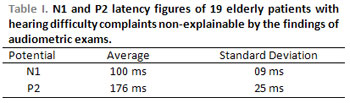
INTRODUCTION Determining topographic levels of a hearing disorder is not as simple as it seems, especially when the individual complains of hearing difficulties in speech understanding when auditory tests are in normal conditions.
It has been noticed an increase of elderly people with hearing disorder-related symptoms due to the rising number of the life expectancy of this population.
Complaint of "listen, but do not understand" symptom, mainly in noise environment, where there are music and people talking, is becoming more frequent from people aging over 60.
Mild to moderate sensorineural hearing loss on speech frequency, especially for sharp sound, has been affecting most of those individuals and it is also the reason for their peripheral-otological-alteration-based complaints.
Another explanation which should be analyzed is for complaints of individuals with normal hearing test or hearing loss on frequencies of 4000 HZ.
In the past few years, alterations on nervous system on hearing arising from aging have been taken as a serious factor of speech understanding by the elderly with or without expressive hearing loss (1).
Such alterations could justify the fact that only 40 to 60% of the elderly who wear hearing aid is favored by it(2).
Audiology has been increasing regarding research, by helping evaluation, diagnosis and habilitation and rehabilitation interventions on hearing system pathology.
Alterations on central auditory process tests involving hearing abilities of localization, attention, figure-ground, memory, recognition, analysis and auditory synthesis can be present on individuals, with or without hearing loss, who complain of communication difficulty(3).
Conventional central auditory process tests take long to be performed and they depend on patients' cooperation.
Electrophysiological approach to evaluate cortical auditory activities can be quicker and less tiring for patients.
Evoked auditory potentials is fundamental on audiology process, though the ability to receive electric potentials, which are made into several levels of the nervous system in response to acoustic stimulation, counts for a single diagnosis method.
The waves N1 and P2 were the first evoked auditory potentials on hearing electrophysiology history described by Davis P.A.(4).
Such potentials are related to auditory system on primary and secondary cortical areas involved in the central auditory process. Achieving them does not depend on patient's active participation, but requiring they become alert and still(5).
They are great in amplitude terms and easy to obtain. Latency N1 is usually from 80 to110ms and P2 from 150 to 200ms.(6)
The Potential N1 starts from the primary auditory cortex in the lateral and superior area of the superior temporal gyrus. The potential P2 also starts from the same point as N1 and goes along Sylvian fissure contralaterally to stimulation, by involving cortical areas of auditory agnosia(7). Its electric activity core is placed next to Heschl's gyrus(8) and its latency has been considerably higher in the elderly(9).
P300 (P3) is another long-distance latency auditory potential which has been a topic of study on elderly auditory(10,11), in latencies between 250 and 350ms in young adults. In order to arise it, it is necessary the active participation by the patients who should count on the different frequency stimuli P300 is not achieved if patient only hears but is not able to count any stimulus. That is why such potential originates from the individual and is so-called endogenous. It is always found together with N1 and P2 which precede it.
The potentials N1 and P2 were used to determine auditory threshold on difficult-to-evaluate patients(12,13) and has been presenting with alterations on neural pathology which affects brain auditory cortex(14,15,16,17,18,19).
Researches on N1 and P2 have been bringing important information on the elderly brain activity with no clear neural pathology.
The amplitude N1 was lower in the elderly group when compared to young adults. The elderly was stimulated by hearing sounds in one ear and conversation sounds in the other(20).
The level of the acceptable background noise while hearing conversations was related to differences on latencies N1 and P2. That acceptable background noise is in dBs degree which measures the amount of noise a person can hear with no discomfort. Higher latencies were found in individuals who could bear more noise with no discomfort when talking. These two electrophysiological indicators were used regardless age, gender and hearing level(21).
The use of stimuli with speech sound in clear sound places has been applied to make electrophysiological test closer to everyday hearing conditions(22).
There is a notable clinic and scientific interest on studying auditory processing through cortical evoked auditory potentials. The reason is that it is believed they show sound recognition and/or detection(23).
All the information already mentioned assures the importance of studying electrophysiological evaluation of hearing process through evoked potentials of latencies N1 and P2 in elderly population who complain of difficulties in speech understanding and with normal conventional audiologic evaluation.
The target of this study is to evaluate N1 and P2 behavior by determining figures of latencies N1 and P2 in the elderly with hearing complaints and normal audiometry.
METHOD After being approved by the Research Ethics Committee of UFSM (process# 0078.0.246.000-05), 6 males and 13 females aging between 60 and 80 were selected. They searched for ENT clinic and were assisted by the first author of this study from January 2006 to June 2207. They reported good hearing but difficulty in speech understanding when people talked at the same time. All of them accepted to take part in the study by signing the Free and Clear Consent Term. All patients presented ENT exam in normal condition, audiometry test with up to 25 dB NA tonal threshold average in the frequencies of 500, 1000, 2000 and 3000 Hz and Percentage Index of Speech Recognition higher than 80% in both sides.
The exclusion data were: cerebral vascular accident history: cranial trauma; cerebral tumors; elderly insanity; schizophrenia; aphasia; chronic renal failure; drinking problems; Multiple Sclerosis; Parkinson, Huntington and Alzheimer's Diseases; psychoactive drug use; absences in evaluations and patients who did not agree on taking part in the study.
AMPLAID 315 audiometer by discending-ascending technique was applied to perform tonal audiometry tests.
The potentials N1 and P2 were achieved by using MASBE CONTRONIC and as stimulus Tone Bursts of 1000 Hz with 50 ms and 10 ms of rise decay times, through headphones, in simultaneous and binaural way, on the frequency of 0.8 pps, and intensity of 80 dB NA. Bioelectrical activity was between 1 and 20 Hz, the analysis gap was 1000ms and recorded from electrons placed in CZ-A1 and CZ-A2 with immitance lower than 5 Kohms and the difference between them no more than 2 Kohms. 240 stimuli were presented in a single intensity and repeated to affirm results. Patients were asked to keep open eyes staring at an aim within their sight field. In order to keep alert level in constancy, it was required the patients to keep counting the 2000 Hz stimuli, which were less frequent (N1 and P2 potential research was done together with the P300 one). Counting stimuli correctly was a criterion to validate the response to P300, which confirmed the patient's attention.
Latencies of N1 and P2 peaks (picture 1) were measured on the response by the frequent stimuli (1000 Hz), and normal-considered figures were 120 ms and 228 ms respectively (5).
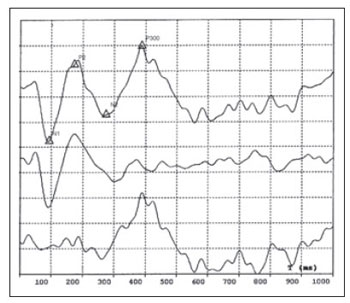
Figure 1. Example of Cortical Auditory Evoked Potential - Cortical Auditory Evoked Potential in response to a series of 300 50ms-duration tone bursts; intensity: 80 dBNA; obtained in a 1000 Ms gap; sensibility; 5µV/ div, from a 75-year-old female patient. The superior line displays the promediation of 60 responses to rare stimuli (2000 Hz) that patients could count. The intermediate line displays the promediation of 240 responses to frequent stimuli (1000 Hz), unknown by patient. The inferior line displays the result of the subtraction between the first and the second responses, which produced the cancelation of N1 and P2 and which made N2 and P300 stand out.
Results from amplitude measures from N1 and P2 as well as latencies and amplitudes from P330 will be soon topics for the coming studies.
RESULTS The N1 and P2 potentials were achieved in all individuals in response to 1000 Hz stimuli in constant way when researching P300 with intensity of 80 dBNA.
Table 1 displays the average of latencies with standard deviation for N1 and P2. The maximum figures for N1 and N2 were 120ms and 220ms respectively.
DISCUSSION Cranford (24) reported latencies of 97 ms (DP 7) for N1 and 187 (DP 22) in 40 individuals aging from 20 and 80 years (10 of them were between 60 and 80 years old) with normal hearing regarding their ages. They were volunteers in a study on the effects of contralateral noise presence when researching N1 and P2. These figures of latencies are quite similar to the ones of this current study.
Franco (25), when studying 25 volunteers in normal condition aging from 22 to 58 years (average age 38), reported 90 ms (DP 8) for latencies N1 and 180 ms (DP 18) for P2. Latencies for N1 were lower than the ones from this study and remained the same for P2.
Tampas (21) examined 21 young adults (average age of 24 years) and achieved latencies of 89 ms (DP 12) for N1 and 145 ms (DE 15). The difference in P2 latency should be related to the evaluated age, thus both N1 and P2 increase according to age. This increase does not mean much for N1, but it is fundamental for P2 which increases 40 ms between 20 and 80 years (26) on the average.
Latency figures from N1 and P2 in this study are considered normal according to the abnormal criteria on N1 and P2 research on adults: 1) obtained waves with no response; 2) absent waves; 3) N1 latency higher than 120 ms and 4) P2 latency higher than 228 ms applied by Musiek 1994(5) and, 5) they coincide with figures from other studies already mentioned.
Studies which relate central auditory process with potentials of long latency on elderly population have been focused on P300 research(8). Although N1 and P2 are displayed in all studies which research P300, we did not find any studies relating their latencies with difficulties on speech understanding in the literature.
Disorders on central auditory process should be suspected every time complaints of speech understanding and reception were higher than conventional audiometric evaluation professionals would suppose (little audiometric alteration for lost of communication complaints). Such suspicion should also be taken into consideration when hearing aid efficiency is lower than expected, by considering only conventional audilogical findings.
In the past few years, therapies for auditory process disorder have been important for providing a better hearing (and life) quality to the elderly with communication problems, by justifying more attention on diagnosing such disorder.
The electrophysiological evaluations of other dimensions of N1 and P2 as well as the researches on other potentials of auditory cerebral cortex are the targets of the coming studies by the current team, aiming to find objective tools on diagnosis and follow-up of the central auditory process disorders.
CONCLUSION Latencies of auditory potentials of N1 and P2 long latency did not present any alterations on elderly patients who complained of speech understanding difficulty and who presented normal tonal audiometry on frequencies lower than 4000 Hz, which suggested that the latency of such potentials is not affected by this type of hearing problem.
The fact that this population (complaining of speech understanding) did not present alterations on latency of such potentials suggests that hearing disorder would not be in the sites from those studied in this work electrophysiologically.
REFERENCES 1. Jerger J, Lew HL. Principles and clinical applications of auditory evoked potentials in the geriatric population. Phys Med Rehabil Clin N Am, 2004, 15: 235-250;
2. Humes LE. Issues in evaluating the effectiveness of hearing aids in the elderly: what to measure and when. Semin Hear, 2001, 22: 303-15;
3. Cruz O L, Kasse C A, Sanches M, Barbosa F, Barros F A. Serotonin reuptake inhibitors in auditory processing disorders in elderly patients: preliminary results. Laryngoscope 2004, 114(9):1656-9.
4. Davis P. Effects of acoustic stimuli on the waking human brain. J of Neurophysiol 1939, 2: 494-499.
5. Musiek FE, Baran JÁ, Pinheiro ML. Behavioral and Electrophysiological Tests Procedures. In: Musiek FE, Baran JA, Pinheiro ML Neuroaudiology - Case Studies. San Diego,CA: Singular Publishing Group; 1994.
6. Musiek K, Rintelmann W. Perspectivas atuais em avaliação auditiva, 1ª ed. São Paulo: Manole; 2001.
7. Steinschneider M, Kurtzberger D, Vaughan H Jr. Event-related potentials in developmental neurophysiology In: Rapin I, Segalowitz S. Handbook of Neuropsychol. Amsterdan: Elsevier; 1992, 239-299.
8. rowley KE, Colrain IM. A review of the evidence for P2 being an independent component process: Age, sleep and modality. Clin Neurophysiol 2004, 115:732-744.
9. Tremblay KL, Billings CJ, Rohila N. Speech evoked cortical potentials: effects of age and stimulus presentation rate. J Am Acad Audiol 2004, 15:226-237.
10. Nunes FB. Da Avaliação do P300 e do Processamento auditivo em idosos com e sem queixa auditivas. São Paulo, 2003, p1 (tese de mestrado-Escola Paulista de Medicina).
11. Fein G, Turetsky B. P300 latence variability in normal elderly: effects of paradigm and measurement technique. Electroencephalogr Clin Neurophysiol, 1989, 72: 384-294.
12. McCandless GA. Clinical application of evoked response audiometry. Speech Hear Res 1967, 10: 468-478.
13. Hyde M, Matsumoto N, Alberti P, Li Y. Auditory evoked potentials in audiometric assessment of compensation and medicolegal patients. Ann Otol Rhinol Laryngol 1986, 95: 514-519.
14. Shimazu H. Evoked response in eighth nerve lesion. The Laryngoscope, 1986, 10: 14-22.
15. Peronnet F, Michel F. The asymmetry of the auditory evoked in normal man and in patients with brain lesions. In: Auditory Evoked Potentials in Man: Psychopharmacology Correlates of ERPS. vol 2. 130-142, Basel: J Desmedt; 1987.
16. Knight R, Hilliard S, Woods D, Neville H. The effects of frontal and temporal-parietal lesions on the auditory evoked potential in man. Electroencephalogr Clin Neurophysiol 1980, 50: 112-124.
17. Jerger S, Jerger J. Audiological applications of early, middle and late auditory evoked potentials. Hearing Journal 1985, 38: 31-36.
18. Sherger M, Von Cramont D. Evoked dipole source potentials of the human auditory cortex. Eletroencephalography and Clinical Neurophysiology 1986, 65: 344-360.
19. Musiek F. Auditory evoked responses in site of lesion assessment. In: Rintelmann W Hearing Assessment. 2nd ed. Boston: Allyn & Bacon; 1991.
20. Hymel MR, Cranford JL, Stuart A. Effects of Controlateral Speech Competition on Auditory Event-Related Potentials Recorded From Elderly Listeners: Brain Map Study. Am Audiol 1998, 9: 385-397.
21. Tampas JW, Harkrider AW. Auditory evoked potentials in females with high and low acceptance of background noise when listening to speech. J Acoust.Soc.Am 2006, 119(3):1548-1561.
22. Tremblay KL, Friesen L, Martin BA, Wright R. Test-retest reliability of cortical evoked potentials using naturally produced speech sounds. Ear Hear 2003, 24:225-232.
23. Martin BA, Tremblay KL, Stapells, DR. Principles and Apllications of Cortical Auditory Evoked potentials. In: Bukard FB, Don M, Eggermont J J Auditory Evoked Potentials - Basic Principles and Clinical Application. Philadelphia: Lippincott Williams & Wilkins; 2007.
24. Cranford JL, Martin R. Age related changes in binaural processing I evoked potential findings. Am J of Otology 1991, 12: 357-64.
25. Franco G M. Potencial evocado cognitivo em adultos normais. Arq Neuropsiquiatr 2001, 59(2-A): 198-200.
26. Goodin DS, Squires KC, Starr A. Long latency event-related components of the auditory evoked potential in dementia. Brain. 1978 Dec;101(4):635-48.
1. ENT expert (ENT doctor at HUSM - UFSM)
2. Master degree doctor in Human Communication Disorder by UFSM (Speech doctor at ENT Clinic Cóser)
3. PhD in Medicine by UFRGS (Professor of Pediatrics and Neurology at UFSM)
4. PhD in Human Communication Disorder by UNIFESP (Professor of ENT at UFSM).
Institution: Universidade Federal de Santa Maria-RS - Federal University - Santa Maria - RS - Brazil.
Maria José Santos Cóser
Mail Address: Rua Duque de Caxias, 1668/304 - Centro - Santa Maria/RS - CEP: 97015-190. Phone/fax: (55)3221.9784. E-mail: mariajosecoser@terra.com.br
This article was submitted to SGP (Sistema de Gestão de Publicações - Publication Management system) of R@IO on October 2nd, 2007 and approved on November 4th, 2007 at 22:07:13.