INTRODUCTIONTinnitus is the perception of sound in the absence of a corresponding external sound source. It affects up to 15% of the population (1) across all age ranges (2,3), but is predominant in the elderly (4,5). In addition to its multiple organic causes-otologic, metabolic, neurologic, somatosensory, cardiovascular, or dental-tinnitus involves major psychological components (3,4,6,7), which are associated with the interpretation and management of the condition. Therefore, adequate diagnosis and treatment of tinnitus requires a multidisciplinary approach.
The types of tinnitus most commonly reported by patients involve the perception of pure tones (e.g., a whistling sound) or frequency ranges (akin to white noise). However, during regular otolaryngological evaluation in the Tinnitus Research Group of the University of São Paulo, some patients began reporting unusual and complex auditory perceptions such as hearing music and voices in addition to typical tinnitus.
Perception in the absence of a corresponding object is generally characterized as a hallucination. As this is a controversial topic in psychiatry and there is no consensus in the definitions employed (8,9), we chose to use a single, general term for such manifestations in our study: hallucinatory phenomena.
Little is known about the prevalence of hallucinatory phenomena in the general population, but evidence suggests they are frequent (10). Auditory and visual phenomena are considered a risk factor for psychiatric disorders (11), but do not occur exclusively in psychosis (12).
Of all the hallucinatory phenomena, the auditory phenomena are of the greatest interest to otological practice, as they require differential diagnosis. Among these, auditory verbal hallucinations (AVHs, "hearing voices") are more common than musical ones. Both types of hallucinatory phenomena have been associated with several neurologic changes (such as stroke or brain tumors), psychiatric disorders (such as depression and schizophrenia), and drug use (ketamine, ranitidine, benzodiazepines, alcohol, cannabinoids, etc.), among other factors (13,14). Musical phenomena may be associated with sensory deprivation (15,16,17); the presumed mechanism involves the disinhibition of certain neuronal circuits, which would lead to the recall of memory traces.
In addition to the cerebral changes involved in the etiology of hallucinatory phenomena, other theories correlate the onset of these phenomena and their content with psychic and emotional factors. According to these authors, such manifestations arise when patients (psychotic or otherwise) lack sufficient symbolization resources to cope with certain traumatic situations, such as intense physical distress, sensory deprivation, loss of time-space orientation, or assaults on the patient's ideals (18). Due to the characteristics of their psyche, psychotic patients perceive hallucinatory phenomena as reality (19).
In view of the need for further clarification of certain psychological aspects of patients presenting to otolaryngology services with tinnitus and concomitant auditory hallucinations, the present study sought to assess whether hallucinatory phenomena of an auditory nature:
1. are related to psychosis;
2. are related in content or form to the patient's psyche;
3. are related to aspects of depression, whether associated to tinnitus or otherwise.
METHODThis study and its informed consent form were approved by the Research Project Analysis Committee of the University of São Paulo School of Medicine Clinics Hospital (HC-FMUSP): No. 1046/06.
Selection criteria
In light of the rarity of the study phenomenon, we included all patients seen at the Tinnitus Research Group of HC-FMUSP between February 2007 and February 2008 who had tinnitus with concurrent auditory hallucinations.
We excluded any patient who would have been unable to begin or complete the stages of the study (due to neurologic illness or hearing impairment not addressed by aural rehabilitation).
The final sample population comprised 10 patients, 8 of whom were women; aged 43-85 years (mean age, 65.7 years).
From an organic standpoint, all patients were diagnosed with hearing loss (conductive, sensorineural, or mixed type of a mild to profound degree) during pre-study medical and audiologic evaluations. One patient had mesial temporal lobe epilepsy with seizures.
The 10 cases were analyzed in a 2-stage process:
-The first stage (conducted by a trained assistant researcher) comprised:
- 1-2 semi-structured interviews meant to characterize the hallucinatory phenomenon;
- application of the Hamilton Depression Rating Scale (HAM-D) to assess the intensity of depression symptoms.
-The second stage (conducted by the chief researcher) comprised:
- 2-4 unstructured psychoanalytic interviews, where the patient spoke freely to the analyst, meant to detect the presence or absence of based on assessment of the manner in which the fundamental aspects of the patient's psyche were organized. The second stage was blinded to the first.
Analysis was conducted in accordance with the theoretical foundations of each instrument:
-HAM-D guidelines;
-Content analysis of semi-structured interviews according to the established topics;
-Freudian and Lacanian theory (for psychoanalytic interviews).
Quantitative analysis consisted of counting the number of events.
RESULTS First stage
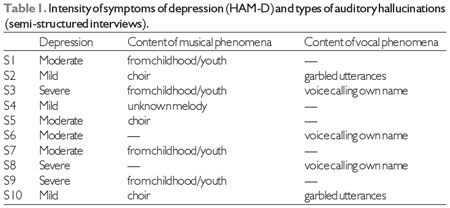
Musical phenomena were more frequent (n = 8) than auditory verbal hallucinations (n = 4), with 2 patients in the sample experiencing both phenomena.
Among the 8 patients reporting musical hallucinations, 4 reported hearing songs from their childhood or youth and 3 reported hearing choirs singing familiar tunes or religious hymns. One patient reported hearing an unfamiliar waltz-like melody.
Of the 4 patients experiencing auditory verbal phenomena, 2 reported having more than one type of AVH. The most common hallucination was the perception-quite clear to some patients-that someone was calling the patient's name (n = 3), particularly during moments of intense solitude and/or fear. Two patients reported hearing sounds that appeared to correspond to the speech of one or more people, but were unable to understand these perceived utterances.
Six patients reported being afraid of the phenomena, with a particular fear of losing their minds; 5 patients reported difficulty concentrating while the hallucinations occurred.
Half of all patients (n = 5) reported improvement in tinnitus-related distress or auditory hallucinations during moments of calm or absentmindedness, but also reported not having explored this possibility in much depth. Regarding the duration of hallucinatory phenomena, 5 patients reported that the phenomena had been present for at least 5 years.
All 10 patients were aware that the tunes or voices they heard were subjective in origin and came from their own minds rather than an external source; however, 6 patients reported being confused at times about the source of the phenomena due to the remarkable clarity of what they heard.
All patients exhibited depressive symptoms to some extent, as measured by the HAM-D (Table 1).
Second stage
By means of psychoanalytic interviews, we determined that none of the 10 patients showed signs of psychosis, not even those who reported auditory verbal hallucinations.
The patients' discourse during psychoanalytic interviews showed that their hallucinatory phenomena (songs or voices) performed some kind of function in the individual psyches of these non-psychotic patients. Generally speaking, the phenomena functioned as a metaphor for aspects of the patient's life that had been lost or intensely threatened, allowing patients to recover these aspects in a way and working as a sort of unconscious protection to help them deal with current difficult life situations. The content of songs or voices heard constituted a privileged means of obtaining this protection, as these 2 examples show:
1. Hannah (name changed to maintain confidentiality), 84, widowed, lives alone. She has suffered from hearing loss for over 15 years. "Everyone has their partners, and no one can be with me", she said resignedly. Mobility issues forced her to stop attending the church to which she had always belonged. Soon afterward, musical phenomena occurred in the form of religious hymns. Hannah made a point of noting that she had been named after a biblical prophetess, citing another prophetess, Deborah, "who, with her singing, gathered her people". Through her hallucinatory phenomena, Hannah unconsciously achieved something similar: soon after being separated from the group to which she had always belonged, she was able to reunite with her people, in a manner of speaking, through the religious songs and hymns she began to hear subjectively.
2. Claire (name changed to maintain confidentiality), 43, experienced musical phenomena in the form of short children's songs that she was sometimes unable to recall. Always a very insecure person, Claire was forced to marry a boorish man who never gave her any support. She found support in her children. After her eldest son began exhibiting strong signs of drug addiction and her brother, who had forced her to marry, died, Claire entered a period of major depression, and soon began to hear, very clearly, people's voices calling her name. Faced with the possibility of losing her main support, her eldest son, and finding herself alone and increasingly insecure, Claire began to hear voices calling out to her.
Psychoanalytic interviews showed that in all cases, patients exhibited a strong tendency toward recalling and dwelling on past distressing situations, maintaining a victimized or suffering posture even when revisiting distant events or those they had already overcome.
Both tinnitus and hallucinatory phenomena were added to this rote repetition of scenarios associated with suffering, thus aiding the maintenance of a condition of suffering, with patients failing to perceive or accept possibilities for positive change, including, in some cases, the treatment strategies proposed by the attending otolaryngologist.
All patients exhibited a generally depressive approach to life. Their depressive symptoms reportedly arose or worsened particularly when they were unable to cope with loss or life changes in a satisfactory manner; aging, changes in social mores and values with the passage of time, and the fear of upsetting or being disregarded by others were stressed as factors.
In 2 patients, vocal phenomena were strongly associated with severe depression; one of the patients improved considerably after treatment with antidepressant medication.
DISCUSSIONIn this sample of tinnitus patients, hallucinatory phenomena (as assessed by semi-structured interviews) were not associated with psychosis. Despite the clarity of auditory phenomena in some cases, all patients remained connected to reality and were aware of the subjective (non-external) nature of their hallucinations; this is consistent with our assessment that psychosis was not involved.
According to the literature, auditory verbal hallucinations (hearing voices) are the most common, particularly in schizophrenia or severe depression (13,23); musical phenomena are far less common, occurring mostly in socially isolated elderly females (14,16,17), and may be associated with hearing loss, neurologic impairment, or psychiatric disorders, especially those in the depression spectrum (14,16,17).
Musical phenomena predominated in our sample, but this actually corroborated the existing literature, as the sample mostly comprised hearing-impaired women in situations of social isolation.
In the study of musical hallucinations, the repetitive and intrusive nature of the perception, coupled with the awareness that this perception is subjective in origin, has led authors to question whether these are truly hallucinatory phenomena or something more akin to obsessive symptoms (24,25,26); in this line of research, such phenomena are considered repetitive mental rituals.
These repetitive mental rituals are present in the strong tendency toward recall, particularly of unpleasant facts and situations, exhibited by all patients in our sample. This influences and intensifies the perceived distress caused by tinnitus and the occurrence of auditory hallucinatory phenomena, and is indicative of a strongly depressive outlook on life. One particularly interesting finding that suggests this was that half of all patients in the sample (n = 5) reported an improvement in tinnitus or auditory hallucinations whenever they were calm or distracted. Nevertheless, they reported making very little use of this possibility as a means of obtaining relief from their symptoms; one may say they strangely preferred to remain in discomfort.
Therefore, we cannot state with certainty that patients became depressed due to the presence of tinnitus and hallucinatory phenomena, but instead may state that patients' depressive outlook on life, with a tendency toward stressing and dwelling on moments of suffering, jeopardizes treatment and decreases the possibility of symptomatic improvement.
Although hearing loss has been reported as a condition that favors the onset of hallucinatory phenomena (15,16,17), the onset of hallucinations in our patients occurred many years after hearing loss and was always tied to traumatic occurrences with which they were unable to cope due to a lack of symbolic resources.
Hallucinatory phenomena thus arose as a sort of unconscious means of psychic protection in the face of helplessness created by a new and distressing situation (18), as shown in the example cases of Hannah and Claire. In addition to being a source of distress and fear, hallucinatory phenomena served as something of a surrogate for something lost and then found again in a curious manner.
This would lead to the activation of memory traces, not by a random release of neuronal circuits (15), but by emotional aspects relevant to each patient. In non-psychotic patients, hallucinatory phenomena are a creation of the mind that arises when symbolization capacity is insufficient to cope with feelings of helplessness; they constitute the remnants of a past reality that act as a protective shield against symbolic emptiness (18).
Viewed from this standpoint, hallucinatory phenomena are somewhat akin to dreams as understood by Freud: they create the possibility of satisfying an unconscious desire, as well as the possibility of some confusion between representation and perception.
Our sample was almost entirely composed of elderly individuals who indirectly mentioned the challenges of aging and the fear of displeasing others or being taken for granted. This reflects the human need for being and feeling heard and regarded by others, which is a key point in the organization of the psyche; it is a lifelong search, and has been since the beginning of time (27,28).
Conversely, the isolation caused by hearing loss and the feeling of being disregarded by others, sometimes due to the experiences of aging, lead to immense psychic distress and diminished motivation, sometimes to the point of losing interest in life, jeopardizing language relations and the patient's perception of the world (29).
Being able to rely on the support of others is a key mediator in overcoming physical or emotional limitations (30). When isolated from everyday social and emotional ties, the elderly tend to find pleasure only in remembering the past (29).
Therefore, we posit that living in an affectively stunted setting, whether due to aging or hearing loss, may lead to intense, subconscious recall of remnants of the past, when living conditions were better, in the form of hallucinatory phenomena. This may support the repetition of these phenomena, as well as patients' difficulty or reticence in pursuing treatment that could reduce their occurrence.
Clinical practice in the Cochlear Implant Group of our service also supports this hypothesis. Some patients with sudden hearing loss and with no evidence of psychosis also report musical and auditory verbal hallucinations, some with reproaching content. In these patients, however, hallucinatory phenomena are more transient and appear to fade as they adapt to deafness.
Although it was not an objective of this study, we found that factors causing emotional distress play a very important role in the treatment of tinnitus patients (9,58). This also holds true for patients with tinnitus and hallucinatory phenomena; depressive aspects are of particular importance.
CONCLUSIONSBased on our findings, we may state that hallucinatory phenomena in tinnitus patients are not directly related to psychosis, but may be strongly associated with patients' emotional experiences, their perception of their current situation, and the manner in which they cope with the challenges of life; particularly important are behaviors brought on by a depressive worldview.
The small sample size of this study obviously limits generalization of our findings. Nevertheless, they do provide interesting research directions, including those for further study of patients experiencing distressing situations in association with deafness.
REFERENCES1. Sanchez TG, Bento RF. An evaluation of tinnitus treatment. Exp Opin Ther Patents, 2000; 10(12):1911-1917.
2. Coelho CB, Sanchez TG, Tyler R. Tinnitus in children and associated risk factors. Prog Brain Res, 2007; 166:179-191.
3. Moller AR. Tinnitus: presence and future. Prog Brain Res, 2007; 166:3-16.
4. Sanchez TG, Medeiros ÍRT, Levy CPD, Ramalho JRO, Bento RF. Tinnitus in normally hearing patients: clinical aspects and repercussions. Rev Bras Otorrinolaringol, 2005; 71(4):427-431.
5. Hébert S, Carrier J. Sleep Complaints in erderly tinnitus patients: a controlled study. Ear Hear, 2007; 28:649-655.
6. Rocha CACB, Sanchez TG. Myofascial trigger points: another way of modulating tinnitus. Prog Brain Res, 2007; 166:209-213.
7. Lloyd SKW, Baguley DM A patient with tinnitus. Clin Otolaryngol, 2008; 33:25-28.
8. Cheniaux E. Psicopatologia descritiva: existe uma linguagem comum? Rev Bras Psiquiatr, 2005; 27(2):157-62.
9. Blom JD, Sommer IEC Auditory Hallucinations Nomenclature and Classification. Cog Behav Neurol, 2010; 23(1).
10. Ohayon MM Prevalence of hallucinations and their pathological associations in the general population. Psychiatry Res, 2000; 97(2-3):153-64.
11. Whalley HC, Gountouna V-E, Hall J, McIntosh A, Whyte M-C, Simonotto E, Job D E, Owens DGC, Johnstone EC, Lawrie SM. Correlations between fMRI activation and individual psychotic symptoms in um-medicated subjects at high genetic risk of schizophrenia. BMC Psychiatry; 2007, 7:61. http://www.biomedcentral.com/1471-244X/7/61.
12. Nasio JD. A alucinação e outros estudos lacanianos. Rio de Janeiro: Jorge Zahar Editor; 1997:52-56.
13. Dalgalarrondo PA. Sensopercepção e suas alterações. Psicopatologia e Semiologia dos Transtornos Mentais. Porto Alegre: Artes Médicas Sul; 2000:81-90.
14. Prommer E Musical Hallucinations and opioids: a word of caution. JPain Symptom Manage, 2005; 30(4):305-307.
15. Hammeke TA, McQuillen MP, Cohen BA Musical hallucinations associated with acquired deafness. J Neurol Neurosurg Psychiatry, 1983; 46:570-2.
16. Gordon AG Musical hallucination - correspondence. Neurology, 1994; 44:986.
17. Griffiths TD Musical hallucinosis in acquired deafness - phenomenology and brain substrate. Brain, 2000; 123(10):2065-76.
18. Alonso SL. Do sintoma simbólico ao mais além: a problemática do alucinatório (on-line) www.estadosgerais.org/encontro/IV/PT/trabalhos/Silvia_Leonor_Alonso.pdf
19. Alvarenga E. Psicoses freudianas e lacanianas. Opção Lacaniana - Revista Brasileira Internacional de Psicanálise, 2000; 28:40-3.
20. Leguil F. Mais-além dos fenômenos. A querela dos diagnósticos. Rio de Janeiro: Jorge Zahar; 1986:60-9.
21. Monseny JÁ. ética psicanalítica do dianóstico. Psicanálise e Psiquiatria: controvérsias e convergências. Quinet A (org.). Rio de Janeiro: Rios Ambiciosos; 2001:69-72.
22. Quinet A. Como se diagnostica hoje? Psicanálise e Psiquiatria: controvérsias e convergências. Quinet A (org.). Rio de Janeiro: Rios Ambiciosos, 2001:73-8.
23. Kot T SerperM Psychological Mechanisms Mediate Psychotic Behavior. J Nerv Ment Dis, 2004; 192(6):428-429.
24. Hugo FJ, Stein DJ, Heerden BV Musical obsessions or hallucinations? (letters - In Reply). J Neuropsychiatry Clin Neurosci, 2000; 12(4):519.
25. Ali J A Musical hallucinations and deafness: a case report and revies of the literature. Neuropsychiatry, Neuropsychol BehavNeurol, 2001; 15(1):66-70.
26. Terao T, Ikemura N Musical obsessions or hallucinations? (letters). J Neuropsychiatry Clin Neurosci, 2000; 12(4):518-9.
27. (Laznik M-C A voz como primeiro objeto da pulsão oral. A voz da sereia - o autismo e os impasses na constituição do sujeito. Wanderley D (org.). Salvador: Ágalma, 2004, 69-87.
28. Ferreira ICH, A voz na constituição do sujeito e na clínica do autismo: o nascimento do Outro e suas vicissitudes. Tese de Doutoramento em Psicologia Clínica. Faculdade de Psicologia e Ciências da Educação da Universidade de Coimbra, 2005.
29. Mannoni M, A velhice hoje. O nomeável e o inominável - a última palavra da vida. Tradução: Dulce Duque Estrada. Rio de Janeiro: Jorge Zahar Ed., 1995:13-38.
30. Taylor MG, Lynch SM, Trajectories of impairment, social support, and depressive simptoms in later life. J Gerontol: Social Sciences, 2004; 9B(4):S238-46.
31. Lee S-H, Kim J-H, Hong S-H, Lee D-S Roles of cognitive characteristics in tinnitus patients. J Korean Med Sci, 2004; 19:864-9.
32. Folmer R L Long-term reductions in tinnitus severity. Ear, Nose Throat Dis, 2002; 2:3.
1) Master of Science. Psychologist of Psychology Division / Otolaryngology of ICHC-FMUSP.
2) MD, PhD. Associate Professor of Otolaryngology Discipline of FMUSP.
3) MD, PhD. Professor and Chairman of Otolaryngology Discipline of FMUSP.
4) PhD. Director of the Psychology Division of the ICHC-FMUSP.
Institution: Clínica Otorrinolaringológica / Divisão de Psicologia do ICHC - FMUSP. São Paulo / SP - Brazil. Mailing address: Rosa Maria Rodrigues dos Santos - Rua Barata Ribeiro, 372 - Apto. 31 - Bela Vista - São Paulo / SP - Brazil - Zip code: 01308-000 - E-mail: rmrodriguess@usp.br
Article received in November 3, 2011. Article approved in January 9, 2012.