INTRODUCTIONThe amyloidosis is a deposit disease that may be classified into two types: systemic and localized (1). The localized amyloidosis in the head and neck is a rare and benign disease, and may involve the orbit, paranasal sinuses, nasopharynx, oral cavity, salivary glands and larynx (2, 3, 4). The larynx is the most common affection region. There are a few reports in the literature regarding localized nasopharyngeal amyloidosis (5, 6).
The clinical classification is generally of recurrent epistaxis, post-nasal gout, nasal obstruction and Eustachian tube disorder when the lesion is expanded to the cavity of concha (4, 5, 6, 7). Despite the localized nasopharyngeal amyloidosis has a slow growth, the disease control is difficult for the recurrence or persistence possibility, even with surgical treatment (1, 6, 7).
CASE REPORTMale, white, 46-year-old patient with complaint of continuous nasal obstruction for three years associated with cases of rhinorrhea, maxillary and frontal sinusopathy, auricular plenitude in the left ear and recurrent epistaxis. Upon otorhinolaryngological exam we identified lesion in the left nasal meatus, soft palate convexity and a light retraction of the left tympanic membrane.
The computed tomography study of the face sinuses confirmed an obliteration by material with density of soft parts and an expansive effect of the maxillary sinus and nasal meatus to the left, with erosion of the maxillary sinus medial wall, nasal infundibula and nasal septum, in addition to the maxillary sinus reactive thickening (Picture 1).

Picture 1. Computed tomography of the face coronal cut confirming an obliteration by material with density of soft parts and an expansive effect of the maxillary sinus and nasal meatus to the left (arrow), with erosion of the maxillary sinus medial wall, nasal infundibula, nasal septum, and maxillary sinus reactive thickening.
We performed biopsy of the lesion whose anatomopathological study revealed amyloidosis.
The full physical exam of the patient was normal and there was no evidence of hepatosplenomegaly upon palpation. Lab exams for evaluation of renal function, electrocardiogram and abdominal ultrasonography didn't either present any alterations.
The patient was submitted to endoscopic resection of the lesion of approximately 3.5 cm at its major diameter, that expanded from the left nasal meatus up to the maxillary sinus (Picture 2). We carried out removal of the lesion and around the centripetally affected areas, started incision in the lateral nasal wall and subperiosteal detachment, ethmoid roof mass detachment and its releasing to the region of the cavity of concha and it was removed through the oral cavity. (Picture 3). The lesion fragments inside the maxillary sinus were removed with the help of optic instrument of 4mm and 70 degrees and angle clamps. The lesion didn't present adherence inside the maxillary sinus, which enabled its resection without the need for an external access (Caldwell-Luc type).
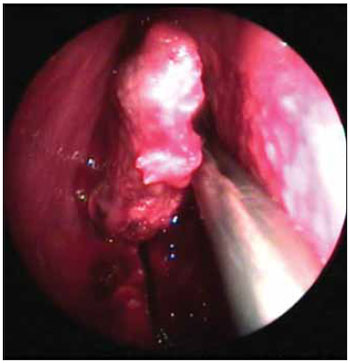
Picture 2. Image of the lesion in the left nasal meatus.
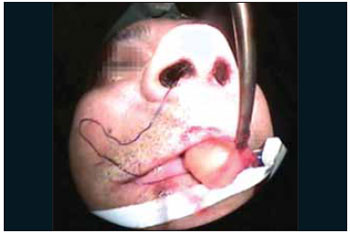
Picture 3. Image of the lesion being removed by the oral cavity.
The anatomopathological exam revealed squamous mucosa fragments and it had a stressed amyloid deposition in the middle of fibroblasts, which confirmed the previous amyloidosis diagnosis (Picture 4).
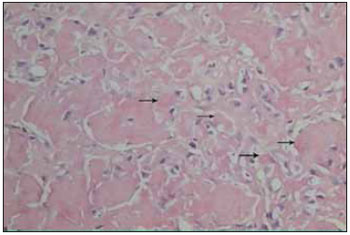
Picture 4. Squamous mucosa fragments with a stressed amyloid deposition at the core (arrows) in the middle of fibroblasts (HE 400x).
The patient presented with 3 years of follow up without recurrence of the lesion.
DISCUSSIONThe amyloidosis results from the deposit of insoluble, fibrous and amyloid proteins, specially in the extracellular spaces of organs and tissues that, when submitted to the Paunz test, presented a birefrigence when seen with polarized light (1, 3). They affect mainly individuals between the fourth and eighth decade of life, mainly the male sex (3:1 to 3:2). 1
The amyloidosis in the head and neck is a rare affection and is considered to be a benign process that generally manifests as localized amyloidosis. It affects mainly the larynx, subglottis and thyroid and may also affect the orbit, salivary glands, paranasal sinuses and oral cavity. The nasopharyngeal affection is extremely rare (1, 2).
When amyloidosis is diagnosed in the head and neck, we must exclude the systemic amyloidosis with involvement of the region of the head and neck as a part of the clinical manifestation. The possibility of the systemic disease must be excluded through a detailed anamnesis, full physical exam and laboratorial exams, such as serum electrophoresis, electrocardiogram and abdominal ultrasonography. Many authors suggest the performance of biopsy of gum, tongue, kidney, liver and rectal mucosa if the systemic disease is highly suspected. For many authors, the abdominal fat suction for Paunz test is an effective procedure, whose sensitivity (75% to 90%) is similar to the rectal mucosa biopsy. However, for other authors, it's not clinically efficient to make a research through biopsies for systemic amyloidosis in cases of localized amyloidosis without apparent systemic symptoms such as renal function alteration (6, 7).
The nasopharyngeal amyloidosis is a benign slow growth tumor, but its location may be aggressive and generally causes osteolysis (1). The symptoms are generally nasal obstruction, recurrent epistaxis and hypacusis secondary to effusive otitis media for disorder of the Eustachian tube (1, 2). Computed tomography or magnetic resonance help in the osseous destruction evaluation and the lesion extension viewing. The definitive diagnosis is histopathological (1, 2, 3).
The localized amyloidosis has an excellent prognosis, but the nasopharynx amyloid tumors are of difficult treatment and has a certain recurrence (4). The surgical excision was accomplished mainly through transpalatal access and the main complication is bleeding due to loss of vascular integrity for the amyloid infiltration in the blood vessels. However, currently, the nasal endoscopic access has been the choice for it's less invasive, as well as the more recent use of microincision instrument.
There is no evidence that the nasal amyloidosis surgical treatment expands the survival of patients or that the localized amyloidosis may progress to the systemic form (5, 6). Therefore, all patients must be followed up for the observation of recurrence evidences or the appearing of the systemic form of the disease, the latter without a definitive treatment so far (1).
FINAL COMMENTSAlthough its a rare disease, the nasal amyloidosis must be considered in the differential diagnosis of nasal obstruction, epistaxis and secreting otitis media. Moreover, the otorhinolaryngologist must acknowledge, understand it, diagnose it and plan its suitable treatment.
BIBLIOGRAPHICAL REFERENCES1. Pang KP, Chee LW, Busmanis I. Amyloidoma of the nose in a pediatric patient: a case report. Am J Otolaryngol. 2001, 22(2):138-41.
2. Patel A, Pambuccian S, Maisel R. Nasopharyngeal Amyloidosis. Am J Otolaryngol. 2002, 23:308-11.
3. Chin SC, Fatterpeckar G, Kao CH, Chen CY, Som PM. Amyloidosis concurrently involving the sinonasal cavities and larynx. AJNR Am J Neuroradiol. 2004, 25(4):636-8.
4. Tsikoudas A, Martin-Hirsch DP, Woodhead CJ. Primary sinonasal amyloidosis. J Laryngol Otol. 2001, 115:55-56.
5. Lim JS, Lebowitz RA, Jacobs JB. Primary amyloidosis presenting as a nasopharyngeal mass. Am J Rhinol. 1999, 13(3):209-12.
6. Zundel RS, Pyle GM, Voytovich M. Head and neck manifestations of amyloidosis. Otolaryngol Head Neck Surg. 1999, 120(4):553-7.
7. Tsai YT, Huang CM, Chen YJ, Leu YS. Localized Nasopharyngeal Amyloidosis - A Case Report. Tzu Chi Med J. 2005, 17(5):353-5.
1. Resident Doctor of the Otorhinolaryngology and Cervico-Facial Surgery Service of the Santa Casa de Misericórdia de Curitiba.
2. Otorhinolaryngologist Medical Doctor. Preceptor Doctor of the Otorhinolaryngology and Cervico-Facial Surgery Service of the Santa Casa de Misericórdia de Curitiba.
3. Otorhinolaryngologist.
4. Otorhinolaryngologist at the Hospital Cajurú - PR.
Institution: Irmandade da Santa Casa de Misericórdia de Curitiba. Curitiba / PR - Brazil.
Mail address:
Rua Dr. Pedrosa, 264 - Apto. 302A - Centro
Curitiba / PR - Brasil - Zip code: 80420-120
Fax: (+55 42) 3232-2735
E-mail: scheilasass@yahoo.com.br
Article received on May 20 2008.
Approved on September 02 2008.

