INTRODUCTION Auditory Brainstem Response (ABR) is a type of test which evaluates hearing integrity. It is used as a complement of audiological procedures helping when diagnosing hearing problems (1).
It is an electro-physiological evaluation, when a brief acoustic signal with a quick start causes synchronized neurological events. These are measured resulting in waves coming from hearing pathway up to the inferior colliculus (2). They are potentials of brief latency generated by sequential and synchronous activation of nervous fibers along hearing pathway, showing neurological integrity of the hearing pathways (3).
The clinical applicability of such potentials was increased due to the fact that they are captured in a non-invasive way using surface electrodes (4).
Beyond the most common clinical applications of ABR such as determination of electro-physiological hearing threshold, which constitute its main clinical application in children, and evaluation of hearing pathways from brainstem in adults (5), late national publications report the importance of ABR on topodiagnosis of central vestibular syndrome (6), on hearing neuropathy (7,8) and on West syndrome (9).
When performing the differential diagnosis between cochlear and retrocochlear hearing loss, the most used criteria on the ABR analysis are: absolute latencies (AL), interpeak latencies (IPL) and reprodutibility of waves I, III and V (10).
The current study focus on the analysis of values of absolute latencies of waves I, III and V and of interpeak latencies I-III, III-V and I-V.
In previous studies, it is shown the probability of basing on values of normality when analyzing ABR tracing, though parameters should be the same. Many times researches do not detail the used parameters, besides there is no agreement on normal values of latencies. For that reason, each clinic should develop its own set of normal values of latencies, through measuring ABR in a group from 15 to 40 subjects with normal hearing (11,12)
Pathological factors such as age and gender can influence on latencies of ABR. The need of establishing separate standards for men and women are questionable. Some authors report that despite the differences of latencies between the two are mild, they should be taken into consideration when establishing parameters of normality (13). Other authors disregard this need by the fact that the differences of gender-related latencies are mild and changeable (4). The equipment used is another factor to be considered when analyzing data, assuring reliable results and increasing diagnosis precision (14).
Stimulation parameters used such as intensity and speed of acoustic stimulus presentation also influence on records of responses (15).
On the ABR from individuals with normal hearing is possible to notice that when reducing intensity of acoustic stimulus, there is an increase of AL of waves of the ABR (2,10,11). The increase of the AL is also observed when increasing the speed of acoustic stimulus presentation, even in individuals with normal hearing. This occurs because the increase of speed of acoustic stimulus presentation harms the synaptic transmission (15,16). Tanaka et al., 1996 (17) and others, suggest that patients should be tested in low and high speeds of stimulus with the purpose of making ABR sensitive when detecting retrocochlear pathologies. The increase of speed of acoustic stimulus presentation reduces the reproductibility of waves (15), but it makes the test quicker (18), and it can also detect alterations which were not recorded when using lower speeds of stimulus.
The change shown in different studies as for values of normality, for the importance of performing biological calibration of the test equipment and for the need of each lab obtains its own normative data for ABR application led into the accomplishment of this current research.
The target of this study is to characterize the normality of latencies of ABR in both different intensities and speeds of acoustic stimulus presentation with the purpose of using the obtained values on the clinical practice.
MATERIAL AND METHODSThe current research was approved by the Ethics Committee - Tuiuti University - Paraná, protocol number 089/2003. All individuals authorized the accomplishment of the research and the publicizing of its results (Annex 1) according to Resolution 196/96. 20 individuals with normal hearing were chosen. 10 of them were female and 10 male, aging between 18 and 30 years. Age and quantity of individuals were selected according to Hood 1998 (11), though the number of samples was reduced when there was the need of separating them into male and female groups.
After obtaining normal results on audiological evaluation (threshold of threshold tonal audiometry up to 20 dBNa, tympanometric curve type A and Transient Evoked Otoacoustic Emissions and Distortion Product bilaterally present) the individuals were submitted to ABR research. The equipment used was audiometer AC40 and impedance audiometer AZ26 - Interacoustic. AUDIX was used to record Acoustic Otoemissions and two-channel-Bio-logic was used to auditory brainstem response research, installed in an acoustically designed and electrically isolated room.
Stimulation and record parameters were established according to Hernández et al. 2003 (10), in order that the results of this research would be compared with the literature which contains the same test parameters.
It was used a click stimulus of reversed polarity with a speed of 19 clicks per second (c/s). Within this speed, the stimulus was presented in the intensities of 90, 70, 50 and 30 dBnHL. Two response records were collected in each of the intensities, with the purpose of verifying the reproductivity of waves. The intensity of 20 dBnHL could have been evaluated, though the aim of the study did not focus on researching electro-physiologic hearing threshold. Each response was composed of 1600 promediation, in a time of analysis of 16,13 ms, and a monoaural presentation was used through ear phones TDH-39. After obtaining responses from different stimulus intensities, the click was presented with a speed of 57,7 c/s and constant intensity of 90 dBnHL, in order to analyze the influence of speed of the click on response record. The gain used to the records of waves ranged between 75,000 and 150,000 mv.
According to The ten-twenty electrode system of international (19), the grounding electrode was placed at the front, on Fp2, the reference electrode on Fz and active electrodes on A1, on the lobe of left ear, and on A2, on the lobe of right ear. Each place where the electrode would be applied with conductive paste in its inferior surface was carefully prepared using abrasive gel and alcohol-soaked gauze in order to remove any dirt. Those were attached on patient skin with the aid of a micropore. A contact electrical impedance of the electrodes was verified before and during the collection of records. It remained below 5 KOhms not exceeding 2 KOhms between the electrodes.
The wave peaks were identified and marked with Roman numeral I, II and V, and it was considered as ´waves´ only the ones with reprodutibility. Through this wave marking, it was possible to obtain values of the AL of waves I, III e V, and of IPL I- III, III- V and I-V. The analysis of the results comprehended:
1) Comparison of the studied variables (Absolute Latencies I, II and V, Interpeak Latencies I-III, III-V and I-V), from different stimulus intensities (90, 70, 50 and 30 dBnHL) in order to analyze the influence of such intensities.
2) Comparison of the studied variables in two frequencies of stimulus presentation (19 and 57.7 c/s) in order to analyze the influence of the stimulus on the ABR.
3) Statistical analysis using Student's t-test with level of significance at 5 % (a=0.05).
4) Obtention of average values and trust intervals (2.5 standard deviations).
RESULTS Through the analysis of records from the ABR, it was possible to obtain average values, standard deviations and trust intervals from the absolute latencies and interpeaks of waves I, III and V from the examined subjects. Such values, as much as the influence of intensity and speed of stimulus presentation over ABR will be shown.
Influence of Intensity of the Click over Absolute Latencies from the ABR It was observed increases on absolute latencies and reduction on amplitude of waves when reducing the intensity of the acoustic stimulus on the record of ABR.
Picture 1 shows one of the records from the ABR from the examined subjects, focusing on the increase of absolute latencies and reduction on the amplitude of waves I, III and V, as intensity was reduced from 90 to 30 dBnHL. Wave V was the most robust component, and it is easily seen in all applied intensities of the stimulus.
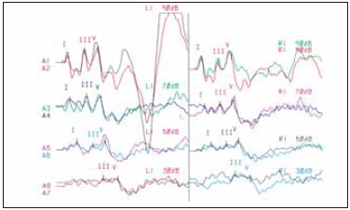
Picture 1. PEATE in different incentive intensities acoustic.
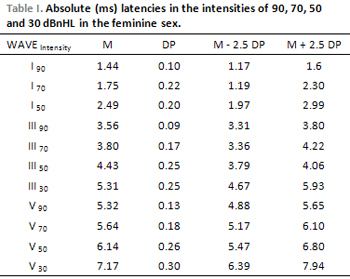
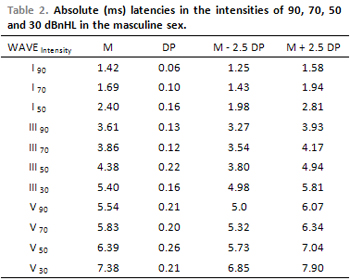
The average of the AL from wave V was greater for men in all intensities of the stimulus, and this difference is statistically significant. Therefore, the average of the AL from wave I, in intensities 90, 70 and 50 dBnHL and from wave III in 50 dBnHL, presented higher in women with no statistically significant difference.
In general, when reducing the click intensity, the AL from wave I had a higher increase comparing to the AL from waves II and V.
Table 1 displays the average values (M), standard deviations (SD) and trust intervals of the absolute latencies from waves in different intensities of the acoustic stimulus in women and Table 2 displays it in men.
The AL from wave V increased, in a non linear way, due to the reduction of the stimulus intensity, showing a higher increase of the latencies in low intensities of the stimulus (Chart 1).
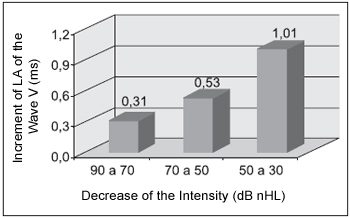
Chart 1. Increase of LA of the wave V due to the decrease of the intensity of the incentive.
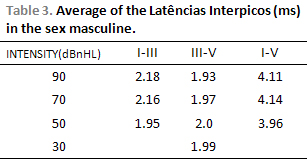
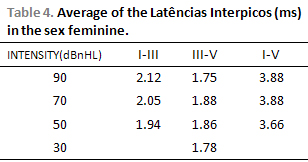
There is a slight reduction of IPL I-III and I-V and an increase of IPL III-V when reducing the intensity of acoustic stimulus in both men and women, though such variations do not present any statistically significant differences, i.e, interpeak latencies remain constant when reducing the intensity of the stimulus (Table 3 and 4).
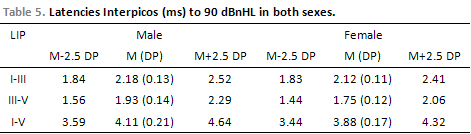
There was no statistically significant difference on IPL between right and left ears, and as for gender, the IPL I-III, III-V and I-V were greater in men than in women with statistically significant difference for the IPL III-V and I-V at 90 dBnHL. For this reason, average values and trust intervals were calculated separately for men and women (see Tables 3, 4 and 5).
Influence of Speed of the Click over Absolute Latencies of ABRWhen analyzing the influence of speed of the stimulus over ABR record, we could observe that an increase of speed of the stimulus made the test quicker and the absolute latencies of waves increased.
When increasing the speed of acoustic stimulus presentation from 9 to 57.7 c/s, the absolute latencies of waves I, III and V increased, and the amplitudes considerably reduced, although they were not object of this study. Picture 2 displays the reduction of amplitudes and the increase of absolute latencies originated from the increase of speed of acoustic stimulus presentation (Table 6). There was no statistically significant difference on the AL of waves when increasing the speed of stimulus presentation, except for wave III in women.
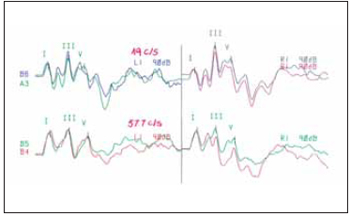
Picture 2. Registration of PEATE with speed of 19 and 57.7 c/s.
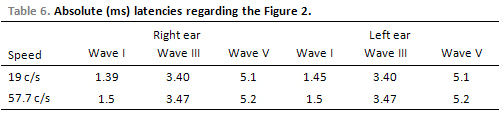
There was an average increase of absolute latencies when increasing the speed of stimulus presentation. This increase on the AL was similar between men and women, and when analyzing both, the average increase of the AL of wave V (0.35 ms) was higher than the average increase of the AL of waves I and II when increasing the speed of stimulus presentation (Chart 2).
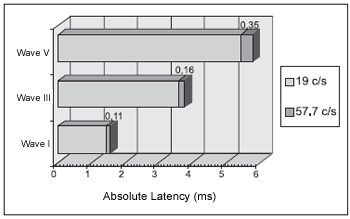
Chart 2. Average of the increase of LA of the waves I, III AND V to the to increase the speed of the click of 19 for 57.7 c/s.
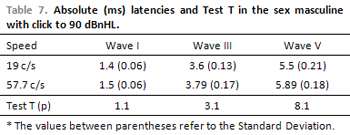
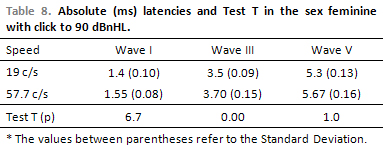
Table 7 displays the average values of the AL of waves I, III and V on different speeds of stimulus presentation, with click at 19 and 57.7 c/s at 90 dBnHL in men, and table 8 displays it in women.
Influence of Speed of the Click over Interpeak Latencies of ABRThe increase of speed of the stimulus presentation influenced the absolute latencies, and also caused an increase on interpeak latencies of ABR.
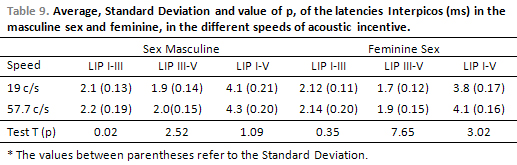
Student's t-test showed an non-statistically significant increase on IPL I-III, III-V and I-V when increasing the speed of the click from 19 to 57.7 c/s in both men and women, except on IPL I-III in men.
Table 9 displays average values, standard deviations and p values coming from Student's t-test for both men and women.
DISCUSSIONThe results of the current research suggest normal values on the analysis of the ABR, though the number of the subjects examined is narrow, what suggests an increase of the used sample.
Besides, this study describes a technique of increase of the speed of acoustic stimulus presentation, which makes the test sensitive when detecting retrocochlear pathologies. This technique was already studied by other authors, though hardly found in Brazilian literature.
The main findings in the scientific literature regarding the features of ABR from individuals with normal hearing and also regarding the intensity and speed of click presentation were collected and compared to the results from this study.
The increase of absolute latencies when reducing the intensity of the acoustic stimulus, observed in this study, was also reported by other authors (2,11).
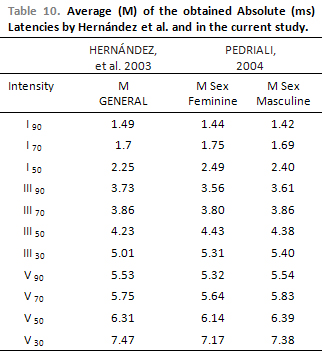
Table 10 displays the average values of the AL of waves I, III and V on different stimulus intensities from the current study and those by Hernández et al. 2003 (10), who used the same parameters of evaluation.
Although these authors had calculated the general average for latency values, the current study sorted a set of values for men and another set for women, because of the statically significant difference on values of AL of wave V between men and women and also following the recommendations by Elberling and Parbo, 1987 (13). This reduced the size of sample, which should contain a higher number of individuals examined in order to increase the trust of these values.
There are differences on values among each study, and although being mild, those differences are important when considering that on ABR a slight increase on values can influence on result of this test. This can emphasize the importance of obtaining proper values of normality for each clinic, according to recommendations by Hood, 1998 (11) and Figueiredo and Castro Júnior, 2003 (12).
Stockard et al., 1979 (20) observed in their studies that as intensity reduces from 70 to 30 dBnHL, the increase of latencies was higher for wave I and lower for wave V. These findings were also observed in the current study when reducing intensity from 90 to 30 dBnHL. Intensity of 20 dBnHL could have been evaluated, though the focus of the current study was not the research of the electro-physiologic hearing threshold.
Another finding, as for the AL increase, observed in the current study and already reported by Hood, 1998 (11), was a non-linear increase of the AL of wave V when reducing the intensity of the acoustic stimulus, which presented higher increases in lower intensities.
As for interpeak latencies, the slight reduction of IPL I-III and I-V and the increase of IPL III-V when reducing the intensity of the acoustic stimulus in men and women were also reported by Stockard et al, 1979 (20).
Souza et al., 2001 (21) also found statistically significant difference between IPL from right and left ears on the examined subjects. As for gender, Lopez-Escamez et al., 1999 (22), showed the influence of this factor over IPL. This influence was also observed in the current study which obtained, in its results, IPL I-III and I-V expressively lower in women than in men.
As for the influence of the stimulus speed over ABR, the results agreed with studies by Burkard e Sims, 2001 (15), which report that the increase of stimulus speed makes test quicker, latencies increase and amplitudes of waves are reduced, what makes their clearness and reprodutibility difficult.
Table 11 displays average values of the AL and IPL of waves I, III and V in milliseconds (ms), with speed of 57.7 c/s in the current study and those values by Hood, 1998 (11). Although similar, all values from the current research were lower than the ones by the author.
The average of the increase of the AL of wave V when reducing speed of stimulus presentation, from the current research (0.34 ms), agrees with Hood, 1998 (11), who considers normal any increase of latencies lower than 0.6 or 0.8ms, Lima and Fukuda, 1999 (16), comparing values of the AL and IPL of ABR from individuals with normal hearing with click at 11 and 61c/s, observed an increase, statistically significant, in all values of latencies when increasing stimulus speed. The current study also had increase on the AL and IPL, though this increase was not statistically significant, perhaps by the fact that the proportion of the speed increase had been lower than the one used by the other authors.
CONCLUSIONFrom the results in this study, we concluded that:
a) It was possible to obtain values of AL and IPL of waves I, III and V in young adults with normal hearing in different intensities and speed of acoustic stimulus. These values will be used in the clinical practice as a parameter of normality.
b) Speed and intensity of acoustic stimulus are important factors to be taken into consideration on ABR interpretation, thus these stimulation parameters influence on values of absolute latencies of waves I, III and V and on interpeak latencies I-II, III-V and I-V.
c) the use of proper parameters of evaluation can show a series of advantages when interpreting results of ABR as a possibility of comparing results of the performed tests with normative data exactly in the same conditions of evaluation.
REFERENCES1. Misuek F, Boreinstein S, Hall J, Schwaber M. Audiometria de tronco encefálico (ABR): neurodiagnóstico e aplicações intra-operatórias. Em: Katz J. Tratado de Audiologia Clínica. 4. ed. São Paulo: Manole, 1999, pp.349-371.
2. Maroonroge S. Overview of Auditory Brainstem Response (ABR): Applications and Limitations. Speech and Hearing Review 2001, 2:214-24.
3. Junqueira CAO, Frizzo ACF. Potenciais Evocados Auditivos de Curta, Média e Longa Latência. Em: Aquino AMCC. Processamento Auditivo: Eletrofisiologia e Psicoacústica. São Paulo: Lovise, 2002. pp.64-86.
4. Ferraro JA,; Durrant. Potenciais Auditivos Evocados: Visão Geral e princípios básicos. Em: Katz J. Tratado de Audiologia Clínica. 4a ed. São Paulo: Manole, 1999, 228-281.
5. Valete CM, Decoster DMH, Lima MA, Torraca TS, Tomitav S, Kós AOA. Distribuição por sexo e faixa etária das aplicações clínicas da audiometria de tronco encefálico. Acta AWHO 2002,3:21.
6. Aquino AMCM., Colafemina JF. Topodiagnóstico nas síndromes vestibulares centrais. Acta AWHO 2000, 19:26-31.
7. Ogeda ECM, Matas CG. Neuropatia auditiva por Kernicterus: estudo de caso. Pró-fono 2002, 14:247-252.
8. Parra VM, Matas CG. Estudo das características audiológicas em casos de neuropatia auditiva. Pró-fono 2002, 14:241-246.
9. Pereira Filho AL, Malucelli DAB, Ferreira LLA, Gonçalves F, Silveira AM. Avaliação dos achados ao exame dos potenciais evocados do tronco cerebral em indivíduos com síndrome de West. Rev. Bras. Otorrinolaringol 2004, 70,1:90-93.
10. Hernandéz JD, Castro FZ, De Prat JJB. Normalización de los Potenciales Evocados Auditivos Del Tronco Cerebral I: Resultados en una muestra de adultos normoyentes. Auditio- Revista Eletrónica de Audiología 2003, vol.2. Disponível em: www.auditio.com. Acesso em: 20 de dezembro de 2003.
11. Hood L. The normal auditory brainstem response. Em: Hood L. Clinical applications of the auditory brainstem response. San Diego - London: Singular, 1998, pp.126-144.
12. Figueiredo MS, Castro Junior NP. Potenciais Evocados Auditivos de Tronco Encefálico (ABR). Em: Figueiredo MS, Castro Junior NP. Emissões Otoacústicas. São José dos Campos: Pulso 2003, pp.85-87.
13. Elberling C, Parbo J. Reference data for ABRs in retrocochlear diagnosis. Scandinavian Audiology 1987. 16:49-55.
14. Flabiano F, Leite R, Matas C. Audiometria de tronco encefálico em adultos audiologicamente normais: comparação das latências absolutas das ondas I, III, V, interpicos I-III, III-V, I-V, amplitudes das ondas I, III, V e relação da amplitude V/I, obtidas em dois equipamentos diferentes. Acta AWH 2002, v.21,1. Disponível em: http://www.actaawho.com.br/edicao/conteudo.asp?edi_id=5&tpc_id=1&con_id=11 Acesso em: 18 nov. 2004.
15. Burkard R.F, Sims D. The human Auditory Brainstem Response to high click rates: Aging effects. American Journal of Audiology 2001, 10:53-61.
16. Lima MA, Fukuda Y. Audiometria de Tronco Encefálico em pacientes HIV positivos Assintomáticos: Análise nas freqüências de 11 e 61 cliques por segundo. Revista Brasileira de Otorrinolaringologia 1999, 65:404-11.
17. Tanaka H, Komatsuzaki A., Hentona H. Usefulness of auditory brainstem responses at high stimulus rates in the diagnosis of acoustic neuroma. ORL J Otorhinolaryngol Relat Spec 1996, 58:224-8.
18. Stürzebecher E, Cebulla M, Neumann K. Click-evoked ABR at high stimulus repetition rate for neonatal hearing screening. International Journal of Audiology 2003, 42:59-70.
19. Klem G.H, Lüders HO, Jasper H, Eljer RC. The ten-twenty electrode system of international federation. Electroencephalography and Clinical Neurophysiology 1999, 52:3-6.
20. Stockard JJ, Stockard JE, Westmoreland B, Corfits J. Brainstem auditory evoked responses: Normal variation as a function of stimulus and subject characteristics. Archives of Neurology 1979, 36:823-831.
21. Souza MA, Beltrame CB, Cechella C. Audiometria de Tronco Encefálico: Análise da latência interpicos em sujeitos do sexo feminino com audição normal. Fonoaudiologia 2001, 1:16-23.
22. Lopez-Escamez JA, Salguero G, Salinero, J. Age and sex differences in latencies of waves I, III and V in auditory brainstem response of normal hearing subjects. Acta Otorhinolaryngol Belg 1999, 53:109-115.
1. Master in Disturbances of the Communication (Fonoaudióloga).
2. Powder-doctor for Université of Montreal, Canada (Fonoaudióloga).
University Tuiuti of Paraná - Curitiba - Paraná.
Address for correspondence: Street Colonel Amazon Marcondes, 285 - Aptº 31. Cabral. Curitiba / PR. ZIP CODE 80035-230. Telephone: (41) 253-4327 or 9951-4078. E-mail: ipmacedo@uol.com.br
This article was submitted in SGP - Sistema de Gestão de Publicações (Publication Management System) of the RAIO in 12/1/2006 and approved in 7/4/2006 19:44:26.