INTRODUCTIONThe external ear is formed by the pinna and the external auditory canal (EAC), and has an important role in the processing of acoustic signals from the free field to the tympanic membrane. The transfer function between the free field and the tympanic membrane, or simply, "the external ear resonance," derives from the contribution of different structures, as described in a classic study in 1974 (1).
-Frequencies below 1000 Hz mainly suffer effects from the torso, neck, and head, with a magnitude of up to 5 dB.
-Frequencies between 1000 and 3000 Hz are the predominant contribution of the EAC. The EAC is essentially a tube that has one open end (area of the shell) and another end closed by the tympanic membrane. The EAC behaves as a resonator of the quarter wave type, and the resonance frequency (F) is given by the formula F = v/4L, where "v" is the speed of sound and "L" is the length of the EAC (2). In adults, EAC resonance occurs in the region from 2700 to 3000 Hz, with amplitudes between 10 and 20 dB (3-5).
-Frequencies between 3000 and 7000 Hz are the predominant contribution of the shell (the region between 5000 and 6000 Hz, with a magnitude of approximately 10 dB) and the pinna (the 4000 Hz region, with a magnitude of approximately 3 dB).
The resonance response of the external ear (REUR - real ear unaided response) can be measured objectively. In essence, a probe microphone positioned at a specific point in the EAC, not occluded, measures the absolute sound pressure level, generated against a particular input signal presented in the free field. By subtracting the level of the incoming signal input REUR, it is possible to obtain a natural amplification or gain of the external ear (REUG - real ear unaided gain) (6).
The typical REUG of an adult presents little or no amplification in the frequency region below 1500 Hz. The presence of a primary peak of amplification provided by the resonance of the EAC, approximately 2600-3000 Hz, and a secondary peak between 4000 and 5000 Hz are given by the properties of the shell (3).
The measurement of resonance, or the gain of the external ear, serves as a basis for obtaining the insertion gain (REIG - real ear insertion gain), which expresses the actual amount of amplification provided by hearing aids in the ear canal of the user. The REIG is given by the difference between the response or gain obtained with the prosthesis "on" and positioned inside the ear (REAR - real ear aided response or REAG - real ear aided gain) and the response or resonance gain of the external ear (REUR/REUG). In other words, REIG = REAR - REUR or REIG = REAG - REUG.
The REIG values are compared with the predetermined prescription targets, generated by mathematical formulas to determine whether the requirements for a particular individual's electroacoustic hearing impairment are being contemplated (7). If the user has one atypical REUR or REUG, this factor will be incorporated into the calculation of the REIG, and this is not necessarily desirable. In such cases, it is preferable that verification is based on the measurements of the REAR (8).
Among other interferences, the anatomical and physiological conditions of the outer and middle ear affect the REUR/REUG. With aging occur certain modifications in the external ear, such as loss of elasticity, decreased fat layer, increased fragility of the skin, collapse of the EAC with a reduction in its volume, increased production of cerumen, increased hair growth in the canal, and an increase in the size of the pinna (5,9). In the middle ear, it is possible to observe a reduction in the elasticity of muscle tissue, tympanic membrane retraction, arthritic changes in the joints between the ossicles, atrophy and degeneration of the muscle fibers and ligaments of the ossicles, and the decline of the muscle function that controls the opening of the Eustachian tube (4,9,10). In addition, some changes related to hearing sensitivity among the elderly can be attributed to changes in the mechanical characteristics of the external and middle ear. The acoustic impedance and the equivalent volumes of the external and middle ear can be verified by means of immittance audiometry (11).
Because older adults experience changes in the external and middle ear that affect the REUG, the aim of this study is to investigate the relation between the natural resonance of the ear and the volumes of the external and the middle ear in the elderly.
METHODThis is a retrospective study approved by the Ethics Committee of the Bauru School of Dentistry-University of Sao Paulo (FOB/USP) (protocol 33/2007). The medical records of patients enrolled in the Speech and Audiology Clinic of FOB/USP, treated between February and July of 2009, were analyzed.
The inclusion criteria were as follows: ages between 18 and 59 years (for adults) or more than 60 years old (for the elderly); with sensorineural hearing loss; presenting no changes in the external or middle ear on ENT examination; presenting immittance data; and presenting full details of REUG measurements, accomplished with the Madsen Aurical equipment by audiologists experienced in the procedure.
Data from 51 subjects who met these selection criteria were collected from medical records and segregated into two groups (adult and elderly) (Table 1). The analysis was performed for the ears and included only those who had no changes when compared with the ENT examination (normal otoscopy).
The AZ7 (Interacoustics), SD30 (Siemens), GSI (TympStar), and Zodiac (Madsen) systems were used to measure immittance. In all cases, we used a tone probe of 226 Hz with an intensity of 85 dB SPL. The pressure was varied from positive to negative (+200 to -200 daPa), to obtain the route of the tympanometric curve.
The equivalent volume of the external ear (VeqEE) was obtained by inserting the probe into the EAC with a pressure of +200 daPa. At this pressure, the impedance of the middle ear and the tympanic membrane is extremely high and the acoustic admittance is virtually zero. Thus, the immittance is measured only by the column of air in the EAC, from the tip of the probe/olive and the tympanic membrane, if the latter is in fact intact (12).
The equivalent volume of the middle ear (VeqME) is defined as the value of the acoustic admittance of the side surface of the tympanic membrane, in reference to the pressure of the tympanogram peak (12). The VeqME was obtained by subtracting the volume registered in the VeqEE, at the point of maximum compliance. The pressure value at which the maximum compliance occurred was also recorded when the measurements were performed using the AZ7 (Interacoustics) equipment.
REUG measurements were performed with the Aurical (Madsen) equipment, in an acoustic treatment room. Per the protocol of the audiological clinic, the probe tube was placed in the EAC by using the geometric method, which is based on the length of the ear mold. Thus, the tip of the probe was positioned 3 mm beyond the end of the mold and up to 5 mm from the tympanic membrane, to avoid standing waves and to ensure that all high-frequency components were measured accurately (13).
All measurements were carried out with a speaker positioned at 0 azimuth and approximately at a distance of 50 cm from the individual. The stimulus was speech noise, presented at an intensity of 65 dB SPL. The equalization of the sound field was performed concomitantly, with the reference measurement microphone placed at the ear level of the individual while controlling the output of the speaker, in order to keep the sound pressure level as stable as possible and not influenced by small changes in the position of the head and torso during the measurement procedures.
The equipment automatically performs a subtraction of the absolute SPL in the EAC (REUR) and the input level supplied (in this case, 65 dB SPL), generating the REUG at each frequency. All measurements are stored in the database of the equipment used. For the purpose of this study, measurements were retrieved from the database and only the frequency and amplitude of the primary peak response were analyzed.
Statistical analyses were performed using the PACOTICO v.5.0 software. The Pearson correlation coefficient (r) was calculated between the primary peak frequency and the amplitude of the REUG, with the equivalent volume of the external and middle ear and the age of the participants. Student's t-test for independent samples was used to compare the differences between the tympanometric data and the amplitude and frequency of the primary peak of the REUG between adults and elderly, and between men and women. In all cases tested, we adopted a significance level of 0.01.
RESULTS In 5 elderly and 3 adult patients, it was not possible to recover the data for the VeqEE.

Legend: SD, standard deviation.
Legend: p < 0.01, statistically significant.
Legend: p < 0.01, statistically significant. * Significant result
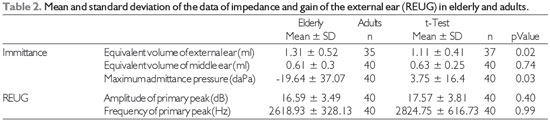
Although the VeqEE of the elderly was 0.2 ml greater than that of adults, there were no statistical differences between the 2 groups (Table 2). Furthermore, the correlation between the VeqEE and patient age was weak and not significant (Table 4). Researchers have found average values of the VeqEE equal to 1.4 ml, and observed no significant changes in this volume with age (14). Another study also found no significant statistical differences in the VeqEE between adults and the elderly (15). One study has found VeqEE values to be 0.2 ml greater in the elderly than in adults. The authors attributed this result to the lower EAC diameter in the elderly (mean 9.25 mm) than that found in the adults tested (mean 10.67 mm) (16).
The mean VeqME obtained in this study (Table 2) is in agreement with the literature data reporting a VeqME of 0.3 to 1.6 ml for adults with normal function of the middle ear (17). Researchers have found that the volumes of the middle ear for adults and seniors were 0.62 and 0.61, respectively (16). No difference was observed in the VeqME between the adults and the elderly, and the correlation between the participants' age was weak and not significant (Table 4). These findings appear to conflict with reports of an age-related increase in the stiffness of the transmission system of the middle ear (9, 10). However, other studies also found no differences in the VeqME when comparing data from adults and the elderly (15, 18, 19).
The mean peak pressure was -19.64 daPa for the elderly and 3.75 daPa for the adults (Table 2), which is in agreement with the literature data reporting a pressure of -100 to + 50 daPa in adults with normal function of the middle ear (11). In surveys in 2004 and 2007, the authors found no age-related changes in peak pressure, when comparing data from adults and seniors (15, 20). They postulated that the degeneration of the anatomical structures of the middle ear or Eustachian tube, resulting from advancing age, did not influence the ventilatory capacity of the middle ear (15, 20).
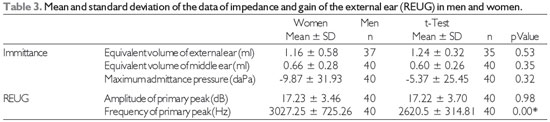
The VeqEE of men was higher than that of women, but this difference was not significant (Table 3). The literature reports significant differences in the VeqEE between men and women in the order of 0.35 ml for adults (21), and 0.3 ml when considering adults and the elderly (16). This effect of gender on the VeqEE can be attributed to the size of the EAC, which tends to be higher in men than in women (21).
No statistically significant differences were found in the VeqEE and the maximum admittance pressure between men and women (Table 3), corroborating with the literature data (16, 20).
The mean frequency and peak amplitude of the primary REUG found for the adult and elderly patients (Table 2) were close to that of a typical adult REUG, i.e., the primary peak between the 2600 and 3000 Hz range of 14 to 18 dB (3). A compilation of studies on the resonance of the external ear indicates an average resonance frequency of 2700 Hz with an amplitude of 16.8 dB (22).
In this study, there was no difference in the frequency and primary peak REUG between the adults and the elderly. Researchers found average peak amplitudes of the primary REUR of 17.3 and 18.2 dB for adults 40-49 and 50-59 years of age, respectively. For the elderly, the values were 18.2 to 19 dB. The authors also observed no age-related differences in the peak REUR (4).
No differences were found in amplitude; however, there was a statistically significant difference found between men and women about the measure of the frequency of the primary peak REUG (Table 3). This result may have occurred owing to the lower VeqEE found in women.
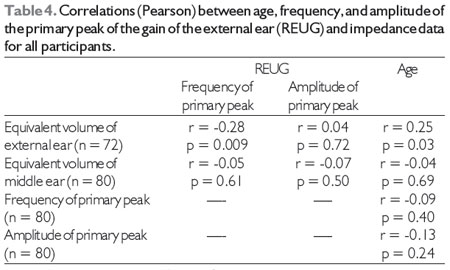
We also observed (Table 4) that there is a negative weak correlation, although significant, between the VeqEE and the primary peak frequency. That is, the higher the VeqEE, the lower the resonance frequency of the EAC. This can be explained by the fact that the EAC behaves as a resonator of a quarter wave dimension (length) of the EAC in order to determine the primary peak resonance (2).
However, there is controversy about the use of tympanometric procedures for estimating the volume of the EAC. On one hand, the volume of the EAC can be evaluated when it is unobstructed and has a volume of up to 1.4 ml. Above this volume, there is a progressive decrease in the accuracy of the procedure (23).
On the other hand, one study reports that acoustic immittance measurements are influenced by the positioning of the probe and the EAC olive: as the probe is inserted deeper, the lesser the volume of the external ear and the greater the pressure generated within the EAC (2). To estimate the volume of the external ear by measuring the acoustic immittance, it is necessary to consider certain factors. For example, a pressure variation of +400 daPa is not enough to reach the maximum impedance of the middle ear; thus, a conclusive result cannot be obtained with only the impedance of the external ear. The use of probes of 220 and 660 Hz in tympanometric procedures overestimates the actual physical volume, with errors of 10% and 24%, respectively, and these differences were attributed to the frequencies of the reactance of the probe system of the middle ear. Because of the retrospective design of this study, it was not possible to control the insertion of the probe and olive in obtaining acoustic immittance measurements, and this is a study limitation.
The absence of differences in the mean values of the REUG in the elderly suggests that targets and measures of insertion gain (REIG) in this population can be used to verify the amplification provided by hearing aids in the EAC. However, some data in this study showed the elderly patients' REUG as being atypical (Figure 1). Thus, in cases where this atypical response is identified, measurement of the REAR is recommended as a verification method (8).
Legend: p < 0.01, statistically significant.
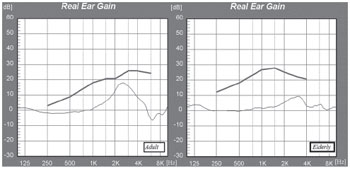
Figure 1. Example of a typical REUG curve in an adult patient (peak at 2500 Hz and gain of 17.9 dB) and an atypical curve in an elderly patient (peak at 3070 Hz and gain of 9.5 dB).
No differences were found between adults and elderly, or between men and women, in terms of equivalent volumes of the external and middle ear as well as frequency and amplitude of REUG primary peak, suggesting that the verification of amplification can be performed using targets and measures of insertion gain (REIG) in this population.
REFERENCES1. Shaw EAG. Transformation of sound pressure from the free field to eardrum in the horizontal plane. J. Acoustical Society of America, 1974; 56:1848-61.
2. Ballachanda BB. Theoretical and applied external ear acoustics. J Am Acad Audiol, 1997; 8(6):411-20.
3. Mueller GH, Hall JW. Audiologist's desk reference volume II: audiologic management, rehabilitation and terminology. San Diego, Singular Publishing, 1998.
4. Liu TC, Chen YS. Aging and external ear resonance. Int J Audiol, 2000; 39(5):235-7.
5. Chasin M. The etiology of the REUG: did we get it completely right? Hear J, 2005; 58(12):22-4.
6. Zenker, F. Medidas en oído real mediante sonda microfónica. Definición y aplicaciones. [online]. Auditio: Revista electrónica de audiología. 15 Septiembre 2001,vol. 1(1), pp. 10-15. http://www.auditio.com/revista/pdf/vol1/1/040101.pdf
7. Mueller HG. Probe Microphone measurements: 20 years of progress. Trends Amplif, 2001; 5:35-68.
8. British Society of Audiology. Guidance on the use of real ear measurement to verify the fitting of digital signal processing hearing aids. Disponível em: http://www.thebsa.org.uk/docs/RecPro/REM.pdf
9. Chisolm TH, Willott JF, Lister JJ. The aging auditory system: anatomic and physiologic changes and implications for rehabilitation. Inter J Audiol, 2003; 42(6):3-10.
10. Howarth A, Shone GR. Ageing and the auditory system. Postgrad Med J. 2006, 82: 166-171. Disponível em: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2563709/.
11. Beck D, Speidel D, Huijnen J, Petrak M. Tympanometry and acoustic reflex: innovation, review, and application. Hear Rev, 2009; 16(4):28-33.
12. Wiley TL, Stoppenbach DT. Basic principles of acoustic immittance measures. In: Katz J, Burkard R, Medwetsky L. Handbook of Clinical Audiology. 5a ed. Philedelphia: Lippincott Williams & Wilkins, 2002: 159-74.
13. Dillon H. Hearing aids. New York: Thieme; 2001.
14. Ahn JH, Park HJ, Park GH, Jeong YS, Kwak HB, Lee YJ, Shin JE, Moon WJ. Tympanometry and ct measurement of middle ear volumes in patients with unilateral chronic otitis media. Clin Exp Otorhinolaryngol. 2008 September, 1(3):139-42.
15. Stenklev NC, Vik O, Laukli E. The aging ear: an otomicroscopic and tympanometric study. Acta Otolaryngol, 2004 Jan; 124(1):69-76.
16. Feeney MP, Sanford CA. Age effects in the human middle ear: wideband acoustical measures. J Acoust Soc Am, 2004; 116:3546-58.
17. McSpaden, JB. Basic tympanometry in the dispensing office. Hear Rev [periódico online]. 2006 [citado 2 dez 2009]. Disponível em: http://www.hearingreview.com/issues/articles/2006-11_04.asp.
18. Uchida Y, Nomura H, Itoh A, Nakashima T, Ando F, Niino N, Shimokata H. The effects of age on hearing and middle ear function. J Epidemiol, 2000; 10:S26-32.
19. Rawool V W, Harrington B T. Middle ear admittance and hearing abnormalities in individuals with osteoarthritis. Audiol Neurotol, 2007; 12:127-36.
20. Golding M, Doyle K, Sindhusake D, Mitchell P, Newall P, Hartley D. Tympanometric and acoustic stapedius reflex measures in older adults: the Blue Mountains Hearing Study. J Am Acad Audiol, 2007 May; 18(5):391-403.
21. Wahab NA, Rashid MF. Tympanometric values in young Malay adults: preliminary data. Singapore Med J, 2009 Nov; 50(11):1077-9.
22. Shaw EAG, Vaillancourt MM. Transformation of sound-pressure level from the free field to the eardrum presented in numerical form. Journal of the Acoustical Society of America, 1985; 78(3):1120-1123.
23. Hussaini AA, Owens D, Tomkinson A. Assessing the accuracy of tympanometric evaluation of external auditory canal volume: a scientific study using an ear canal model. Eur Arch Otorhinolaryngol, 2011 Dec; 268(12):1721-5.
1) Master in Sciencies - School of Dentistry of Bauru - University of São Paulo; Speech Pathologist and Audiologist at Hearing and Communication Institute and at Audicare.
2) PhD in Neuroscience and Behavior - Psychology Institute, USP; Professor in the Department of Speech Pathology and Audiology, School of Dentistry of Bauru, University of Sao Paulo.
3) PhD in Sciences - Communication Disorders, HRAC; Professor in the Department of Speech Pathology and Audiology, School of Dentistry of Bauru, University of Sao Paulo.
Institution: Faculdade de Odontologia de Bauru da Universidade de São Paulo. Bauru / SP - Brazil. Mailing address: Bárbara Guimarães Bastos - Rua Maximiliano Robespierre, 52 - Vila Zezé - Jacareí - São Paulo - SP - Zip code: 12310-700 - E-mail: barbarabastos@gmail.com
Article received in 17 de fevereiro de 2012. Article approved in 22 de maio de 2012.

