INTRODUCTIONThe acoustic analysis began to be more often used in Brazil and in the phonoaudiologic clinical in the last decade and is aimed at quantifying and characterizing the sound signal. In addition, by means of objective evaluation it's possible to create normative databases of populations, detect vocal problems early and monitor the phonoaudiologic treatment efficiency. The data found by means of acoustic analysis are complementary to the auditory perception analysis, which remain sovereign, in case there are conflicts between the perceptive and acoustic data (1,2).
At the same time, the correlation between these two evaluations and the laryngoscopic evaluation, whose main objective is to amplify the image, enabling the evaluation of the presence of slight lesions, may amplify the range of diagnostic and therapeutic possibilities (3). Besides the sound signal objectification, the acoustic analysis allows the evaluator to capture early vocal changes and it's a great resource for promotion and prevention of the vocal health (4,5).
The acoustic analysis offers sound wave format, analysis of fundamental frequency, (f0), defined as the number of vibrations per second produced by the vocal cords, frequency disturbance measurements, such as: jitter; defined as the cycle by cycle frequency disturbance; amplitude disturbance measurements; shimmer, which is the cycle by cycle amplitude variability and the noise measurements such as NHR that correlates the harmonic component with the noise component (1,2,5,6,7,8).
The auditory perception evaluation is frequently carried out in the clinical praxis of the phonoaudiologist and is impressionist, as for the individual's vocal quality.
Then, it depends on the experience of the professional who will compare his/her findings with others performed afterwards by the same evaluator (9).
To produce a sound a sound source is primarily necessary, that is, a system in course and an energy source able to displace the sound source from resting by means of the air. Phonation uses portions of the respiratory and digestive tracts, and causes modifications to the expiratory air flow passage. The first modification occurs in the larynx and after in the oral or nasal resonance cavities (10,11). Acoustically, the modifications arising out of the variations in the resonant tract are known as filter action, described by Fant, 1970 (12). The vocal tract acts as a filter and its resonance frequencies are referred to as formants. The vowels are recognized by their formants, which are produced by articulating mechanisms and modified by the specific adjustments of the vocal tract (13).
In the national literature, the number of works that perform the extraction of normative acoustic data of the Brazilian Portuguese vowels formants in women without vocal complaints is low. Moreover, the existing researches describe reduced samples of individuals and the use of different computerized programs (7,14,15,16,17,18,19).
Aiming at helping in the creation of a normative database for future works in the acoustic analysis area in Brazil, the objective of this research was to make an extraction of oral vowels formants frequency values of the Brazilian Portuguese spoken in the city of São Paulo and of the sound signal disturbance measurements in non-smoker, non-alcoholic women without vocal complaints.
METHODThis research was carried out after approval of the Ethics Committee of the Cancer Institute Arnaldo Vieira de Carvalho (ICAVC) under the number 073/04.
The individuals in this work were selected in several action of Health Promotion and Prevention, performed by the Valentim Institute, by means of an itinerant bus that went through some cities of the State of São Paulo, between the months of April and July, 2006, in a total of a hundred and seven individuals of the female sex (average=44 years).
In order to compose a sample of this work all individuals should meet the following inclusion criteria: female sex, older than 18 years of age, non-smoker, non-alcoholic and with normal laryngological exam, that is, without malign or benign mass lesion. It was not a purpose of the work to detect the presence of slits, then this datum was not taken into account in the laryngological evaluation. The exclusion factors were women with vocal complaints and who had undergone any larynx surgery or that were not included in abovementioned inclusion criteria.
Therefore, the first step of this selection consisted of the laryngological evaluation through the direct laryngoscopy to check for the presence or not of larynx benign or malign lesions, carried out with local anesthesia (2% of intraoral lidocaine) and with KAY Elemetrics laryngoscope, Model RLS9100B, with KAY Elemetrics telescope, model 9106 and Panasonic micro-camera, model GPUS522. All women with suspicion of malign lesion were forwarded to the Head and Neck Surgery Department of the Cancer Institute Arnaldo Vieira de Carvalho (ICAVC). The women who presented with benign lesions received instructions about vocal hygiene by means of a manual prepared by the Phonoaudiology Service of ICAVC and were oriented to look for phonoaudiologic treatment.
The women without alterations in the laryngoscopy got to the next step of the work consisting of phonoaudiologic anamnesis, containing identification data, use of tobacco or alcohol, gastro-esophageal reflux, medications, surgeries or complaints concerning the voice. All women signed an informed consent term. After elimination of the use of tobacco, alcohol and vocal complaints, they were forwarded to the front part of the bus, adapted for the performance of the acoustic recordings. The voice recording was made directly into the computer and analyzed by the CSL 4300B and Multi-Dimensional Voice Program (MDVP), Kay Elemetrics (Lincoln Park, NL).
The signal was captured by an unidirectional microphone, positioned on a support at 15 cm from the mouth of each woman, who remained standing and were prompted to count the numbers from 1 to 10, emission of vowel /a/, for measuring the vocal parameters and then emission of the seven vowels /a/, /e/,/é/,/i/,/o/,/ó/,/u/ always with a deep breath and keeping the usual pattern of the speech pitch and loudness. The studied acoustic measures were: fundamental frequency (f0), frequency of the three first formants of the seven vowels of the Brazilian Portuguese, jitter, shimmer, APQ (Amplitude Perturbation Quotient), PPQ (Period Perturbation Quotient), NHR (Noise Harmonic Ratio).
Voice auditory perception evaluation was also made by means of the Girbas scale (20) by an experienced phonoaudiologist in the vocal evaluation, and G corresponds to the global level of vocal alteration, I (instability), R (roughness), B (breathness), A (asteny), S (strain) and a numeric scale from 0 (absent/normal), 1 (discreet), and 3 (intense alteration).
For the results analysis, initially the average variation was verified for each vocal parameter concerning the age. This variation behavior enabled to divide the ages in age groups, because the parameters presented a constant tendency. Then, three age groups were created, namely, Group 1, women over the ages between 18 and 39 years (n = 46), Group 2, between 40 and 60 years (n = 47) and Group 3, between 61 and 86 years (n = 14), the age of the oldest participant. Later the sample frequency distribution normality was verified for different parameters and considering this condition the Test T, Student was applied for averages comparison. The Test T was applied with significance of 5% to compare the variables average concerning the three distinct age groups, and T < TC.
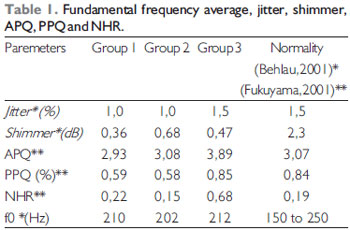
RESULTSThe results were divided into three age groups. Group 1 was formed by women with age ranges between 18 and 39 years, Group 2, women between 40 and 60 years and Group 3, women between 61 and 86 years old. The fundamental frequency averages results, jitter, shimmer, APQ, PPQ and NHR for the female gender are described in Table 1. In the results table the normality values were entered according to Behlau, 2001 (1) and Fukuyama, 2001 (21).
The jitter values were similar for Groups 1 and 2 and there was an increase of 0.5% for Group 3. The values found for the three age ranges are within the normality range which is of 1.5% (1). The difference in the results is not expressive for the significance level of 5%.
A different datum to shimmer, that presented its highest value in Group 2 compared to Groups 1 and 3. The values found are below the normality value which is of 2.3 dB (1). The shimmer values didn't either present significant difference for the significance level of 5%.
There was an increase of the APQ values as the ages increased. The values found in Groups 1 and 2 are within the normality values which are below 3.07 (21), but Group 3 is out of this pattern. The difference in the APQ results is not expressive for the significance level of 5%.
For fundamental and NHR frequency parameters, there was a decrease in Group 2 values when compared to Group 1, but a great increase compared to Group 3; however, the statistical analysis showed the difference between these results is not expressive for significance level of 5%. The values found for the age groups fundamental frequency are within the normality range that varies from 150 Hz to 250 Hz (1). For NHR only Group 2 was within the normality range, which is below 0.19 (21). Very similar PPQ values were also found in Group 1 and 2, with an increase to the value in Group 3. There was no significant difference in the level of significance of 5% for the PPQ parameter. Groups 1, 2 and 3 were within normality range which is below 0.84% (21).
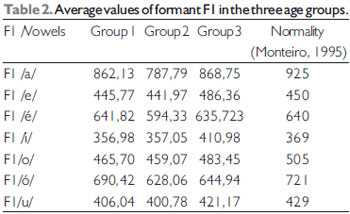
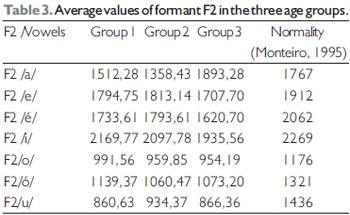
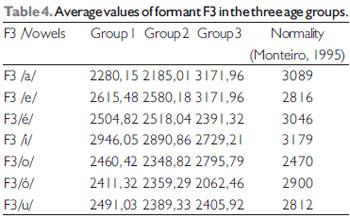
The average of formants F1, F2 and F3 of the seven vowels of the Brazilian Portuguese /a/,/e/, /é/, /i/, /o/, /ó/,/u/ are described in Table 2, Table 3 and Table 4, respectively, as well as the normality reference values based on the research by Monteiro, 1995 (17).
The individuals included in Group 3 obtained higher F1 values for vowels /a/,/e/,/i/,/o/,/u/, compared to Groups 1 and 2. Only in vowels /é/,/ó/ the values were higher for individuals of Group 1. the results of formants demonstrated there was a fall in the values of formants in Group 2, compared to Group 1 and then there was an elevation in the values of Group 3 for all vowels. There was a significant difference in formant F1 for vowels /e/, /i/ between Groups 1 and 3 and Groups 2 and 3. For vowels /é/,/ó/ the significant difference remained between Groups 1 and 2. The F1 values average of the seven vowels in the three age groups were within the normality range.
The behavior of values F2 was very diversified. This formant frequencies of vowels /i/, /o/, /u/ were higher for group 1. Group 2 had higher values for vowels /e/,/é/,/u/ compared to the other groups. The F2 for vowel /a/ was increased in Group 3. There was a significant statistical difference between Groups 1 and 2 and between Groups 1 and 3 only for vowel /ó/. The seven vowels averages for F2 were decreased compared to the normality range found for this second formant.
For vowels /a/,/e/,/o/,/u/ there is a fall in the values of F3 for Group 2, compared to Group 1 and then an elevation in Group 3. The opposite occurs with vowel /é/, which has an elevation in Group 2 and then a fall in Group 3, In vowels /i/,/ó/ there are consecutive falls for Groups 2 and 3, compared to Group 1. The difference was significant between Groups 1 and 3 for vowels /e/,/i/ and between Groups 2 and 3 for vowel /i/. For F3 all the averages of the vowels in the three age groups are diminished as for the normality.
We observed most people presented as vocal impression (G) global level, score 1, that characterizes a discreet impact on the vocal quality. The voice features: Instability (I), roughness (R) and strain (S) obtained scores between 0 and 1, that is, no alteration found or discreet alteration. As for breathness (B) and asteny (A), these were respectively not much found or void in this population studied.
The Vocal Impression Global Level index (GO for Group 1 was of 13 individuals (28.26%) who presented score 0, followed of 29 (63.04%) of scores 1 and 4 (8.69%) score 2. Instability (I) obtained 23 (50%) individuals with score 0, 21 (45.65%) with scores 1 and 2 (4.34%) with score 2. Roughness (R) obtained 32 (69.56%) with score 0, 9 (19.56%) with score 1 and 5 (10.86%) with score 2. Breathness (B) presented with 41 (89.13%) of score 0, 3 (6.52%) with score 1 and only 2 (4.34%) with level 2. For the parameter Asteny (A) the index was void and finally for Strain (S) there were 35 (76%) individuals with score 0, 9 (19.56%) with score 1 and 2 (4.34%) with level 2.
For Group 2, the Vocal Impression Global (G) Level index was of 15 (31.91%) individuals who presented the score 0, 28 (59.57%) score 1 and 4 (8.51%) score 2. Instability (I) obtained 19 (40.42%) individuals with score 0, 24 (51.06%) with score 1 and 4 (8.51%) with score 2. Roughness (R) obtained 25 (53.19%) with score 0, 16 (34%) with score 1 and 6 (12.76%) with score 2. Breathness (B) presented 45 (95.74%) with score 0, 2 (4.25%) with score 1 and no individual with score 2. For the parameter Asteny (A) the index was void and finally for Strain (S) there were 27 (57.44%) individuals with score 0, 16 (34%) with score 1 and 4 (8.51%) with level 2.
For Group 3, the Vocal Impression Global (G) Level index was of 3 (21.42%) individuals who presented the score 0, 6 (42.85%) score 1 and 5 (35.71%) score 2. Instability (I) obtained 5 (35.71%) individuals with score 0, 5 (35.71%) with score 1 and 4 (28.57%) with score 2. Roughness (R) obtained 7 (50%) with score 0, 3 (14.28%) with score 1 and 5 (35.71%) with score 2. Breathness (B) presented 13 (92.85%) with score 0, 1 (7.14%) with score 1 and no individual with score 2. For the parameter Asteny (A) the index was void and finally for Strain (S) there were 9 (64.28%) individuals with score 0, 3 (21.42%) with score 1 and 2 (14.28%) with level 2.
DISCUSSIONThe vocal evaluation, by means of acoustic analysis, helps the phonoaudiologist in the performance of an objective evaluation of the voice also in the creation of databases that identify the specific features of vocal disorders or patterns of normality, but these are still uncommon in the national researches (1).
The results obtained in this work concerning the fundamental frequency (f0) ranged from 202 Hz to 212 Hz. This datum was similar to the findings obtained by several authors (8,14,22) who found values between 204Hz and 206Hz for women without vocal complaint. Other works presented with higher values of f0 between 219 Hz and 235 Hz (5,19) for the group of women without complaints. There was a slight increase of f0 values between Groups 1 and 2 when compared to Group 3. This finding does not match the literature that states there is a decrease of values of f0 with the aging, probably due to the reduced size of the sample (23,24).
As for the jitter value, which is the variability of the f0 at short term, there is an increase in its values as there is a lack of control in the mass emission and increase. In the other hand, such parameter may be trained, as in the case of lyrical singers, who present with a higher control of their emission and consequently a less noisy vocal quality. Such parameter correlates to the roughness and age increase (8). This study found values between 1.0 to 1.5% for the women analyzed, that are equivalent to the study performed by other author (14) which was of 1.5%. Other works present lower values, that range from 0.2% to 0.62% (7,8,19,23,25). A higher value than 3.1% was found by another author (22). There was an increase of 0.5% for group 3 compared to groups 1 and 2, confirming there occurred an increase of the jitter value concerning age, since it matched the findings of the literature (1,24).
The shimmer value represents the sound wave amplitude variability, describes the phonatory stability and its increased values reflect a higher noise in the emission, breathed voices and may suggest the presence of mass lesions (5). In this study there was a variation in the values between 0.36 to 0.68 dB. This finding got closer to the work performed by another research (8) that found a value of 0.22dB for this parameter. The other researches presented much higher values that ranged from 1.4dB to 37.2dB (7,14,19,22,25). The shimmer vocal parameter showed an increase in the course of aging and this fact matches the literature, since the shimmer undergoes interference with the age increase (1).
The other fundamental frequency perturbation measure, PPQ (%), is an index that appoints the sound source amplitude periodicity variation and also correlates with the phonatory system control. This parameter was also the highest one for Group 3, as Groups 1 and 2 presented their values within the normality range. As from this data, it's possible to presume that with the age increase there may be less fine control of the laryngeal musculature movement, due to a reduction of the tonus, and muscular mass loss and then increasing in the vibration variability between the PPVV at each phonatory cycle (26).
As for the APQ, that is an amplitude variation measure, this study found the values that ranged from 2.93 to 3.89. Because it's a perturbation measure, its value represents the phonatory stability level and depends on the phonatory system control. The lower the phonatory control, the higher will its value be. Group 3 presented its values out of the normality range. This data may be explained by the fact people at this age range do not have an adequate vocal control, and present with trembling and instability in the emission. The increased value may even be justified by the hormonal phase which the women go through and the vocal quality of the menopause characterized by roughness and asperity presents an inherent relation with the APQ and NHR (24).
The noise measure, NHR, ranged from 0.15 to 0.68. The noise is not a periodical sound and represents the vibration movement created in the vocal cords that don't find a relation between themselves. A dysphonic voice presents high levels of noise in the spectrogram, because of the unevenness of the vocal cords coaptation (1). The individuals comprised in Group 3 were the ones who obtained the highest value in this parameter, which suggests with an age increase there is reduction of the pulmonary capacity, vocal edema due to hormonal falls and decrease of the vocal cords vascularization (26).
Fukuyama, 2001 (21) found the values of 2.10 (APQ), 0.30 (PPQ) and 0.12 (NHR) with the MDVP program in 25 Brazilian women without vocal complaints. Such parameters were difficult to find in the national literature. In the international literature we found values of APQ for women with NHR of 1.75 and 0.12 and APQ of 1.7 (27).
The difference between the results of this work and those found in the literature concerning the f0, jitter, shimmer, APQ, PPQ and NHR values may concern the several existing programs for data extraction, recording means, microphone position, environmental noise and also for cultural factors that alter the pattern of voice intensity and frequency (1,2,8).
The vowels are identified by their formants that, in turn, are acoustic resonances of the vocal tract. The vowels formants range depending on anatomofunctional features of each individual and the position of the phonoarticulatory organs upon emission (28). The three first formants of each vowel are more representative concerning the acoustic description of the vowels (13). The first formant, named F1, depends of the opening of the jaw, lowering of the tongue, vertical displacement of the tongue and laryngeal constriction. F2 relies on the horizontal movement of the tongue and F3 on the size of the oral cavity (1).
The researches carried out by Behlau 1984 (14) and Monteiro (1995) (17) present works with the formants average values for Brazilian women. The researches were accomplished with a limited number of individuals and different acoustic analysis programs, and the Behlau study was made with a sound spectrograph V.I. 700 and with 30 individuals of the feminine sex and Monteiro used a Soundscope program, by GW Instruments and with 20 female sex individuals. The values found by the researchers are within the values found in this study, which was made with the CSL program.
In this study, for F1, all vowels of Group 2 had their values diminished compared with Group 1. When we compared Group 1 with Group3, except for the vowels /é/,/ó/, the Group 3 values were higher, more acute than in Group 1. This means the formant F1 result shows there's a fall in the values as from 40 years and then there is an elevation of values after the 60 years. The first formant, F1, depends on the opening of the jaw and the values increase of the formants from the 60 years may be justified as resulting from mass loss and fat which may characterize a lower volume of osseous and dental intra-oral mass, as well as diminishing of the face inferior third vertical dimension (29).
The formant F2 described higher values in the youngest population, groups 1 and 2. F2 is related to the tongue movement in the horizontal direction, depends on the fine and precise control of the tongue, with hypotrophy, reduction of the tonus that occurs with age, this may somehow be interfered with the difference between the younger groups and Group 3.
Formant F3 represents individualized aspects of the vocal tract of each speaker and the smaller the oral cavity, the higher its value will be, in the other hand, the larger the size of the oral cavity, the lower the value of the formant. There was an increase in the values of almost all vowels /a/,/e/,/o/,/u/ for Group 3 when compared to Groups 1 and 2. The F3 increase from the 60 years may also be justified as a result of osseous and dental losses and flaccidity in the tongue musculature which increase the size of the oral cavity (30).
The Girbas scale was chosen, because it offers the advantage of simple application, in addition to be widely used in the clinical practice (9).
All the age groups had the largest part of their individuals with score 0, followed of score 1 and a few presented with score 2. The analysis was carried out with non-smoker, non-alcoholic women without vocal complaints, so that slight levels for roughness, strain and instability were already expected.
Raucousness is related with mass lesions that consequently alter the vocal cords vibration evenness. It may start from the consumption of tobacco, alcohol and to hormonal alterations. The strain, that occurs in the glottis compression, is related to hyperkinetic dysphonia and may be a trace of muscle-skeletal tension syndrome. The phonation instability may indicate a lack of vocal control, emotional alterations and, in more severe cases, neurological diseases (1).
The presence of breathness in some women may be justified by the presence of the posterior triangular slit, which is frequent in women, but in this study, we made no correlation between laryngological findings and vocal analysis, because, for it addressed a vocal sorting, the laryngological exam only considered alteration upon the presence of benign or malign lesion. Therefore, there wasn't the detailing of the presence or not of triangular slits in these women. Asteny was not expected since it's normally found in neurological lesions, muscle weakness and vocal power loss (1).
The results obtained in the auditory perception evaluation demonstrated there is a great variability in normal voices as a result of the great interpersonal difference.
CONCLUSIONThe research accomplished for extraction of the formants frequency values of the Brazilian Portuguese spoken in São Paulo and the sound signal perturbation measures in non-smoker, non-alcoholic women without vocal complaints showed it's necessary to create normative data, since the works performed with this purpose presented a reduced number of individuals and with a variability among the programs used for the values extraction.
The fundamental frequencies (f0) were compatible with the values found in the literature. The jitter, shimmer, APQ, PPQ and NHR measures were compatible with the existing literature, but they also found a discrepancy concerning some articles researched, and we concluded these parameters are submitted to the difference in the data extraction and age. The auditory perception analysis findings show the values are within the normality patterns for normal voices.
The data found in formants F1, F2 and F3 were difficult to be justified in the literature, since the correlation between the formants and the age is not a finding with enough studies.
Therefore, the acoustic analysis, auditory perception and laryngological analyses present an agreement among their findings and prove to be very important for the normality researches. We should remark there is a great variability among normal voices, since the voice is the representation of individual characteristics.
BIBLIOGRAPHICAL REFERENCES1. Behlau, M. Voz do Especialista-Vol 1. Rio de Janeiro: Revinter; 2001.
2. Araújo SA, Grellet M, Pereira JC, Rosa MO. Normatização de medidas acústicas da voz normal. Rev Bras Otorrinolaringol. 2002, 68:540-44.
3. Nemr K, Amar A, Abrahão M, Leite GCA, Kohler J, Santos AO, Correa LAC. Análise comparativa entre avaliação fonoaudiológica perceptivo-auditiva, análise acústica e laringoscopias indiretas para avaliação vocal em população com queixa vocal. Revista Rev Bras Otorrinolaringol. 2005, 71:113-7.
4. Corazza VR, Silva VFC, Queija D, Dedivits RA, Barros APB. Correlação entre os achados estroboscópicos, perceptivo-auditivos e acústicos em adultos sem queixa vocal. Rev Bras Otorrinolaringol. 2004, 70:30-4.
5. Pontes PAL, Vieira VP, Gonçalves MIR, Pontes AAL. Características das vozes roucas, ásperas e normais: análise acústica espectrográfica comparativa. Rev Bras Otorrinolaringol. 2002, 68:182-84.
6. Behlau M. Considerações sobre a análise acústica em laboratórios computadorizados de voz. In: Araujo B. Fonoaudiologia Atual. São Paulo: Revinter; 1997, 93-115.
7. Gama ACC. Análise acústica de voz: estudo comparativo entre mulheres sem queixa vocal e com disfonia. São Paulo, 1997 (Tese de Mestrado - Universidade Federal de São Paulo).
8. Felippe ACN, Grillo MHMM, Grechi TH. Normatização de medidas acústicas para vozes normais. Rev Bras Otorrinolaringol. 1997, 72:659-664.
9. Bodt MS, Wuyts F, Van de Hening PH, Croux C. Test - retest study of the GRBAS scale: influence of experience and Professional background on perceptual rating of voice quality. Jornal of Voice. 1997, 1:74-80.
10. Russo I, Behlau M. Percepção da fala: Análise acústica do português brasileiro.São Paulo: Lovise, 1993.
11. Dedivitis RA, Barros, APB. Fisiologia laríngea. In: Dedivits RA, Barros, APB. Métodos de avaliação e diagnóstico de laringe e voz. São Paulo: Ed. Lovise; 2002, p. 39-52.
12. Fant G. Acoustic theory of speech production. 2nd ed. Paris, Mounton, 1970.
13. Camargo Z. Avaliação Objetiva da Voz. In: Carrara-Angelis E, Furia LB, Mourão LF,Kowalski LP.A atuação da Fonoaudiologia no câncer de cabeça e pescoço. São Paulo: Lovise; 2000, 175-92.
14. Behlau M. Uma análise das vogais do português brasileiro falado em São Paulo: perceptual, espectrográfica de formantes e computadorizada da freqüência fundamental. São Paulo, 1984 (Tese de Mestrado - Escola Paulista de Medicina).
15. Carrara E. Análise comparativa da configuração laríngea perceptual auditiva e espectrográfica acústica da qualidade vocal pré e pós-emissão vocal em registro basal. São Paulo, 1991 (Monografia de Especialização - Escola Paulista de Medicina).
16. Rodrigues S. Proporção harmônico-ruído: valores para indivíduos adultos brasileiros. São Paulo, 1993 (Monografia de Especialização - Escola Paulista de Medicina).
17. Monteiro MC. Uma análise computadorizada espectrográfica dos formantes das vogais orais do português brasileiro falado em São Paulo. São Paulo, 1995 (Monografia de Especialização - Universidade Federal de São Paulo).
18. Rodrigues S. Análise múltipla do efeito da técnica de vibração de língua. São Paulo, 1996 (Tese de Mestrado - Escola Paulista de Medicina).
19. Tosi D. Índice de perturbação da freqüência fundamental a curto e a longo prazo em mulheres sem alteração vocal. São Paulo, 1999 (Monografia de Especialização - Centro de Estudos da Voz).
20. Dejonckere PH, Remacle M, Fresnel-Elbaz E, Woisard V, Crevier-Buchman L, Millter B. Differentiated perceptual evaluation of pathological voice quality: reliability and correlations with acoustic measurements. Rev Laryngol Otol Rhinol. 1996, 17:219-24.
21. Fukuyama EE. Análise acústica da voz captada na faringe próximo ä fonte glótica através de microfone acoplado ao fibrolaringoscópio. Rev Bras Otorrinolaringol. 2001, 67:776-86.
22. Behlau M, Tosi O, Pontes PAL. Determinação da freqüência fundamental e suas variações em altura ("Jitter") e intensidade ("Shimmer"), para falantes do português brasileiro. Acta AWHO. 1985, 4:5-9.
23. Ferrand CT. Harmonics-to- noise ratio: an index of vocal aging. Journal of Voice. 2002, 16:480-87.
24. Gorham-Rowan M, Laures - Gores. Acoustic - perceptual correlates of voice quality in elderly men and women. J Commun Disord. 2006, 39:171-184.
25. Figueiredo DC, Souza PRF, Gonçalves MIR, Biase, NG. Análise perceptivo-auditiva, acústica computadorizada e laringológica da voz de adultos jovens fumantes e não fumantes. Rev Bras Otorrinolaringol. 2003, 69:791-99.
26. Mifune E, Justino V, Camargo Z, Gregio F. Análise Acústica da Voz do Idoso: Caracterização da Freqüência Fundamental. Rev CEFAC. 2007, 9:238-47.
27. Nicastrini M, et al. Multidimensional voice program (MDVP) and amplitude variation parameters in euphonic adult subjetcs. Normative Study. Acta Otorhinolaryngol Ital. 2004, 24:337-41.
28. Behlau M, Pontes PAL, Ganança, MM, Tosi O. Análise espectrográfica de formantes das vogais do português brasileiro. Acta AWHO. 1988, 7:67-73.
29. Dervis E. Changes in temporomandibular disorders after treatment with new complete dentures. J Oral Rehabil. 2004, 31:320-26.
30. Fazito LT, Perim JV, Di Ninno CQMS. Comparação das queixas alimentares de idosos com e sem prótese dentária. Rev CEFAC. 2004, 6:143-50.
1. Doctoral Degree in Sciences at the Medicine College of the University of São Paulo. Coordinator Professor of the Phonoaudiology Service of ICAVC and of the Course of Voice Specialization of the Cancer Institute Arnaldo Vieira de Carvalho.
2.Voice and Dysphagy Specialist at the Cancer Institute Arnaldo Vieira de Carvalho. Coordinator of the Phonoaudiology Department of the Oncologic Center of Mogi das Cruzes / SP.
Institution: Instituto do Câncer Arnaldo Vieira de Carvalho. São Paulo / SP - Brazil
Mail address:
Instituto do Câncer Arnaldo Vieira de Carvalho / Setor de Fonoaudiologia
Largo do Arouche, 66 - República
São Paulo / SP - Brazil - Zip code: 01219-010
Phone: (+55 11) 3367-3844
Article received on December 17, 2008.
Approved on December 18, 2008.