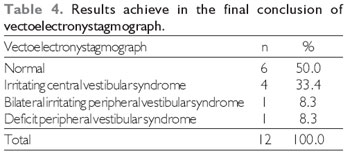
When concluding the vectoelectronystagmograph examination, 6 (50.0%) patients showed an altered examination and 6 (50.0%) had an examination without any alteration, and among the 6 altered patients, 4 had central vestibular syndrome and 2 had peripheral vestibular syndrome. At Table 4, results achieved in the final conclusion of PD patients' vectoelectronystagmograph were found.
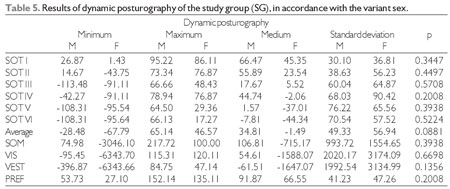
With respect to the results of dynamic posturography, among the 12 patients, 11 performed this test, because a patient had a physical limitation and she could not perform this task. At Table 5, the results of dynamic posturography of the study group (SG) were verified, in accordance with sex variation.
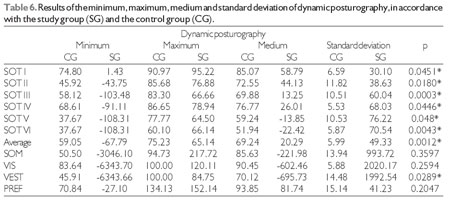
Table 6 shows the results of dynamic posturography of the study group (SG) and the control group (CG).
DISCUSSIONIn relation to sample, it was observed that the highest number of individuals was concentrated in the male sex, what is equivalent to the registration made by FAHN & PRZEDBORSKI (14); they affirmed that men are more affected than women and they can have a 3:2 proportion. For other authors (15), PD has a universal character and they can impact both sexes, different races and they can occur regardless of social class.
Regarding patients' age when PD was discovered, 4 individuals found the disease aged between 40 and 50, 4 between 50 and 60 and 4 above 60. The prevalence of the disease increases with the population's age and it usually starts around 55 years of age, and it attacks the individual in the full working and life enjoyment stage. Several authors (16) also referred that PD prevalence increases through age, and the average age of disease is around 55 years in both sexes and has a wide range of age, from 20 to 80. For O'SULLIVAN (17), average age when the disease starts is around 58 and 60, although a smlall percentage can be affected by the diseases at 40 years of age, even 30. In the present research, no patient was under 40 years of age or nor anyone had a diagnosis before that age and it was neither observed a higher number of individuals affected when age increased. In this study, it was not considered for statistical analysis the patients' age group because of the small sample; however, stratification per age can be made in further studies in which a higher number of patients can be achieved.
In the findings of the walking test, most patient showed an alteration, and deviation was found in all cases; Romberg test resulted in small difficulties in comparison with Romberg-Barré test, in which almost all the patients showed an altered result, and they all fell down, such a fact can be justified by the increase of the difficulty of this test in comparison with Romberg test and by the muscular rigidity of Parkinson patients, what by compromising the stem muscles determines serious alterations such as curve and projection of the body forward (propulsion) and backward (retropulsion) that are alterations of posture that can cause a downfall backward and forward., respectively (18). In Unterberger test, alterations found were advancements followed by deviations. These findings corroborate with VOLPI & NAVARRO (19), who performed a case study with the purpose of applying vestibular rehabilitation in patients with benign paroxysmal positional vertigo (BPPV), without any associated disease and another with PD associated. Among the evaluations, the test of static equilibrium was performed by way of Romberg and Romberg-Bare tests and the dynamic equilibrium test was performed by way of Babinksi-Weil test. In the firstly performed equilibrium tests, the PD patient showed an anteropulsion in Romberg test, lateropulsion on the right in Romberg-Bare and walking deviation on the right in Babinsky-Weil test.
In this research, an alteration was found in PD patients' dynamic equilibrium tests, what corroborates with another study (6), in which the dynamic equilibrium of different neurological patients was quantitatively evaluated, among them those with PD, by way of Get Up and Go test (GUGT). The researchers did not find a statistically significant difference in comparison with the dynamic equilibrium between the studied diseases. For them, maybe it has occurred as a result of the low sampling, although they observed that all participants in the study were able to walk a three-meter distance, however they did not succeed in completing the distance with a time equal to or below ten seconds, a time estimated for a healthy individual. In PD patients, average was 17 seconds. In accordance with the authors' findings, it is possible to say that the dynamic equilibrium is affected in neurological diseases, and it can cause difficulty in performing their daily activities (DA) and practical life activities (PAA).
With respect to the results achieved in the movement coordination tests, patients showed difficulties in coordinating the movements of stretched arm tests, besides dysdiadochokinesia followed by an alteration in the index-nose test. PD is characterized by a degeneration of the black matter and other pigmented nuclei in the brainstem. As a result, there is a reduction of the cerebral dopamine, creating in PD individuals manifestations that are concentrated in a poor control of movements (20). It is important to emphasize that these tests are complementarily relevant, for the possibility of providing additional topodiagnostic information in contrast with other data of the vestibular function examination and never separately (21).
As to the results of vectoelectronystagmograph, the biggest alterations are related to the research of post-caloric nystagmus, in which 5 (41.5%) of the patients had an altered result, 2 of whom (16.6%) were cases of directional prevalence. The findings of this study partially agree with BASSETO et al.'s reports (22), who found alterations in PD patients'' vestibular examination, which mostly occurred in the caloric test, however prevalently in the bilateral labyrinth hyporeflexia.
REICHERT et al. (23) developed a study with 36 PD patients and they found a higher incidence of hyporeflexia and areflexia followed by the prevalence of labyrinth and hyperreflexia. Additionally, the present research greatly differs from that study, since it did not find hyporeflexia and areflexia as a relevant finding, but it noticed the prevalence of labyrinth and hyperreflexia.
In the present research, among the 12 evaluated, 6 (50.0%) were found with an altered examination, and in a higher proportion the central vestibular syndrome. BASSETO et al. (22), evaluating 30 PD patients, they observed the occurrence of nine cases of bilateral peripheral vestibular deficit syndrome; six cases of unilateral peripheral vestibular deficit syndrome; six cases of unilateral irritating peripheral vestibular syndrome; five cases of normal vestibular examination; two cases of bilateral irritating peripheral vestibular syndrome; one case of bilateral irritating central vestibular syndrome, and one case of bilateral central vestibular deficit syndrome.
In another study by BASSETO et al. (24), a research was performed in order to verify the efficiency of the vestibular rehabilitation exercises by way of the pre- and post-evaluation of the Dizziness Handicap Inventory questionnaire, Brazilian adaptation, in PD patients. PD patients were submitted, among the procedures, to the vestibular examination by way of vectoelectronystagmograph. With respect to the evaluation of the vestibular function, an alteration was found in all the elderly (100%) with a prevalence of unilateral labyrinth hyporeflexia (37.5%) in the group A (submitted to CAWTHORNE E COOKSEY) exercises) and bilateral (25.0%) in the group B (submitted to Herdman exercises) followed by labyrinth hyperreflexia (25%). In the vestibular examination, it turned evident the frequency of the peripheral vestibular deficit syndrome in both groups, in five patients (62.5%) out of the 8 evaluated.
Concerning the results of the dynamic posturography in the study group (SG), in accordance with the variation sex, it was verified that there is neither a statistically significant difference in no SOT condition and nor with respect to the use of somatosensory (SOM), visual (VIS), vestibular (VEST) systems and the degree of visual preference (PREF) to maintain the orthostatic equilibrium. In the researched literature, there are reports that men or women suffer, in a higher or lower proportion, the alterations related to PD physical equilibrium.
When compared the study group with the control group, it was verified a statistically significant difference (p<0.05) in all SOT, in the average and utilization of the vestibular system (VEST), what was not applied to use the somatosensory (SOM), visual (VIS), vestibular (VEST) systems and the degree of visual preference (PREF) to maintain the static equilibrium, thus indicating alterations in PD equilibrium, especially related to the difficulty of these patients in using the vestibular system.
During DP, we could also observe many downfalls. This finding corroborates with those of other authors, who affirm that the alterations in the equilibrium are found in PD patients. A great deal of PD patients' shows an inadequate interaction of the systems responsible for the physical equilibrium ; vestibular, visual and proprioceptive systems; as a result of this alteration, these patients tend to move their gravity center forward, and they are unable to perform compensatory movements to regain equilibrium and thus they easily fall down (25). COUNALT-COUBOIS et al. (26) assign the difficulties in equilibrium to motor alteration of the disease as well. According to these authors, PD patient is found in a permanent conflict of central sensitive processing, because he/she comes in touch with full visual and somatosenorial information and with exaggerated galvanic vestibular reactions.
COUNALT-COUBOIS et al. (26) had the purpose of evaluating the stimulation impact of the bilateral subthalamic nucleus in the control of PD equilibrium and determining how the basal ganglia is related to the sensorimotor modifications and it works in the neurosensorial organization of the equilibrium and motor postural programming. PD patients were evaluated, among other procedures, by static and dynamic posturography, including sensorial organization and adaptation of the test, immediately before and 6 months after the bilateral implementation of the electrode inside the subthalamic nucleus. As a result, the authors observed that the static test showed an improvement in the accuracy of the postural control and the dynamic test showed the reduced number of downfalls and the patients' ability to develop more sensorimotor strategies, when they were stimulated. The sensorial organization test showed an improvement in the equilibrium and thus a better solution of the sensorial conflict. They concluded that the stimulation of the bilateral subthalamic nucleus allowed for a reduction in the rigidity and therefore an improvement in the ability to use muscular proprioception as reliable information, resulting in the suppression of the proprioceptive conflict.
YARROW et al. (27) used the pressure platform to evaluate 21 PD patients', who presented tremor in orthostatism and, as it could be influenced by the postural instability and disequilibrium, they observed that these patients showed alterations in equilibrium and posture.
ABE et al. (28) developed a researched with the insertion of analyzing the PD patients' equilibrium, slight and moderate degrees, by way of a photogrammetry and they verified a higher ratio of anterior and posterior oscillation in patients with slight degree in relation to the patient with moderate degree. They also observed that the ratio of anterior oscillation in patients with slight degree was superior to the ratio of posterior oscillation in these same patients, such a fact was not observed in the patient with a moderate degree.
PD patients' postural instability can be characterized as an alteration in the processing of sensorial stimuli, especially of the proprioceptive, vestibular and somatic systems. As PD advances, there is a loss of the postural reflexes, which caused downfalls and inability to stand upright without any help (10).
With the abovementioned studies, we observed that PD patients can develop alterations in the physical equilibrium, what, in this study, could be verified by the findings of tests of static and dynamic tests, movement coordination, vectoelectronystagmograph and especially by the findings n the dynamic posturography, indicating it is extremely useful to diagnose and investigate PD (29).
CONCLUSIONPD patients show an alteration in the physical equilibrium. Dynamic posturography proved to be more sensitive to detect the equilibrium alterations in PD patients than vectoelectronystagmograph. Computed vectoelectronystagmograph proved to be normal in half of the individuals in the study group, indicating that the labyrinth and the vestibulo-oculomotor pathways would be normal in these individuals and that the equilibrium disorder presented by them would arise from the dysfunction in other areas of the central or peripheral nervous system.
BIBLIOGRAPHICAL REFERENCES1. Pedalini ME, Bittar RSM. Reabilitação vestibular: uma proposta de trabalho. Pró- fono. 1999, 11(1):140-144.
2. Sanz EM, Guzman B, Cerverón CC, Baydal JM. Análisis de la interacción visuo-vestibular y la influencia visual en el control postural. Acta Otorrinolaringol. 2004, 55:9-16.
3. Ganança FF, Castro ASO, Branco FC, Natour J. Interferência da tontura na qualidade de vida de pacientes com síndrome vestibular periférica. Rev Bras Otorrinolaringol. 2004, 70(1):94-101.
4. Ganança MM, Caovilla HH, Munhoz MSL, Silva MLG, Ganança FF. Xeque-mate nas tonturas: A VPPB em xeque. Acta AWHO. 1997, 16(3):129-37.
5. Robbins C, Kumar C. Patologia estrutural e funcional. 6ª edição. Rio de Janeiro: Guanabara Koogan; 2000, p.1268.
6. Torriani C, Mota EPO, Gomes CS, Batista C, Costa MC, Vieira EM, Koreeda DI. Avaliação do equilíbrio dinâmico em diferentes pacientes neurológicos por meio do teste Get Up And Go. Rev Neurocienc. 2006, 14(3):135-39.
7. Brusse KJ, Zimdars S, Zalewski KR, Steffen TM. Testing functional performance in people with Parkinson Disease. Phys Ther. 2005, 85(2):134-41.
8. Westerberg BD, Roberson JB, Stach BA, Silverberg GD, Heit GH. The effects of posteroventral pallidotomy on balance function in patients with Parkinsons disease. Stereotact Funct Neurosurg. 2002, 79(2):75-87.
9. Ganança FF, Castro ASO, Branco FC, Natour J. Interferência da tontura na qualidade de vida de pacientes com síndrome vestibular periférica. Rev Bras Otorrinolaringol. 2004, 70(1):94-101.
10. Melnick ME. Distúrbios dos gânglios da base: metabólicos, hereditários e genéticos em adultos. In: Umphred, D. A. Fisioterapia neurológica. 2nd. ed. São Paulo: Manole; 1994.
11. Mangabeira Albernaz PL, Ganança MM. Vertigem. São Paulo: Moderna; 1976.
12. Castagno LA. A new method for sensory organization tests: the foam-laser dynamic posturography. Rev Bras Otorrinolaringol. 1994, 60(4):287-96.
13. Mor R, Fragoso M, Taguchi CK, Figueiredo, JFFR. Vestibulometria & Fonoaudiologia: como realizar e interpretar. São Paulo: Lovise; 2001, p.181.
14. Fahn S, Przedborski S. Parkinsonismo. In:___ Tratado de neurologia. 9.ed. Rio de Janeiro: Guanabara Koogan; 1997, cap. 115, p.768-84.
15. Kuopio A, Marttila RJ, Helenius H, Toivonen M, Rinne UK. The quality of life in Parkinson.s disease. Mov Disord. 2000, 15(2):216-23.
16. Marsden CD. Parkinson's disease. J Neurol Neurosurg Psychiatry. 1994, 56(6): 672-81.
17. O'sullivan SB. Doença de parkinson. In: O'sullivan & Schmitz, T.J. Fisioterapia: avaliação e tratamento. São Paulo, Manole; 1993, p.549-64.
18. Reis T. Doença de Parkinson: pacientes, familiares e cuidadores. Porto Alegre: Palloti; 2004, 368p.
19. Volpi FS, Navarro, FM. Um estudo de caso da reabilitação vestibular em pacientes idosos com VPPB e doença de Parkinson associada. Fisioter Mov. Curitiba. 2006, 19(2):83-90.
20. Lim LIIK, Van WEEH, Goede CJT, Jones D, Rochester L, Hetherington V, et al. Measuring gait and gait-related activities in Parkinson's patients own home environment: a reliability, responsiveness and feasibility study. Parkinsonism Relat Disord. 2005, (11):19-24.
21. Rigon, R. Achados Otoneurológicos em pacientes portadores de diabetes mellitus tipo 1. Santa Maria, 2006. 51f. Dissertação de Mestrado. (Mestrado em distúrbios da comunicação humana da Universidade Federal de Santa Maria).
22. Basseto JM, Zeigelboim BS, Jurkiewicz AL, Klagenberg KF. Achados otoneurológicos em pacientes com doença de Parkinson. Rev Bras Otorrinolaringol. 2008. 74(3):350-5.
23. Reichert WH, Doolittle J, Mcdowell FH. Vestibular dysfunction in Parkinson disease. Neurol. 1982, 32:1133-8.
24. Bassetto JM, Zeigelboim BS, Jurkiewicz AL, Ribas A, Rosa, MRD. Reabilitação vestibular em idosos com Parkinson. Rev CEFAC. 2007, 9(2):269-81.
25. Zucco F. A reabilitação vestibular no idoso. Revista Fisio&Terapia. 2003, 7(39):35-7.
26. Colnat-Coulbois S, Gauchard GC, Maillard L, Barroche G, Vespignani H, Auque J, Perrin PH P. Bilateral subthalamic nucleus stimulation improves balance control in Parkinson's disease. J Neurol Neurosurg Psychiatry. 2005, 76:780-7.
27. Yarrow K, Brown P, Gresty MA, Bronstein, A.M. Force platform recordings in the diagnosis of primary orthostatic tremor. Gait And Posture. 2001, 13(1):27-34.
28. Abe PT, Vitorino DFM, Guimarães LHCT, Cereda RA, Milagre VLR. Análise do equilíbrio nos pacientes com doença de Parkinson grau leve e moderado através da fotogrametria. Rev Neurocienc. 2002, 12(2):73-76.
29. Bittar RSM. Como a posturografia dinâmica pode nos ajudar nos casos de tontura. Arq. Int. Otorrinolaringol. 2007, 11(3):330-33.
1 Master. Phonoaudiologist.
2 Docttor. Asssistant Professor in the Degree of Phonoaudiology of Federal University of Santa Maria, Rio Grande do Sul. Phonoaudiologist.
Institution: Universidade Federal de Santa Maria. Santa Maria / RS - Brazil. Mailing address: Universidade Federal de Santa Maria - UFSM - Franciele da Trindade Flores - Rua 8 de maio, 137 - Bairro Salgado Filho - Santa Maria / RS - Brazil - ZIP Code: 97040- 360 - Telephone: (+55 55) 9916-2537 - Email: francieletflores@yahoo.com.br
Article received on September 9, 2010. Article approved on January 24, 2011.