INTRODUCTION The need for a more precise awareness of the flora in the chronic otitis media is a basic point in the specialist day-by-day, both for the large frequency of cases and for the fact the cure of suppuration is an indispensible condition for a posterior functional surgery.
The (COM) chronic otitis media is a disease that still prevails in our area and tends to be persistent an destructive being able to lead to the production of irreversible sequels. Its etiopathogenesis is multifactor and the recurrent respiratory infections play an important role for the maintenance of this picture. The infectious process is characterized as polymicrobial, generally evolving with the association of facultative bacteria, strict aerobic and anaerobic and the latter is present in 30 to 60% of the cases (1).
According to JAHN (2), after the introduction of antibiotics as from the forties, the complications resulting from chronic otitis media disappeared almost completely from the otologic clinic. However, the indiscriminate use of antibiotics in medicine has been contributing, in the last years, for the appearing of multi-resistant samples and for the return of complications in this disease.
The main bacterial studies are due to PALVA, KARJA and RAUNIO (3); LANG col (4); HARKER and KOONTZ (5); KARMA, JOKIPH and OJALA (6); MELON and GORET (7); ITZHAK BROOK and BETHESDA (8); FEDERSPIL and col (9).
In one hand, we have to consider the types of germs mostly detected in ear secretion cultures and in the other hand the role of germs and their metabolic products in the evolution of chronic otitis.
The change of the bacterial population in chronic infection with time is a fact confirmed in the literature (1,2).
The objective of this work is to carry out a comparative study between the bacterial findings in the secretion of simple chronic and cholesteatomatous otitis media.
METHOD In the period from January 2006 to September 2008, we did a bacterioscopic retrospective study of 83 patients (125 ears) with COM, and including 43 patients (52 ears) with cholesteatomatous chronic otitis media (CCOM) and 40 patients (73 ears) with simple chronic otitis media (SCOM), attended in the ORL service of the Universidade de Santo Amaro - SP (UNISA). Patient data, such as the duration of the disease, previous laboratorial exams were taken note of and the clinical and/or surgical specimen were only collected from those who were not using antimicrobial in the period of until 15 days before the consultation. The study was duly registered in SISNEP and with authorization no 077/2008 of the ethics committee of the Universidade de Santo Amaro (UNISA - SP).
Out of a total of 125 infected ears, 52 with CCOM and 73 with SCOM were submitted to the secretion bacteriological exam. The age ranged from 2 to 75 years with predominance of the age range from 16 to 20 years old. There were 42 male and 41 female patients, out of whom, 64 were adults and 19 were children. The duration of otorrhea ranged from a minimum of 2 months until a longer time of 10 years.
For collection of the ear material, we first carried out the cleaning of the external auditory meatus with sterile saline solution. Then the secretion is collected through a very practical and simplified aspirator, which enabled the prevention of the collected material contamination. This equipment consists of a sterile collector glass, in which a rubber cover with two holes is connected. A input hole to adapt an aspiration system that will be connected to one tip of the aspirator, used to aspire the middle ear, through the external auditory meatus, in order to obtain the aspiration content.
In the other hole (output) we adapted a device that will be connected to a rubber that will be directly linked to an aspiration motor whose control startup will be made through a pedal (Figure 1). The operator may work under otoscopic/microscopic view and the middle ear fluid will be collected in the sterile bottle and sent as soon as possible to the laboratory, no longer than 24 hours, for exam of the collected sample. This enables a relatively sterile sample preventing its contamination, through the direct contact with the external auditory meatus or with the auricular speculum contact. Our secretion sample was obtained directly from the tympanic box through tympanic perforation.
The patients were forwarded for study at random, in the natural and causal sequence with which they arrived to the service. All had otorrhea at the initial service.
The material collected is introduced in test tube containing tioglicolate broth, sent to the laboratory and placed in sterilizer at 36oC for 18 to 24 hours. The sowing was performed in plates of:
- Ágar MacConkey.
- Ágar Sangue Columbia.
- Ágar Sangue Azida.
- Ágar Sangue Chocolate.
The plates are placed again in sterilizers and the first two ones at 36oC for 18 to 24 hours and the two last ones in carbon gas sterilizer at 36oC for 18 to 24 hours.
According to the growth observed we carry out the sowing in specific means for identification of the microorganism.
For the plates of Agar MacConkey with observed growth (gram negative bacilli), a new sowing is applied in the following means:
- Ágar Citrato
- Rugai and Araújo Means
- Plate for automated identification in the Mini API system.
The microorganisms that grow in the Rugai and Araújo's means are submitted to the following proofs: Indol, sucrose, glucose, ureases, lysine, motility proof, LTD and Gas.
In the validity of non-fermenting bacteria we used the oxidases proof and reading in the Mini API system.
As for the agents that grew in the Agar Sangue means (gram positive coconuts), the research was carried out following the type of agent found:
- For Staphylococcus sp.: Coagulase proof and/or DNAase was performed. In the positive samples for this test, Staphylococcus aureus was confirmed, while in those with negative proof a second test was performed, the novobiocine proof, and the resistance colonies identified as Staphylococcus saprophyticus and the sensitive ones as Staphylococcus epidermidis.
- For Staphylococcus sp.: The hemolytic group was identified and new proofs are carried out.
For statistical analysis we applied the chi-square test (19) to study associations between SCOM and CCOM and the variable studied. The nullity hypothesis rejection level was fixed at 0.05 or 5%.
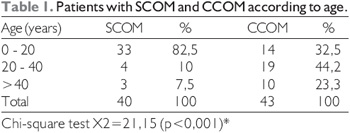
RESULTS Table 1 shows the distribution of the patients with (SCOM) simple chronic otitis media and (CCOM) cholesteatomatous chronic otitis media according to the age. The SCOM has a major association with the age from 0 to 20 years old.
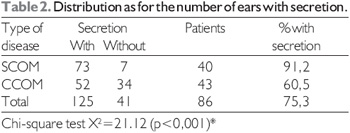
Table 2 shows the distribution as for the number of ears with secretion. The SCOM presented a major association with secretion.
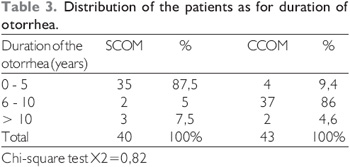
Table 3 shows the distribution of the patients as for the duration of the otorrhea. We did not find statistical significance between SCOM and CCOM during the period from 0 to 5 years and 6 years or more.
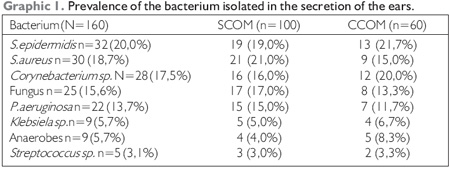
Graphic 1 shows the prevalence of the bacterium detected in the ears secretion. In the CCOM when compared to the SCOM, the S. aureus, fungus and P. aeruginosa were significantly less frequent, considering the most frequent anaerobes. The S. aureus was more frequent in the SCOM, while the anaerobes were more frequent in the CCOM. The P.aeruginosa was more frequent in the SCOM and the corynebaterium sp. presented a higher frequency in CCOM.
The S. epidermidis appeared with equal frequencies both in the SCOM and the CCOM.

Figure 1. Sterile collector glass, in which a rubber cover withtwo holes is connected.Copyright on behalf of Professor Dr. J. Evandro A. P. de Aquino.
The systematic exploitations are few concerning the microbiology of chronic otitis media in the literature researched in the last years. Studies by BARRETO & SERNADA (10) and SWARTZ & BARON (11) show the development of the bacteria and the enzymes secreted by them in the evolution of the chronic otitis. The incidence of the chronic otitis media is subject to large regional variations and its frequency is low in areas with a trained medical group, good hygiene, facility of the population for access to medical treatment. In regions where the conditions are less favorable, the chronic ears keep on increasing its incidence.
In the secretion from CCOM in our research, the S. epidermidis and Corynebacterium sp., that are native bacteria of the human skin, were found more frequently and the rate of appearing of S. aureus, P. aeruginosa and fungus were significantly lower than those of the SCOM. For IBEKWE and col (12) the S. aureus and the P. aeruginosa propose more several clinical problems in the management of COM and infectious diseases or in many other organs. These facts suggest that the bacterial infection must be not an essential cause of secretion, but one of the factors in the aggravation of the cholesteatoma, that is, an inflammatory change caused by keratin or cytokine, where it must be the strongest factor for cholesteatoma, while the secretion in the SCOM and many times resulting from bacterial infection. They concluded that this may prolong the aural secretion in the cholesteatoma more than in the SCOM, despite the use of antibiotics.
The incidence of P. aeruginosa in the secretion (13.7%) tends to decrease both in the cholesteatoma and in the SCOM. Such decrease may be reported with the use of new quinolones used currently as treatment. The incidence of Corynebacterium sp. in this study was of 17.5% of the cases and is accounted by mixed infection. In some cases the growth of Corynebacterium coming from the external auditory meatus humidified by the secretion with other causal organisms was possible.
IBEKWE & col (12) found it in the study of 102 ears with anaerobes, aerobes and fungi. Forty four percent were pure cultures, 33.3% mixed and 18.6% had no growth. Seventy-four percent were aerobic, 25% fungi and only 0.9% anaerobes; P. aeruginosa (22.5%) was the most isolated microorganism, followed by S. aureus and Aspergillus sp. In contrast, our outcomes are close to the works by Ibekwe and col. and these facts point out the need to promote an investigation of the action of the Corynebacterium sp. in the development of lesions of the COM.
Also comparing our outcomes, we found the work by SWEENEY and col (13) who isolated anaerobes in 52 out of 130 patients (44.0%) in whom they believe the use of tioglicolate in the first 73 patients inhibited the growth of anaerobes.
CONSTABLE & BUTLER (14) found anaerobes in 20 from 100 aspired patients, in whom the time of processing between the aspired until the laboratory was of one hour, but the medium used was enriched and the samples were incubated only 24 hours before the exposure to the laboratory air. Therefore, all these factors must lead to the reduction of the number of isolated anaerobes in these studies.
In contrast with ours, the studies by BROOK (15, 16) showed some diverging points. This author found anaerobic bacteria in 51.0% of the aspired of ears of children with COM. Such aspired agents were inoculated in an enriched medium were they report the growth of anaerobes in a period of 14 days, sufficient for growth.
The isolated aerobic bacteria were GRAM -, mainly S. aureus, P. aeruginosa and the isolated anaerobes were in mixed cultures with other anaerobes or with aerobic bacteria and the number of isolated anaerobes was between 2 and 4 per species showing a polymicrobial etiology of the COM. He also carried out a comparative study in the bacteria found in the middle and external ear. Only 50.0% of the bacteria found in the middle ear were also present in the external auditory meatus. Such findings show that the cultures collected from CAE before its sterilization may be masked. This is specially important as for the P. aeruginosa, which is the mostly found in the CAE than in the middle ear, although such organism inhabits the CAE, it may also be found in the middle ear, where it can take part of the inflammatory process.
The direct aspired elements of the middle ear through perforation of tympanic membrane are much safer in the establishment of the bacteriology of the COM and they may help in the selection of the own antimicrobial therapy.
The anaerobic bacterial rate in this infection is suggestive for its high rate of findings in the middle ear, compared to its finding in the CAE, 38 anaerobic species were found in the middle ear, by the same author, compared to only 7 found in the CAE. In our findings, the anaerobic germs were found with more frequency in the CCOM (8.3%).
We did not find any author in the literature who has distributed his patients as for the duration of the otorrhea. We may note that in the SCOM, the otorrhea had a higher duration frequency between 0 to 5 years old, while in the CCOM such frequency had a duration between 6 and 10 years or more.
This time of evolution since the first symptom varies too much per patient, and even not finding a non-negligent group of patients who exceeds 10.0% with an evolution with more than 30 years of disease, 30.0% of such patients wait between 6 and 10 years or more to seek the first medical service, and keep their symptoms for many years.
CONCLUSION We did not find notorious changes in the bacteriology of the suppurative chronic otitis media compared to the cholesteatomatous otitis.
In the suppurative chronic otitis media, the most frequent findings were the S. aureus, Pseudômonas sp. and fungi.
In the cholesteatomatous chronic otitis media, the most frequent findings were the anaerobes and Corynebacterium sp.
The frequency of appearing for S. epidermidis, Klebsiela sp. and Streptococcus sp. was equal in our study.
BIBLIOGRAPHICAL REFERENCES 1. Finegold SM & Wexler HM. Therapeutic implications of bacteriologic findings in mixed aerobic anaerobic infections. Antimicrob agents chemother. 1988, 32(5):611-16.
2. Jahn AF. Chronic otitis media: Diagnosis and treatment. Med. Clin. North. 1991, 75(6):1277-91.
3. Palva T, Karja J. Palva A. Raunio V. Bacterial in the chronic ear. Pre and postoperative evaluation. Pract. Oto-Rhino-Laryngol. 1969, 31:30-45.
4. Lang RW, Liu S, Lim DJ, Birk HG. Antimicrobial factors and bacterial correlation in chronic otitis media with effusion. Ann. Otol. Rhinol. Laryngol. 1976, 85(supp. 25):1945-51.
5. Harker LA, Koontz FP. The bacteriology of cholesteatoma. First Intern Conference on Cholesteatoma. Edited by Mac Cabe BF, Sade J, Abramson M. Aesculapius publishing Co.; 1977, p.264-67.
6. Karma P, Jokiph L, Ojala K, Jokiph AM. Bacteriology of the chronically discharging middle ear. Acta Oto- Laryngol (stockh). 1978, 86:110-14.
7. Meron J, Goret F. la microbiologie du cholesteatoma. Dounes bibliographiques Acta ORL (Belg). 1980, 34,(1):43-50.
8. Itzhak B & Bethesda J. Aerobic and anaerobic bacteriology of cholesteatoma. Laryngoscope. 1981, 91:250-56.
9. Federspil P, Feidt H, Koch A. Microbial spectrum in chronic otitis media and therapeutic conclusions. In: Proceedings of the 3rd Int. Conf. on cholesteatoma. Edited by: Tos M, Thomsen J, Peitersen E. Kugler & gedim Public; 1989, p. 595-8.
10. Barreto Sobrinho LPS & Sernada DF. Contribuição para estudo dos germes das otites media purulentas agudas e crônicas não colesteatomatosa. Sua sensibilidade aos antibióticos. Revista Paulista de Medicina. 1958, 52(maio):1-13.
11. Schwartz LE & Brown RB- Purulent otitis media in adults. Arch Intern. Med. 1992, 152(11):2301-4.
12. Ibekwe AO, Alshareef Z, Benavam A. Anaerocrobes and fungi in chronic suppurative otitis media. Ann. Otol. Rhinol., Laryngol. 1997, 106(8):649-52.
13. Sweeney G, Picozzi GL, Browning GG. A quantitative study of aerobic and anaerobic bacteria in chronic suppurative otites media J. Infect. 1982, 5:47-55.
14. Constable L, & Butler I. Microbial Flora in chronic otitis media. J. Inf. 1982, 5:57-60.
15. Brook I. Aerobic and anaerobic bacteriology of cholesteatoma. Laryngoscope. 1981, 91:250-3.
16.Brook I. Chronic otitis media in children: microbiological studies. Ann. J. Dis. Child. 1980, 134:541-64.
1. Doctoral Degree - UNIFESP. Head Professor.
2. Otorhinolaryngologist.
3. 2nd year Resident at Cema.
4. Head Professor at UNISA. Doctor Professor of Otorhinolaryngology.
5. Otology Professor of the Hospital Beneficência Portuguesa. Head Professor.
Institution: Universidade Santo Amaro (UNISA). São Paulo / SP - Brazil. Mail Address: José Evandro A. P. Aquino - Alameda Ribeirão Preto 410 - Apto 1106 - Bela Vista / SP - Brazil - Zip code: 01331-000 - Telephone: (+55 11) 8183-9729 - E-mail: clinicaorlsp@uol.com.br
Article received on August 14 2009. Accepted on August 31 2009.