INTRODUCTIONProportions, harmony, and symmetry of facial features are considered determinants of the perception of beauty (1,2,3,4). Symmetry refers to the fact that one side is similar to the other.
Evolutionary biologists predict that facial symmetry should be attractive, since it represents a sign of health and genetic quality (5,6). Symmetry must, therefore, be regarded as a major factor of facial attractiveness (4).
Anthropometry is the science that studies the measures, weights, and proportions of the human body, providing objective data to assess morphology (7).
Craniofacial anthropometry started when anthropologists measured human skulls in order to categorize and classify them by race. It was discovered then that the nasal index was the best index in order to distinguish the various human races (8) .
The clinical application of craniofacial measures was initially focused on cases of congenital and disfiguring facial trauma. In situations in which the surgeon needed to know standard measures, anthropometric studies served as an excellent base (9) .
Currently, these findings have great significance in rhinoplasty, as this surgery aims to improve facial aesthetics by changing the dimensions and proportions of the central element of the face: the nose (1). These dimensions and proportions, which can be corrected by rhinoplasty, have a very important role in the general perception of the face as symmetrical or asymmetrical (10,12,13). The presence of asymmetries should be recognized preoperatively in all views of the nose (13).
Furthermore, detection and discussion of the presence of pre-existing facial asymmetry, both in patient education and in surgical planning are extremely important in the preoperative evaluation of a rhinoplasty, since they can reduce the impact of the changes in the form the nose after surgery (1).
The concept of beauty and facial proportions suffers considered normal variation with time and different cultures, so the notion of a universal aesthetic standard is not correct and should be tailored to each ethnic group. With the increasing demand for aesthetic nasal surgery, it is essential that the surgeons know the standards of the population with whom they are dealing, in order to maintain the characteristics of that population (3).
To better define norms and standards of facial aesthetics, population studies are needed. There are insufficient studies of nasal and facial measurements of the Brazilian population, especially regarding the presence of facial asymmetry, as well as objective measures for their identification.
To evaluate the presence of facial asymmetry by anthropometric measurements in conjunction with a subjective evaluation, of patients in preoperative rhinoplasty and volunteers without complaint, to verify whether patients with nasal complaints (aesthetic or functional) have greater facial asymmetry than those without it.
METHODThis study was approved by the Ethics Committee on Human Research of UFPR (CAAE: 0197.0.208.000-11, registered at CEP: 2595.202/2011-08).
A prospective cohort study was performed by a protocol and photographs of volunteers recruited from among students of medicine, Federal University of Parana and professionals engaged in health care at the hospital and pre-operative rhinoplasty patients of both sexes and aged between 18 and 55 years. The sample amounted to n = 201.
Exclusion criteria were age less than 18 years and more than 55 years, previous history of trauma, history of nasal or facial surgery, presence of craniofacial anomalies, and persons of black, Asian or mixed race (non-Caucasian noses) to minimize ethnic variations.
All photographs were taken by the same researcher, with the same camera and same standardization. Camera Model Sony Cyber-shot DSC-W125 7.2 Megapixels in size with zoom fixed at 6.0, at a distance of 1.5 m between the machine and volunteer, to account for uniformity of scale and measures. The incidence was anterior-posterior position in Frankfurt.
The photographs were subjected to analysis of facial action parameters by using the program Adobe Photoshop CS3, as in Figure 1. Anthropometric measurements were obtained based on facial soft tissue landmarks, starting with an imaginary sagittal line originating at the midpoint of the hair line, crossing the midpoint of the nasal bridge, the central point of cupid's bow, upper lip, and the lowest point of the chin toward the medial canthus (MC), lateral canthus (LC), lateral alar margin (LAM), oral commissure (OC), and tragus (Tr), as shown in Figure 1.
Measurements were taken in pixels, and included the ratio of the measurement of one side divided by the measurements of the other side. The ratios are as follows: RLMTr = midline-tragus ratio; RLMCL = midline-lateral corner ratio; RLMCM = midline-medial canthus ratio; RLMMAL = midline-lateral alar margin ratio; RLMCO = midline-oral commissure ratio.
We calculated the percentage of asymmetry using the following formula: (Ratio - 1) x 100, and degrees of asymmetry were defined: >2.5%, >5%, and >10% for RLMMAL.
The photographs of rhinoplasty patients and volunteers were evaluated by 3 evaluators (researchers) related to Plastic Facial Surgery in order to analyze the subjective presence of facial asymmetry. The face was considered asymmetric if all the 3 researchers considered thus.
Data were statistically analyzed using the Z test and Odds ratio for calculation of risk (chance or probability of results happening in each group), considering p < 0.05 significant.
RESULTSWe evaluated 101 volunteers and 100 patients in preoperative rhinoplasty (n = 201), 64% women and 36% men.
The results are given in Tables 1 and 2 and Figures 1 and 2.
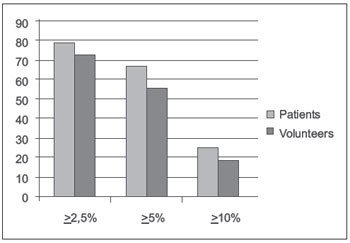
Chart 1. Degree of asymmetry in relation to RLMLAM: for >2.5%, OR = 1.44 (CI 1.35 to 1.53); for >5%, OR = 2.08 (CI 1.884 to 2.276); and >10%, OR = 1.43 (CI 1.332 to 1.528).
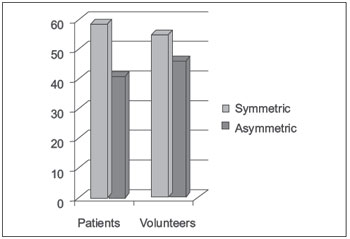
Chart 2. Subjective evaluation of facial asymmetry: patients (n = 100) x volunteers (101). OR = 1.2 (CI 1.15 to 1.25).
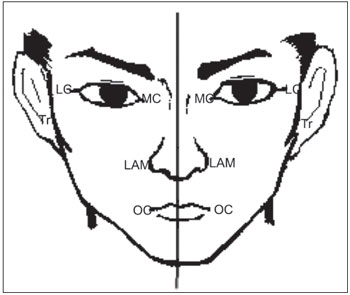
Figure 1. Representation of the landmarks of the facial anthropometric measurements.
The ability to alter the outcomes in facial surgery requires a deep understanding of the evaluation of facial aesthetics, proportion, and symmetry by the surgeon.
Many direct surgical procedures correct facial symmetry or balance, including rhinoplasty.
Symmetry means more than one face side should be identical to the other, it is the overall balance of structures of the face, with all the parts working in harmony and addresses to the fact that the face or opinion of it is unbalanced.
In a face symmetrical and balanced, and therefore pleasant, the vision should flow imperceptibly and continuously between the different subunits, nasal and facial (14) .
The main goal of surgery is to achieve an aesthetic nasal anatomy, which allows a harmonious relationship where no facial feature steals the attention of others and each structure enhances the beauty of the whole.
Rhinoplasty can change the angle of the nose with the face, the length, the width of the nostrils; changes in shape, size, and width change both the intrinsic proportions of the nose and its relations with the other elements of the face (10).
All parts of the face have a role in creating facial symmetry, but some parts contribute more than others. The nose and chin are the major determinants of facial symmetry, mainly because they are at the center of the face and protrude from the face.
The nose is the center of the face, and therefore the focal point of the face. The shape and size of the nose can vary greatly from person to person and can significantly affect facial symmetry (1, 3, 10, 11).
In a study by Nouraei et al., measurements in preoperative and postoperative patients undergoing rhinoplasty showed improved symmetry in the nose postoperatively. This also corresponds to perceptual analyses of the face, as a whole, which became more symmetrical (12). This demonstrates the role that the nose has in the perception of facial symmetry.
The nose itself may still not be symmetrical, due to congenital defects or acquired, which can change the shape of the nose and also facial symmetry.
Correction of nasal asymmetry should be the goal of any surgical procedure that aims to change the nasal contour (13).
Hafezi et al. (15), studying photographs of rhinoplasty patients, found a high rate of facial asymmetry and rhinoscoliosis (crooked or deviated nose). They noted a slight contraction in appearance from the concave side of the nasal deviation, concluding that there is a strong relationship between growth retardation and rhinoscoliosis, causing facial asymmetry.
The finding of similar asymmetrical faces among family members supported the notion that genetics determines facial deformities such as asymmetry by controlling the growth of the face and nose, going against the theory that the deformities are acquired by trauma or developmental disorders (15).
Moreover, Kim et al. (16), analyzing the mechanisms of association between septal deviation and deviation and asymmetry in other parts of the facial skeleton, through evaluation of external and internal parameters of the face (computed tomography), concluded that differences in the growth of bones around the nose may be associated with septal deviation in patients who have suffered nasal trauma. That is, they believe that the septal deviation occurs as a result of asymmetric growth of the jawbones.
Patients with a desire to seek rhinoplasty usually present to the rhinologist with aesthetic and/or functional complaints. The functional complaints may include septal deviation causing nasal obstruction.
In this study, we have been evaluating and documenting the presence of facial asymmetry in patients desiring rhinoplasty by anthropometric measurements and correlated with perception of facial symmetry or asymmetry, assessing whether there is a higher prevalence of facial asymmetry in patients planning rhinoplasty compared with controls.
Anthropometric measurements of the nose provided objective data about the shape and size of the nose (8).
Since the nose is one of the most important components of facial aesthetics, the study of its form and attributes is of great importance not only in rhinoplasty, but also in other areas such as facial reconstruction and forensics (2).
The use of absolute values of the facial measurements can be misleading. Therefore, the evaluation of facial proportions is recommended (17). In our study, we analyzed the ratio between the measurements of each side of the face, i.e., dividing the absolute measure on one side by the other. In order to avoid errors in some patients who are more asymmetric on the left side and others the right, the ratios were always calculated by dividing the side showing more asymmetry by the side showing the lower asymmetry. The was therefore considered totally symmetrical if the ratio was equal to 1.
As in a similar study carried out by Chatrath et al. (1), none of the patients had a perfectly symmetrical nose or face. However, this does not mean that the nose or face is imperfect. However, the surgeon and patient must always be aware of these differences.
Freng et al. (18) compared the facial growth of patients with and without septal deviation, and found significant problems with growth in areas surrounding the nose. The deformities resulting from these growth problems usually do not attract the attention of surgeons and rhinologists (orbits dystopian, raised lip corners, asymmetric zygomatic arches, nasal wings asymmetric and poorly positioned, growth of non-parallel sides of the nose).
In our study, with regard to the mean of the measures, we found a statistical significance only insofar as the ratio of the midline to tragus (RLMTr = 0.9127 x 0.95) (Table 1).
In the objective evaluation, by ratios of the measures, we found a large percentage of individuals with asymmetry measures. In all measurements, more than 89% of patients were found with asymmetrical measurements. Except for the measurement of RLMTr and RLMCM, all others presented a larger percentage of asymmetry in patients than in healthy volunteers, and RLMMAL showed the greatest OR (3.95) (Table 4). Chatrath et al. (1) in their study found more than 90% asymmetry in facial measurements of ratios.
We also found high levels of asymmetry of the RLMMAL (See chart 1), and 25 patients (25%) and 19 volunteers (18%) had levels of up to >10% asymmetry from one side to another. Lesser degrees of asymmetry (>2.5%) were found in up to 79% of patients and 72% of volunteers. Reitzen et al. (13) assessed the same ratios and found similar results for patients with bulbous tips. Given a degree of asymmetry of >5%, there was a higher OR, 2.08 (CI = 1.884 to 2.276).
These measurements show asymmetries in other parts of the face (orbits and lips), which reflect possible changes in facial growth changes due to nasal or facial asymmetric growth leading to nasal affections. Because the nose is located on the jaw, the changes in the symmetry of the jaw elements reflect changes in nasal axis, and vice versa, and consequently in its symmetry (11,15).
There are also studies correlating the convexity of nasal septum deformities accompanying adjacent facial structures (16). As we did not evaluate the presence or absence of septal deviation or other intranasal changes, we cannot conclude with certainty, but this should be studied in future research.
In the subjective evaluation of the presence of facial asymmetry, in the rhinoplasty group, 59 patients of 100 patients were considered asymmetrical (59%), compared to 55 volunteers (54%) (Chart 2), obtaining an OR of 1.2 (CI 1.15 to 1.25), i.e., the group of patients had a 20% increase in asymmetry relative to the group of volunteers. In their study, Chatrath et al. (1) found subjective perception of facial asymmetry of less than 40% in patients with preoperative rhinoplasty.
However, subjective assessment by the researchers is not able to find all the asymmetries found through objective measures.
Several authors (1,11,15,16) have studied the presence of facial asymmetry in rhinoplasty patients, but there was no comparison with controls (patients without indication or desire for rhinoplasty). There is a high incidence of asymmetry in the general population, even in those without facial aesthetic complaints, and we believe this is of great importance to our studies.
Chatrath et al. observed that individual objective measures were poor determinants of subjective perception of facial asymmetry, and were unable to determine a level of asymmetry in the measurements (1). Therefore, together with the anthropometric measurements there should be a subjective evaluation, by common sense and aesthetic knowledge of the surgeon.
Also in their study, it was considered that the measure that best correlated with the subjective presence of facial asymmetry was RLMMAL.
Several studies cited by Zaidel et al. (6) indicate that in humans, unlike in other species, symmetry and attractiveness are not confused.
However, assessment of the presence of asymmetries in the nose and face is not intended to achieve a perfectly symmetrical face or nose.
The evaluation of the asymmetry of the face as a whole is intended to help surgeons to better plan the surgery and inform patients about the limitations of the surgical procedure, which results in greater satisfaction with the results (15).
Reitzen et al. (13) evaluated the presence of asymmetries between the nostrils in patients with bulbous tips, and believes that the discrepancies found in the measures become more apparent after surgical tip refinement, leading to unexpected cosmetic imperfections and lack of patient satisfaction. Therefore, measuring the asymmetry in this case the nose and nares of the base is also important.
The use of anthropometric measurements and calculation of these ratios, together with the judgment of the surgeon, may be useful in the evaluation of facial asymmetry in patients with preoperative rhinoplasty in order to assess the presence of nasal and facial asymmetries.
In the final evaluation, which measures more than aesthetic standards, what should prevail is the desire of the patient in harmony with the aesthetic surgeon (8). Therefore, we suggest the use of anthropometric measurements in conjunction with the subjective evaluation of the surgeon.

RLMTr = midline-tragus ratio; RLMCL = midline-lateral canthus ratio; RLMCM = midline-medial canthus ratio; RLMMAL = midline-lateral alar margin ratio; RLMCO = midline-oral commissure ratio.
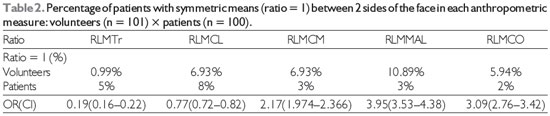
OR = Odds ratio, CI = confidence interval.
Anthropometric evaluation of facial asymmetry in patients with preoperative rhinoplasty at the Hospital de Clinicas da Universidade Federal do Paraná found high prevalence of asymmetry among both pre-rhinoplasty patients and volunteer subjects. Although average measures of RLMTr were the only statistically significant and higher values in the group of patients than in the volunteers, we found a higher prevalence of asymmetry in the patients for the RLMCL (93.07%), RLMMAL (97%), and RLMCO (98%), and higher RLMTr (99.01%) and RLMCM (93.07%) in volunteers.
In the subjective evaluation, a greater percentage of patients (59%) considered themselves asymmetric than volunteers (54%), and in the objective evaluation of the measures, for all measurements the great majority of patients had asymmetry (>89%), and in 25% of patients and 18% of volunteers, we found a degree of >10% asymmetry between sides.
The evaluation of the patient's face as a whole before rhinoplasty is important, both for surgical planning and guidance of the patient. Anthropometric measurements can assist in this evaluation because they are able to detect and validate the presence of asymmetry with greater detail than the subjective assessment of the researcher.
REFERENCES1. Chatrath P, De Cordova J, Nouranei R, Ahmed J, Saleh HA. Objective Assessment of Facial Asymmetry in Rhinoplasty patients. Arch Facial Plast Surg. 2007,9:184-187.
2. Pazos JAT, Galdanes ICS, Lopez MC, Matamala DAZ. Sexual dismorphism in the nose morphotype in adult chilean.Int. J. Morphol., 26(3):537-542, 2008.
3. Patil SB, Kale SM, Jaiswal S, Khare N, Math M. The Average indian Female Nose. Aesthetic Plast Surg 2011 May 5
4. Meyer-Marcotty P, Stellzig-Eisenhauer A, Bareis U, Hartman J, Kochel J. Three-dimensional perception of facial asymmetry. The European Journal of Orthodontics Advance Access. February, 2011.
5. Rhodes G, Proffitt F, Grady JM, Sumich A. Facial symmetry and the perception of beauty. Psychonomic Bulletin & Review 1998, 5 (4), 659-669.
6. Zaidel DW, Cohen JA. The face, beauty, and symmetry: perceiveing asymmetry in beautiful faces. Intern. J. Neuroscience, 115:1165-1173, 2005.
7. Farkas LG. Examination. In: Farkas LG, editor. Anthopometry of the head and face. 2nd Ed. New York: Raven Press; 1994. p. 3-56.
8. Doddi NM, Eccles R. The role of anthropometric measurements in nasal surgery and research: a systematic review. Clinical Otolaryngology 2010,35:277-283.
9. Farkas LG, Katic MJ, Forrest CR. International anthropometric study of facial morphology in various ethnic groups/races. The Journal of craniofacial surgery. V. 16, n. 4 July 2005.
10. American Society of Plastic Surgeons (2007). Nose Surgery (Rhinoplasty). http://www.plasticsurgery.org/patients_consumers/procedures/Rhinoplasty.cfm
11. Yao F, Lawson W, Westreich RW. Effect of Midfacial Asymetry on Nasal Axis Deviation. Arch Facial Plast Surg. 2009;11(3):157-164.
12. Nouraei SAR, Pulido MA, Salch HA. Impact of Rhinoplasty on Objective Measurement and Psychophysical Appreciation of Facial Symmetry. Arch Facial Plast Surg. 2009;11(3):198-202.
13. Reitzen SD, Morris LGT, Davis RE. Prevalence of Occult Nostril Asymmetry in the Oversized Nasal Tip. A Quantitative Photographic Analysis.Arch Facial Plast Surg. 2011;13(5):311-315.
14. ESPINOSA REYES JA, PALACIO M. Plástica Colômbia. La Punta Nasal. http://www.plasticacolombia.com/articulos/anatomia_punta_nasal.php
15. HAFEZI F, NAGHIBZADEH B, NOUHI A, YAVARI P. Asymmetric facial Growth and Deviated Nose. Ann Plast Surg 2010;64:47-51.
16. KIM YM, RHA KS, WEISSMAN JD, HWANG PH, MOST SP.Correlation of Asymmetric Facial Growth with Deviated Nasal Septum. Laryngoscope, 121:1444-1148, 2011.
17. NAINI FB, MOSS JP, GILL DS. The enigma of facial beauty: Esthetics, proportions, deformity, and controvery. American Journal of Orthodontics and Dentofacial Orthopedics, September 2006, 277-281.
18. FRENG A, KVAM E, KRAMER J. Facial skeletal dimensions in patients with nasal septal deviation. Scand J Plast Reconstr Surg Hand Surg. 1988;22:77-81.
1) Medical Doctor. ENT Resident at HC/UFPR.
2) ENT (ABORL) . ENT Doctor.
3) Medical student at UFPR.
4) ENT (ABORL) . Teacher in the Rhinology department of HC/UFPR.
5) MD Education, Clinical Psychology and Physical Education. Coordinator of Medical Scientific Research at HC/UFPR.
6) PhD in ENT (Escola Paulista de Medicina, Brazil. Professor and Head of Department, at UFPR, Brazil.
Institution: Hospital de Clinicas da UFPR. Curitiba / PR - Brazil. Mail address: Bettina Carvalho - Rua General Carneiro, 181 - Center - Curitiba / PR - Brazil - Zip code: 80060-900 - Telephone: (+55 41) 3264-9976 - E-mail: bettinacarvalho@yahoo.com.br
Article received in March 5, 2012. Article approved in July 22, 2012.

