INTRODUCTIONMouth breathing can cause structure and function alterations on stomatognathic system. Assistance and studies in this area have been more emphasized due to the need of professionals for treating these types of alteration.
Nose should be the only way for breathing, as nose is responsible for moisturizing, warming and lubricating the inhaled air, and also for protecting inferior air passages.
Therefore, we can find individuals who breathe through mouth or even mix mouth and nose when breathing. This can be a vicious habit or alterations such as adenoid hypertrophy, allergies, septum deviation and nasal pyramid and others.
The mouth breathing can cause alteration on stomatognathic structures, which are common in different functions such as mastication, swallowing, pronunciation and development of odontostomatological structures (1). Thus, in the mouth breather, dental malocclusion, open mouth position, labial hypotonia, tongue altered position are alterations which can lead to atypical swallowing (2).
It is known that growth, development and function of bone structures from oral cavity are closely connected to bucofacial muscles. They need to be in accordance in order to provide good occlusion, so teeth will arise in a dynamic environment where face, mastication and tongue muscles work (3).
Anterior open bite (a kind of malocclusion by the presence of a negative vertical trespass between cut edges of the anterior, upper and lower teeth) sometimes comes from an orofacial myofunctional irregularity by long term harmful habits. This type of malocclusion is often associated with atypical swallowing cause, as the presence of this trespass would make anterior projection of tongue between teeth during swallowing easier (4).
Some researches have showed the relation between presence of malocclusion and atypical swallowing (5-8).
Regarding the mouth breather, literature agrees when referring to occlusion and swallowing alterations found in this group of patients (9-11), therefore, studies which clarify the influence of occlusion alteration of swallowing from mouth breather were not found.
The target of this study is to verify the influence of anterior open bite of swallowing from the mouth breather.
MATERIAL AND METHOD The Ethics Committee for Analysis of Projects - CAPPesq from Clinical Directory of HC-FMUSP has approved the Protocol of Research number 467/00 regarding the current study.
It as done a research of the data from patients submitted to Phonoaudiological Evaluation at Ambulatory of Oral Motricity at HCFMUSP. Procedure consisted of data from records of phonoaudiological evaluation of each patient regarding breathing, dental occlusion and swallowing.
All individuals presented ENT diagnosis of nasal obstruction by adenotonsillar hypertrophy and mouth breathing.
72 patient records were examined. This group of patients was composed by men and women aging from 5 to 13. They were divided into four groups: G1 - 17 patients with anterior open bite aging between 5 and 7 years; G2 - 17 patients with normal dental occlusion, matched with patients from G1 by gender and age; G3 - 19 patients aging between 8 and 12 years with anterior open bite and G4 - 19 patients with normal dental occlusion, matched with patients from G3 by gender and age.
Dental Occlusion classification was performed by an orthodontist through pictures of each patient obtained in the moment of phonoaudiological evaluation. The critearia for the classification were the following (4,12).
Normal Occlusion: when in arrow-shaped, medium, anteroposterior axis plane, the mesiovestibular cuspid of the first molar is in occlusion with mesiovestibular groove of the first lower molar; in transverse plane, when upper teeth stand out lower teeth and touch the ones from the same arch and their opposed ones and in frontal, superior inferior axis plane, when upper teeth cover 1/3 of the crown of the lower teeth.
Anterior Open Bite: when in frontal plane, upper-lower axis, we can observe the presence of room between anterior, upper and lower teeth and posterior teeth are in occlusion (4).
Data referring to classification of swallowing were taken from phonoaudiological evaluation records of each patient. These evaluations are performed by speech doctors in the department of Oral Motricity of HCFMUSP. The criteria for classification of swallowing are the following:
- Normal swallowing: labial sealing and tip of the tongue placement on the papilla (3);
- Atypical swallowing: atypical pressure of lips, tongue pressure over anterior teeth or between anterior arches and compensatory head movement (13).
Individuals with genetic alterations; with facial abnormalities and individuals who were or had been under phonoaudiological therapy and/or orthodontic treatment were not included in this sample.
STATISTICAL METHODIn order to analyze data in this study, it was made use of:
- Qui-square test: used to compare standard of swallowing with type of occlusion. P < 0.05 was considered statistically significant.
- Fisher accurate test (14): used to compare standard of swallowing with type of occlusion between ages from 5 to 7 and from 8 to 12 years. P < 0.05 was considered statistically significant.
It was used an asterisk (*) when results were statistically significant.
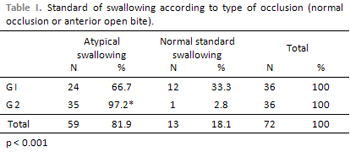
RESULTSTable 1 shows standard of swallowing of patients with normal occlusion - G1 and of patients with anterior open bite - G2. It was observed statistical difference as for the presence of atypical swallowing between groups 1 and 2.
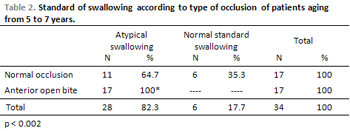
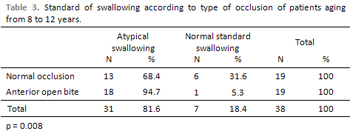
Tables 2 and 3 show results as for standard of swallowing in each studied age. It was observed statistical difference between the presence or not of atypical swallowing only in patients from 5 to 7 years old.
DISCUSSIONLiterature does not agree on the age when a child achieves a standard of mature swallowing. It varies from 18 months to 6 years of age (15,16). In this study, only few records could be found in transitional phase, as it is composed by children from 5 to 12 year old.
Therefore, researches with the target to verify the percentage of children with standard of immature swallowing after 4 years of age showed altered swallowing in 3% to 48% of them (8,18-20). Even considering that some of our children are in transitional phase of swallowing, our result of 81.9% of children with standard of altered swallowing is higher than the results found in previous studies.
In this way, we could say that there is a relation between mouth breathing and presence of atypical swallowing, as we have observed an expressive higher number of children with standard of altered swallowing. These data agree on findings by Neiva & Wertzner (1996) and Junqueira et al. (2002) and disagree on the ones by Matos et al. (2002) (8).
Our study confirmed the relation between mouth breathing and atypical swallowing, which was already mentioned in previous studies. These ones did not clear the influence of occlusion alterations on standard of swallowing of the mouth breather, since there is a relation between mouth breath and anterior open bite and a relation between anterior open bite with atypical swallowing (15,6,7,9,21,11)
According to the studied literature, we could observe that children with anterior open bite are statistically subjected to present atypical swallowing, according to Moraes (1994); Neiva & Wertzner (1996) and Wadsworth (1998). Despite such accordance, the percentage of atypical swallowing found in children with anterior open bite (97.2%) was higher than the findings from the collected literature, reinforcing, thus, the influence of mouth breathing in the presence of atypical swallowing.
Matos et al. (2002), do not report statistical importance in the relation between anterior open mouth and presence of atypical swallowing.
It is important to mention that such relation occurred in a significant manner only in children aging from 5 to 7 years. According to Granville-Garcia et al. (2000), we could assign this result to age, since these children would have less condition when compensate the presence of anterior room inside the mouth provided by open bite.
As we did not find a statistically significant correlation between atypical swallowing and anterior open bite in mouth breathers in patients from 8 to 12 years of age, we could affirm that the reason these children swallow in a improper way do not depend only on dental occlusion, but on open mouth position, in order to keep air flow and/or by the presence of a hypertrofied palatine tonsil (2, 22-24).
We can assure that the correlation between mouth breathing and atypical swallowing is not only because of dental malocclusion. Such result can be affirmed when comparing the percentage of children with malocclusion and atypical swallowing (66.7%) with result in the literature (5).
CONCLUSIONAccording to the analysis of the result from this study, we conclude that there is a statistical significant relation between mouth breathing and presence of atypical swallowing.
Despite this study confirm a higher tendency of children with anterior open mouth presenting atypical swallowing, we found a higher percentage than in the collected literature. We so conclude that the correlation between mouth breathing and atypical swallowing is not only because of dental malocclusion.
REFERENCES1. Carvalho GD. S.O.S. Respirador Bucal. 1ª edição. São Paulo: Lovise; 2003.
2. Marchesan IQ. Correção Forma-Função - Sistema Estomatognático. In: Marchesan IQ. Motricidade Oral: uma visão clínica do trabalho com outras especialidades. São Paulo: Pancast; 1993, 25-34.
3. Marchesan IQ. Avaliação e terapia dos problemas de respiração. In: MarchesanIQ. Fundamentos em Fonoaudiologia: aspectos clínicos da motricidade oral, Rio de Janeiro: Guanabara Koogan; 1998.
4. Kuramae M, Tavares SW, Almeida HA, Almeida MHC, Nouer DF. Atypical swallowing thrust correction associated to anterior open bite: a clinical case report. J Bras Ortodon Ortop Facial, 2001;6(36):493-501.
5. Moraes SEZ. Oclusão normal e maloclusão: morfologia e fonoarticulação em crianças com dentadura mista, São Paulo, 1994. (Tese de Mestrado em Ciências dos Distúrbios da Comunicação Humana: Campo fonoaudiológico - EPM).
6. Neiva FCB, Wertzner HF. Descrição das alterações miofuncionais orais em crianças de 8:1 a 9:0 anos. Pró-Fono, Set. 1996;8(2):36-44.
7. Wadsworth MS. The prevalence of orofacial myofunctional disorders among children identified with speech and language disorders in grades kindergarten trough six. Int. J. of Orofacial Myology, 1998;24.
8. Matos MJF, Lima GQT, Costa RCN, Ribeiro CCC. Avaliação da deglutição atípica em crianças de 4 a 7 anos em rede escolar pública. J Bras Fonoaudiol, Curitiba, Jan-Mar. 2002;3(10):40-47.
9. Biazzetto ZC, Zenaro PS, Salcedo PHT. Alterações fonoaudiológicas encontradas em crianças com hipertrofia da amígdala palatina. Revista Cadernos São Paulo: Centro Universitário São Camilo, Jan-Jun. 2000;5(1):59-69.
10. Junqueira PAS, Di Francesco RC, Trezza P, Zeratti FE, Frizzani R, Faria MEJ. Alterações funcionais do sistema estomatognático pré e pós-adenoamigdalectomia. Pró-Fono Revista de Atualização Científica: Carapicuíba, Jan-Abr. 2002, 14(1):17-22.
11. Manganello LC, Silva AAF, Aguiar MB. Mouth breathing and dentofacial alterations. Rev. Assoc. Paul. Cir. Dent., 2002;56(6):419-22.
12. Pillon J, Vieira MM. Freqüência da ocorrência de maloclusão dentária em crianças com hábitos orais deletérios. Revista Fono Atual, São Paulo: Pancast, Out-Dez. 2001, 4(17):23-31.
13. Guedes ZCF. Deglutição atípica e o fonoaudiólogo. In: Sih, T. Otorrinolaringologia Pediátrica, Rio de Janeiro: Revinter; 1998.
14. Kirkwood BR. Essentials of Medical Statistics. Oxford, Blackwell Science Ltd; 1988. 234p.
15. Ferreira LP, Barros MCPP. In: Temas de Fonoaudiologia. 2ª edição, São Paulo: Loyola; 1985.
16. Braga GC, Machado CP. Deglutição Atípica. In: Petrelli E. - Ortodontia para Fonoaudiologia: Lovise, São Paulo, 1994;147-148.
17. Granville - Garcia AF, Barata JS, Brayner RG, Meneses SRS, Closs LQ. Fisiologismo da deglutição infantil normal. J Bras Fonoaudiol, Curitiba, Jan-Mar. 2000;1(2):27-29.
18. Penteado RZ, Almeida VF, Leite EFD. Saúde bucal em pré - escolares: um estudo fonoaudiológico e odontológico. Pró-Fono, Set. 1995, 7(2);21-29.
19. Pereira LF, Silva AMT, Cechella C. Ocorrência de hábitos orais viciosos e distúrbios fonoarticulatórios em indivíduos portadores de deglutição atípica. Pró-Fono, Mar. 1998;10(1):56-60.
20. Tomé MC, Guedes ZCF, Silva AMT, Cechella AC. Estudo da ocorrência de alterações da deglutição e da oclusão dentária em crianças com queixa de falar errado. Pró-Fono, Mar.1998;10(1):61-65.
21. Fayyat ELRC. A influência dos hábitos orais e a respiração bucal no aparecimento de mordida aberta anterior em crianças com dentição decídua. Revista Fono Atual. São Paulo: Pancast. 2000;3(12):36-40.
22. Dragone MIOS. Deglutição Atípica: uma prática clínica. In: Distúrbios da Comunicação. São Paulo: Educ, Jul-Set. 1986;1(3):119-127.
23. Ourique S. A importância da integração entre odontologia e fonoaudiologia na reabilitação de pacientes portadores de desordens na articulação temporo-mandibular. Revista Fono Atual, São Paulo: Pancast, Out-Dez. 1997;1(3):31-33.
24. Subtelny JD, Subtelny JD. Abnormal deglution and myofunction therapy: facts and fallacies. In: Stewart RE. Pediatric Dentistry. St. Louis: Mosby; 1982.
1. Improvement in Clinical Phonoaudiology by Hospital das Clínicas da Faculdade de Medicina - USP (Contributor Speech doctor in the department of Oral Motricity from ENT Clinic Division of Hospital das Clínicas da Faculdade de Medicina - USP.
2. Speech Doctor master in Experimental Physiopathology by FMUSP (Speech Doctor)
3. PhD in Human Communication Disorders by Universidade Federal de São Paulo (Speech Doctor at ENT Clinic Division of Hospital das Clínicas da Faculdade de Medicina - USP.
3. PhD student in Science by Faculdade de Medicina da Universidade de São Paulo (Assistant Odontologist of the Odontology Division of Hospital das Clínicas da Faculdade de Medicina - USP.
4. Specialist in Clinical Audiology by Santa Casa de Misericórdia de São Paulo (Speech doctor reseacher of the Oral Motricity department of the ENT Clinic Deivision of Hospital das Clínicas da Faculdade de Medicina - USP.
Study done at ENT Clinic Division of Hospital das Clínicas da Faculdade de Medicina - USP.
Mail address: Fga. Catiane Maçaira de Lemos - Rua Padre Estevão Pernet, 783 - Tatuapé - São Paulo / SP - Telefone: (11) 2294-2725 - E-mail: catianemacaira@uol.com.br
This article was submitted to SGP - Sistema de Gestão de Publicações (Publication Management System) from RAIO on January 4, 2006 and was approved on June 11, 2006 22:37:16.