INTRODUCTIONCharacteristic facial features, congenital cardiac anomalies, cleft palate and learning disabilities, are all major characteristics of the velocardiofacial syndrome, described in some patients by Sedláckova(1) and outlined by Shprintzen et al (2). New phenotypic alterations of this syndrome have been described in the meantime (3-5). Although considered as one of the most frequent syndromes associated with cleft palate (6), it is not frequently recognized in the pediatrics practice. It's caused by delection of the long arm of the chromosome 22 (22q11).
Recently, middle and inner ear malformations have been described in VCFS. Patients with hearing loss associated with otitis media and with external ear malformations are described (7-8). The first reference to a primary defect of the ossicular chain was made in 2003, in a child with signs of the VCFS and 22q11.2 delection (9), from whom was found primary lung disgenesia along with congenital conductive unilateral hearing loss, due to malformation and subluxation of the left stapes, therefore, a conductive hearing loss not related to otitis media, which is very common in this syndrome. Middle and inner ear malformations were foud in two children with VCFS. One of them showed a Mondini type cochlear malformation, an abnormal shape of the ossicles, with fusion of the malleus with the incus and a monopodal stapes. The other child showed a congenital middle ear malformation with fixation of the malleus on the left annulus tympanicus, and a common cavity bilaterally between the vestibule and the lateral semicircular canal (10).
This article aims at describing and characterizing the middle and inner ear malformations found in two Brazilian boys with the VCFS.
METHODThis paper was approved by Comitê de Ética em Pesquisa da PUCSP, protocol nº 261/2008.
Subjects: Two boys with clinical signs of VCFS, at the ages of 4.7 and 6.7 years old.
Procedures: Audiological evaluation, including pure tone audiometry, timpanometry, acoustical reflex, and Computerized Tomography (CT) of temporal bones. In both, analyses of DNA sample with markers of 22q11 region were performed. A Toshiba Aquilion-slice thickness 0.6mm tomograph, an Interacoustics AC33 audiometer, and an Interacoustics AZ-7 middle ear analyser were used.
RESULTSPatient 1 is a boy at the age of 6.7 years old, son of nonconsanguineous parents. He was born by cesarean, after a 41-week pregnancy. No family antecedents. He showed a submucous cleft palate, which was operated when he was 2.6 years, with good functional result. The neuropsychomotor development was normal. He shows clinical signs of VCFS, without cardiac defects. The DNA sample analyses from the patient and his parents, with five markers, revealed the delection of, at least, one marker in the 22q11.2 region, which confirms the VCFS diagnosis.
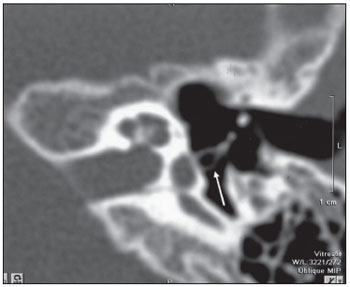
The audiogram shows air tone thresholds of 15dB HL at 250, 500, 1000 Hz, 20dB HL at 2000 and 4000Hz and 25dB HL, 60dB HL and 70dB HL (respectively at 4000, 6000 and 8000 Hz) in the right side. Air tone thresholds of 15dB HL at 250 and 500 Hz, 20 dB HL at 1000 and 2000 Hz, 25dB HL at 4000 Hz and 40dB HL at 6000 and 8000 Hz in the left side. Bone tone thresholds of 5dB HL at 500 e 1000 Hz, 0dB HL at 1000 Hz and 10 dB HL at 2000 and 4000 Hz. SRT was 35 dB HL in the right and 30 dB HL in the left. WRS was of 100% at 60 dB bilaterally. Timpanometry was of type B and the acoustical reflex was absent bilaterally. The CT of temporal bones shows signs of bilateral inflammatory otomastoidopathy, a common cavity between the vestibule and the lateral semicircular canal on the right side and an assimetry of the lateral semicircular canal on the left (Picture 1). Ossicles had a normal configuration.
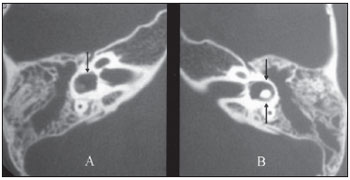
Picture 1. Patient 1: CT showing bilateral inflammatory otomastoidopathy and a common cavity between the vestibule and the lateral semicircular canal at right(arrow inA). Assimetry of the lateral semicircular canal at left ( arrows in B).
Patient 2 is a 4.6 year-old boy, son of non consanguineous parents. He has a third degree cousin from his mother branch, which bears a cleft palate. Born by cesarean he developed respiratory infection, hyperbilirubinemia and hypoglycemia in his 4th day of life, treated for 10 days.
He had a minor delay in his motor development and a heart murmur dysfunction that was monitored by a cardiologist. He had a delay in language development and, currently, shows a hypernasal voice and compensatory articulation errors. The oral examination shows a hypoplastic uvula, a short palate with reduced elevation movements. He has clinical signs of the VCFS. The analyses of DNA samples from him and his parents revealed that the patient shows delection in, at least, four markers in the region 22q11.2, which confirms the VCFS diagnosis.
The audiological evaluation shows a conductive hearing loss, with air thresholds around 40 to 50dB HL on the right side and 25 to 30dB HL on the left, with normal bone thresholds, between 0 and 10 dB HL bilaterally. SRT was of 50dB HL on the right side and 30 dB HL on the left side. Tympanometry curve type A and absence of acoustical reflex bilaterally.
CT of temporal bones shows a bilateral displasia of the lateral semicircular canals, which are shorter in comparison with the posterior and superior semicircular canals, globosity of vestibules (Picture 2 and 3) and mild pericochlear radiolucent foci (Picture 4). Deformity of the stapes was found at the left side, characterized as a kinking of the posterior crus (Picture 5). This finding was only detected after an oblique reformation parallel to the stapes (about 30o to 45o).
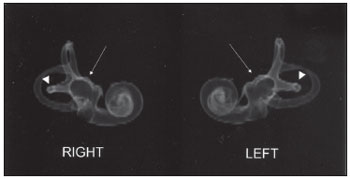
Picture 2. Patient 2: 3-D images from the osseous labyrinth based on CT showing bilateral displasia of the lateral semicircular canal ( arrowheads ) and globosity of the vestibules ( arrows).
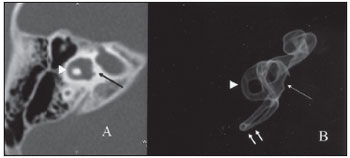
Picture 3. Patient 2: Axial and 3-D reconstruction showing displasia of the lateral semicircular canal (arrowheads in A and B) in comparison with the posterior semicircular canal (double small arrows in B) and globosity of the vestibule (long arrows in A and B).
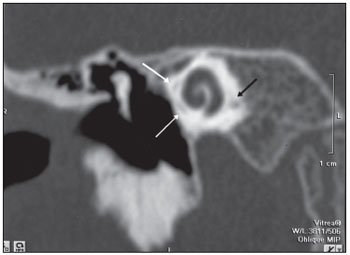
Picture 4. Patient 2: Mild pericochlear radiolucent foci (arrows) in CT coronal view.
Picture 5. Patient 2: Oblique CT reformation with evidence of deformity of the posterior crus of the left stapes (arrow).
Hearing loss is a very frequent symptom in VCFS and in most instances is related to chronic or recurrent middle ear infections. Our findings, which have already been described by others, shows that there can be also middle and inner ear malformations, along with malformations of vestibule and semicircular canal. On the other hand these primary middle and inner ear malformations in VCFS leads to the studies about the role of the genes TBX1, in the morphogenesis of middle and inner ear (11). From the clinical point of view, we consider it to be highly important to carry out a thorough evaluation and the monitoring of the hearing evolution, as well as the occurrence of symptoms related to the vestibular function, already described in children with the VCFS (12). Further studies are necessary to establish whether this is a consistent morphological trait in VCFS. From the radiological point of view, oblique reformations with zoom parallel to the stapes are very helpful in detecting mild deformities or incomplete crus. Sometimes the routine axial images do not show completely the stapes and reformations based on multislice acquisitions are of high quality. Regarding the labyrinth, a three-dimensional reconstruction is an interesting tool for a global analysis.
BIBLIOGRAPHICAL REFERENCES1. Sedlácková E. The syndrome of congenital shortened velum and dual innervation of the soft palate. Folia Phoniatr (Basel). 1967, 19:441-3.
2. Shprintzen RJ, Goldberg RB, Lewin ML, Sidoti, EJ, Berkman MD, Argamaso RV, et al. A new syndrome involving cleft palate, cardiac anomalies, typical facies, and learning disabilities: velo-cardio-facial syndrome. Cleft Palate J. 1978, 15:56-62.
3. Beemer FA, Nef JJEM, Delleman JW, Shprintzen RJ. Addicional eye findings in a girl with the velo-cardio-facial syndrome [letter]. Am J Med Genet. 1986, 24:541-2.
4. Mackenzie-Stepner K, Witzel MA, Stringer DA, Lindsay WK, Munro IR. Abnormal carotid arteries in the velocardiofacial syndrome: a report of three cases. Plast Reconstr Surg. 1987, 80:347-51.
5. Tabith Jr A, Genaro KF, Trindade AS. Velocardiofacial syndrome with facia and pinna asymetries. Braz J Med Biol Res. 1996, 29:1445-7.
6. Shprintzen RJ, Siegel-Sadewitz VL, Amato J, Goldberg RB. Retrospective diagnoses of previously missed syndromic disorders among 1000 patients with cleft lip, cleft palate, or both. Cleft Palate J. 1985, 21:85-92.
7. Reyes MR, LeBlanc EM, Bassila MK. Hearing loss and otitis media in velo-cardio-facial syndrome. Int J Pediatr Otorhinolaryngol. 1999, 47:227-33.
8. Ford LC, Sulprizio SL, Rasgon BM. Otolaryngological manifestations of velocardiofacial syndrome: a retrospective review of 35 patients. Laryngoscope. 2000, 110(3 Pt 1):362-7.
9. Cunningham ML, Perry RJ, Eby PR, Gibson RL, Ophein KE, Manning SC. Primary pulmonary dysgenesis in velocardiofacial syndrome: a second patient [letter]. Am J Med Genet. 2003, 121A:177-9.
10. Devriendt K, Swillen A, Schatteman I, Lemmerling M, Dhooge I. Middle and inner ear malformations in velocardiofacial syndrome [letter]. Am J Med Genet. 2004, 131A:225-6.
11. Vitelli F, Viola A, Morishima M, Pramparo T, Baldini A, Lindsay E. TBX1 is required for inner ear morphogenesis. Hum Mol Genet. 2003, 12:2041-8
12. Swillen A, Devriendt K, Legius E, Prinzie P, Vogels A, Ghesquiere P, et al. The Behavioural phenotype in velo-cardio-facial syndrome (VCFS): from infancy to adolescence. Genet Couns. 1999, 10:79-88.
1. Master's degree. General Director DERDIC_PUCSP.
2. Doctoral Degree. Radiologist - Imaging Doctor - Hospital Beneficência Portuguesa de São Paulo.
3. Graduation in Medicine. Otorhinolaryngologist - Phoniatrist at DERDIC/PUCSP.
4. University Diploma in Phonoaudiology. Phonoaudiologist at DERDIC/PUCSP.
Institution: Divisão de Educação e Reabilitação dos Distúrbios da Comunicação da Pontificia Universidade Católica de São Paulo - DERDIC/PUCSP Med Imagem - Hospital Beneficência Portuguesa de São Paulo. São Paulo / SP - Brazil
Mail address:
Alfredo Tabith Junior
Rua Dra. Neyde Apparecida Sollitto, 435
São Paulo / SP - Brazil - Zip Code: 04022-040
Fax: (+55 11) 5908-8009
E-mail: alfredo.tab@uol.com.br
Article received on January 14, 2008.
Approved on March 19, 2009.

