INTRODUCTIONExcessive exposure to high-intensity noise may be harmful to hearing and lead to noise-induced hearing loss (NIHL), which is cumulative, progressive, and irreversible (1). Noise is a physical phenomenon that is an acoustic mixture of sounds at frequencies that do not follow any precise rule. It is classified into 3 types: continuous, with variations of 3-5 dB(A) over a long period; intermittent, with variations larger or smaller than 3-5 dB(A); and impulse, with peaks lasting less than 1s (2).
Auditory dysfunction is a frequent complaint of workers exposed to occupational noise, and NIHL and disorders such as tinnitus can lead to suffering and have a negative effect on the quality of life of these workers (3).
According to the Regulatory Norm 15 (RN-15), the maximum level of noise exposure over an 8-h working day is 85 dB(A); for higher noise levels, the duration of exposure should be reduced (4). For intermittent or continuous noise, there is a serious and eminent risk associated with unprotected exposure to 115 dB(A); and for impulse noise, there is risk associated with exposures equal to or greater than 140 dB(Linear) or 130 dB(C) (Fast) (2).
The Jorge Duprat Figueiredo Foundation of Occupational Health and Safety (FUNDACENTRO) recommends that the threshold level of integration is 85 dB(A); it also uses dose increases of 3 dB, unlike the RN-15, where doses are increased in 5-dB increments (4,5). In other words, to FUNDACENTRO the increase of 3 dB reduces by half the time of exposure to noise and to RN-15 the increase of 5 dB reduces by half the exposure time.
According to Regulatory Norm 7 (RN-7), which outlines parameters for monitoring occupational exposure to noise, tone audiometry in air tests must be performed at 0.5, 1, 2, 3, 4, 6, and 8 kHz. NIHL is suggested for individuals whose audiograms at the 3, 4, or 6 kHz frequencies have threshold values above 25 dB(HL) in one or both ears when both air and bone conduction are measured (6).
The most appropriate method for measuring occupational noise exposure is to use a dosimeter, which can be adjusted in accordance with the laws relevant to each worker and evaluates an individual's daily dose of noise exposure throughout a working day (7). In the USA, dosimetry is the most common method of measuring ambient noise (8).
Aside from conventional pure tone audiometry tests, tests of distortion product otoacoustic emissions (DPOAE), which evaluate high frequencies, can be used to evaluate effects on the auditory system. These tests can be used for early diagnosis of NIHL because individuals who have audiometry test findings within acceptable limits may have abnormal DPEOA test results (9,10).
The aim of this study was to verify studies in the literature that show that environmental noise affects the hearing ability of firefighters, and to analyze the methodology used in these studies.
METHODThe PubMed and Scielo databases were searched and English or Portuguese studies from 2002 to 2012 that included the keywords firefighters, noise, and hearing loss were identified. Initially 24 studies were selected, but only 10 met the inclusion criteria of investigating firefighters' exposure to occupational noise.
LITERATURE REVIEWA study in South Korea evaluated the hearing of 81 factory workers and 371 firefighters over 4 years using both audiological tests and questionnaires that covered smoking history, alcohol use, and service time. The noise levels in the workplaces of the firefighters were described as being between 76-79 dB(A), and increases in hearing loss among the firefighters were found to be proportional to exposure time and were particularly associated with high frequency noise. The authors concluded that 85 dB may not be sufficiently conservative for a working day of 8 h, 5 days per week, because it does not allow for adequate recovery of the cochlear cells after each exposure period (11).
In an internet-based study relating to health promotion and the prevention of hearing loss, 404 firefighters from 35 corporations across multiple states in the USA responded to a questionnaire about the use of hearing protection devices. The researchers found that 41% of the firefighters used hearing protection devices for less than 50% of the necessary time and 30% reported that they never used such devices (12).
To evaluate short-term changes in the hearing ability of firefighters, 118 firefighters underwent audiometry tests: hearing loss was identified in 8% of the right ears and in 13% of the left ears of drivers of large vehicles (13).
In an analysis of high-frequency hearing thresholds in firefighters and military police in Brazil, researchers noted that professionals aged between 40 and 49 had higher thresholds for the 14- and 16-kHz frequencies than a control group (14).
In another study conducted in Croatia, levels of environmental noise were measured and 34 firefighters underwent audiometry tests. Hearing thresholds were found to be changed in the 4- and 8-kHz frequencies. The excessive noise was mainly located in the fire fighting truck, when sirens were sounded, and in the water pump (15).
To identify common sources of noise, other researchers measured environmental noise and described the attitudes and beliefs of firefighters regarding the importance of the use of hearing protectors. Fire fighting trucks and emergency driving, water pumps, chainsaws, and communications equipment were identified as noise sources. Most firefighters believed that compared to other occupations, their risk of hearing loss was small, and they did not use hearing protectors because they believed that the protectors interfered with communication (16).
In one study that aimed to determine whether firefighters are considered a population at risk for NIHL, 12.609 examinations were performed over a period of 11 years. Hearing threshold levels of firefighters were compared with an age-matched control group that was not exposed to noise. A regression analysis was performed to determine the incidence of presbycusis in the absence of noise. The study found that the hearing ability of firefighters was decreased less than expected in the absence of exogenous factors, and therefore dismissed the possibility of firefighters being a population at risk for NIHL (17). However, in an editorial note, potential conflicts of interest relating to the study were reported and the results obtained were questioned (18).
In another cross-sectional epidemiological study of 72 firefighters, a 57-item questionnaire collating personal data, auditory and non-auditory complaints, and annoyance was administered. Fifty-eight firefighters reported experiencing daily noise in the workplace, 73.9% reported car-related noise, 68.0% reported telephone noise, and 38.2% reported administrative noise. In addition, sound mapping of the 8th Grouping Fire Station and neighboring regions from the city of Santo André (SP) was performed and average noise levels of 76-82 dB(A) were found in the station and 67-73 dB(A) in the near vicinity. Thus, urban noise is representative of firefighters' occupational noise exposure. The questionnaires also identified a high incidence of complaints and adverse health effects related to noise exposure (19).
In another study of firefighters in the USA, the Omaha System was applied (a research protocol that uses standardized documentation of customer service from the beginning to end of treatment). The study involved 346 firefighters who initially passed a screening test to identify NIHL and who then underwent an intervention in which hearing protectors were used. Occupational health registers of the Omaha System were used to classify the behavior of firefighters in relation to NIHL and identify those that were considered adequate and appropriate. The study found that changing habits can positively affect health (20).
In a literature review of health problems experienced by firefighters, hearing loss, hip osteoarthritis, and sarcoidosis were identified as being more common. Hearing loss was found in an additional 5 studies and other diseases were identified in 2 studies (21).
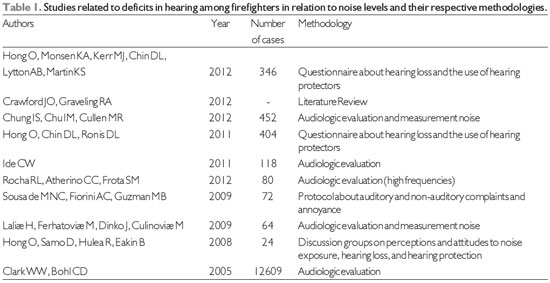
Table 1 shows the studies used in this review. Chars 1 and 2 present the methodologies used and the results obtained.
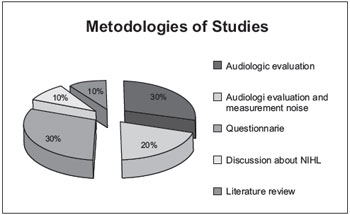
Graph 1. Methodologies used in studies performed over the last 10 years.
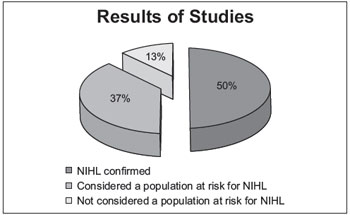
Graph 2. Results of studies.
Of the 10 studies selected for this review, 2 (20%) included quantifications of environmental noise and its association with audiological test results (11,15), 3 (30%) only included audiological tests (audiometry)(13,14,17), 3 (30%) administered questionnaires (12, 19), and 1 (10%) involved a group discussion of NIHL (16) and 1 (10%) literature review. Thus, there were few studies of the association between audiological tests and noise quantifications.
Furthermore, all but one (17) of the studies cited (1-16, 19-21) found that high sound pressure levels damage the auditory system, and the veracity of the exceptional study was questioned (18). These findings indicate that there is a necessity for preventive measures to be adopted by this population since it is considered to be at risk.
The importance of DPOAE for the evaluation of cochlear damage among workers exposed to high-intensity noise is well established. However, none of the studies reviewed used this method of evaluation together with audiometry tests despite it being relevant to the diagnosis of NIHL (9,10). The importance of new studies that adequately quantify noise exposure in the different work environments of firefighters that include subjective as well as objective tests of hearing such as DPOAE evaluations (which can aid early diagnosis of cochlear lesions) as well as normal audiometry evaluations should thus be clear. High-frequency hearing tests are becoming an important complementary method of monitoring the hearing of workers exposed to noise.
The laws in Brazil, both the RN-15 and the Occupational Hygiene Norm (OHN-01) of Fundacentro, are concerned with the time versus the intensity of occupational exposure to noise (4, 5), and therefore there is a need for studies that evaluate the noise exposure of firefighters since NIHL can affect their quality of life.
Hearing conservation programs in this population are important to both prevent NIHL and reduce its impact because when exposure to high sound pressure levels occur, damage to the auditory system is halted. Another important point is that awareness of the damage that noise can cause should be increased because many firefighters believe that the risk to their health is relatively small (16), and a lack of awareness of NIHL can lead to other problems including workplace accidents due to hearing loss. Thus, it is necessary that firefighters are made aware of the importance of the use of hearing protectors and that they rest for periods sufficient for the regeneration of cochlear cells.
CONCLUSIONMost of the reviewed studies reported that firefighters are a population at risk of hearing impairment, and therefore it is necessary that preventive measures be implemented to reduce the incidence of occupational hearing loss. In recent years, few studies of firefighters have been conducted and even fewer have included environmental noise measurements as well as audiological tests. In addition, all of the studies conducted audiological tests that involved the subjective assessments of hearing, which are incomplete and thus not sufficient for an accurate diagnosis of hearing ability among workers.
In summary, these results show the importance of new research to adequately quantify the noise exposure of firefighters in different work environments in order to identify possible adverse conditions as well as aid in the diagnosis of hearing loss.
REFERENCES1. Araujo SA. Noise induced loss in metallurgical workers. Otorrinolaringol. 2002; 68:47-52,
2. Massera C. The study of noise - Thenoise in the environment. Avaliable in: http://www.scribd.com/doc/6929151/estudo-do-rudo. Avaliable in: 10 mai 2012.
3. Ogido R, Costa da EA,Machado HC. Prevalence of auditory and vestibular symptoms among workers exposed to occupational noise. Rev. Saúde Públ. 2009, 43:377-80.
4. Brazil. Ordinance 3.214 june 8,1978, approves the NR do Charpter V. Títle II, of the CLT, relating to Safety and Occupational Medicine. NR-15, Annexs I e II. Jun. 8, 1978.
5. Fundacentro. Evaluation of occupational exposure to noise. Standard Occupational Hygiene NHO 01, São Paulo, 2001.
6. Brazil. Ordinance nº 24 December 29,1994. New compositionof NR - 7. Program medical control of occupational health. Official Journal of the Union, Dec. 20, 1994.
7. Creppe RC, Porto LGC. Usinga dosimeterin the evaluations of occupational noise. Avaliable in: http://www.segurancaetrabalho.com.br Avaliable in: 7 jul. 2012.
8. Hager LD. Sound exposure profiling: a noise monitoring alternative. Am Ind Hyg Assoc J. 1988;59:414-8.
9. Marques FP, Costa EA. Exposure to occupational noise: otoacoustic emissions test alterations. Rev Bras Otorrinolaringol. 2006;72:362-6.
10. Duarte AS. Emissões Otoacústicas. Fernandes FDM, Mendes BCA, Navas ALPGP. Tratado de Fonoaudiologia. 2nd ed. São Paulo: Roca, 2010. Vol.1, pp. 78-84.
11. Chung IS, Chu IM, Cullen MR. Hearing effects from intermittent and continuous noise exposure in a study of Korean factory workers and firefighters.BMC Public. Health. 2012;12:80-7.
12. Hong O, Chin DL, Ronis DL. Predictors of Hearing Protection Behavior Among Firefighters in the United States. Int J Behav Med. 2011.
13. Ide CW. Hearing losses in wholetime firefighters occurring early in their careers.Ocup. Med. 2011;61:509-11.
14. Rocha RL, Atherino CC, Frota SM. High-frequency audiometry in normal hearing military firemen exposed to noise. Braz J Othinolaryngol. 2010;76:687-94.
15. Lalic H, Ferhaovic H, Dinko J, Culinovic M. Hearing damage as a consequence of firefighters' professional exposure to noise. Acta Med. Croatica. 2009;63:195-9.
16. Hong O, Samo D, Hulea R, Eakin B. Perception and attitudes of firefighters on noise exposure and hearing loss. J Occup Environ Hyg. 2008;5:210-5.
17. Clark WW, Bohl CD. Hearing levels of firefighters: risk of occupational noise-induce hearing loss assessed by crosssectional and longitudinal data. Ear Hear. 2005;26:327-40.
18. Ryals BM, Svirsky MA. Editorial note: Regarding sufficiency of author´s disclosures: Hearig levels of firefighters: risk of occupational noise-induced hearing loss assessed by crosssectional and longitudinal data. Ear Hear. 2008;29:815-6.
19. Sousa de MNC, Fiorini AC, Guzman BM. Annoyance caused by noise to a population of firefighters. Rev Soc Bras Fonoaudiol. 2009;14:508-14.
20. Hong O, Monsen KA, Kerr MJ, Chin DL, Lytton AB, Martin KS. Firefighter hearing health: An informatics approach to screening, measurement, and research. Int. J. Audiol. 2012;51:765-70.
21. Crawford JO, Graveling RA. Non-cancer occupational health risks in firefighters. Occup Med (Lond). 2012;62:485-95.
1) Speech Therapist. Masters Student in Human Communication Disorders at the State University of São Paulo -UNESP- Marília/SP - Brazil.
2) Phd in Biological Sciences- UNESP Campus of the State University of São Paulo -UNESP- Botucatu/SP- Brazil. Professor at the Speech Therapy Department of the Faculty of Philosophy and Science at the State University of São Paulo - UNESP-Marília/SP - Brazil.
CRFª-2nd Region
Instituition: State University of São Paulo. Marília/SP - Brazil. Mailing address: Carla Linhares Taxini - 2432 Campos Salles Avenue - Vila Guarani - Matão / SP - Brazil - Zip Code: 15997-066 - E-mail: carlataxini@gmail.com
Support: Fapesp (process nº 2011/04124-0)
Article received August 22, 2012. Article accepted November 4, 2012.