INTRODUCTION The success of a cosmetic rhinoplasty is initially judged for its aesthetic outcome. However, the final outcome is only succeeded if the respiratory function is preserved (1).
Both lower thirds of the nose are formed by the cartilaginous pyramid - two upper lateral cartilages and the nasal septum cartilaginous portion (2). The lower third is formed by the nasal tip - lower lateral cartilages. The upper lateral cartilages are held on the lower surface of the nasal bones and expand caudally to form the cartilaginous portion of the nasal middle third, by holding laterally to the maxilla frontal process. In the middle line, the union of the upper lateral cartilages to the quadrangular cartilage of the septum forms the angle of 15º to 17º and corresponds to the middle nasal valve (subliminal) that contains the inner nasal valve. This area is the main region of resistance to the nasal airway flow (1,2).
The inner nasal valve is anatomically defined by the angle between the septum, medially, the caudal end of the upper lateral cartilage, laterally (ideally 10 -15o in Caucasians), and the lower infundibulum anterior end (3).
The middle nasal valve is an important area for its aesthetic and functional properties. This efficient and simple structure reveals its importance. Because it is a mobile and delicate tissue that allows the variable increases to the nasal resistance, so crucial for the nasal flow (1,4,5).
The correction of the wide nasal dorsum is a critical step in the rhinoplasty for it works in the nasal valve area with the challenge of a favorable aesthetic outcome without prejudice of its function.
This work describes an alternative technique for reduction of the wide nasal dorsum, aiming to reduce the nasal middle third width, with prevention of the inner nasal valve function.
METHOD This technique has been carried out for more than 3 years. According to our data, 25 patients aged between 22 and 55 years were operated with this technique.
Surgical Technique A precise preoperative clinical analysis is carried out. All parameters, measures, angles, symmetries and nose relations are analyzed. Any problem to be corrected is taken note of at this moment. The excess of upper lateral cartilage is determined through a subjective evaluation made by the surgeon, taking into account the patient's complaints.
The surgery may be carried out under general or local anesthesia with sedation, according to the surgeon and the patients' preference. The choice technique for the access may be close or open, also according to the surgeon.
Before the anesthetic induction or sedation nasal topical vasoconstrictor drops (oxymetazoline chlorohydrate) are instilled. Then the infiltration is performed in the dorsum, tip and nasal septum with a solution of lidocaine 2% with adrenalin 1:80000 for local anesthesia and vasoconstriction with the minimum necessary of anesthetic so as to avoid distortion of the nasal anatomy. The infiltration of the intercartilaginous incision region and hemitransfixing incision are also carried out, in the case of closed rhinoplasty, or in the marginal incision region and that of the columella for open rhinoplasty.
In the case of the closed access choice, the intercartilaginous and hemitransfixing incision is performed with communication between each other, or marginal and columella incision for displacement of the soft tissue according to a consecrated technique, in the case of outer access. Then the nasal dorsum skin is displaced from the osteocartilaginous structure, in a level above the upper lateral cartilages, through dissection with delicate Metzenbaum scissors with the nasofrontal angle as the upper limit.
The subsequent steps to be taken are the following: 1) separation of the septum upper lateral cartilages; 2) correction of the nasal gibe; 3) elliptic dissection and resection of the upper lateral cartilages; 4) work on the nasal tip; 5) lateral and bilateral paramedial osteotomy when applicable; 6) sutures.
Separation of the Septum Upper Lateral Cartilages The separation of the upper lateral cartilage of the nasal septum junction is carried out by means of incisions along the nasal septum up to the lower portion of the nasal bone bilaterally with number 15 scalpel lamina.
Nasal Gibe Correction The nasal gibe correction is made at this moment, if required, through the lowering of the septum quadrangular cartilage and medial portions of the CLS gradually. Then, the nasal dorsum osseous portion periosteum is unglued for removal of the osseous gibe with osteotome and further curettage.
Dissection and Resection of the Lateral Cartilages Ellipsis In the case of the choice of open or closed access, the ungluing of the nasal inner epithelium is made by leaving the CLS fully denuded.
Ellipsis confection: Before the confection of the ellipsis, the CLS' structure and excess analysis is made. The upper lateral cartilage excess is marked for the exact location of the region where an ellipsis will be dried in the diagonal and superior-inferior direction of the cartilage. The ellipsis width is determined according to the nasal structure and excess of the present cartilage. Then, a horizontal ellipsis is delimited with methylene blue almost parallel to the quadrangular cartilage, leaving 3 mm of cartilage around it for sustaining of the upper alar cartilage (Figures 1 and 2).
With the help of a hook the nasal wing is everted to expose the upper lateral cartilage and then with a number 11 scalpel lamina the ellipsis is dried horizontally following the cartilage lateral projection, at half distance of its width so as to prevent interference with the nasal valve. The evaluation of the size of the ellipsis to be dried must be made carefully to avoid stenosis of the nasal valve. It is important to recall that we left about 2 to 3 mm of cartilage in the ellipsis margin.
Refinement of the Nasal Tip The correction of the tip deformities is made in this step according to the pre-surgical plan.
Lateral and Paramedial Osteotomy The other rhinoplasty steps are carried out for a suitable contour of the dorsum. Lateral osteotomy operations are made and, if required, the paramedial osteotomy for a perfect correction of the nasal dorsum. A careful analysis of the nasal dorsum is made through the delicate palpation to assure there are no irregularities.
In the sequence adhesion plaster is applied and the fixing of a hard mould is proceeded. There is no need for nasal splint. The adhesive plaster and the mould are removed after seven days, when a new plaster is applied to be maintained for seven more days. The patient is guided in the postoperative as for the use of analgesic medication, if required, and a nasal physiologic solution for washing.
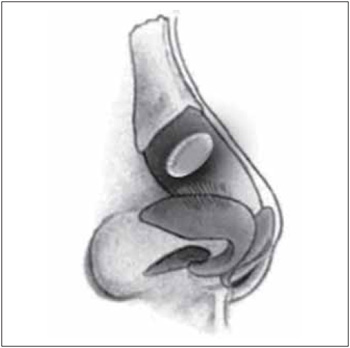
Figure 1. Lateral view of the ellipsis performed in the upper lateral cartilage.
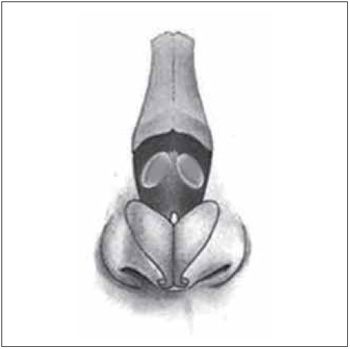
Figure 2. Front view of the ellipsis performed in the upper lateral cartilage.
In the patients evaluated below, the follow-up ranged from 6 to 24 months. The follow-up was carried out through inspection, physical exam and photographic documentation at every 3 months in the first year and in the sequence of each 6 months when possible.
There was no complication in the cases studied, specially as for the respiratory function. Only 2 patients reported a slight nasal pressure. The proposal for the next cases is to document through acoustic rhinomanometry the nasal area before and after the surgery.
At the end of the sixth month it was possible to note an almost natural aesthetic appearance, a phase in which the edema begins to resolve. All patients were satisfied with the dorsum final outcome.
Cases Report Case 1. Female patient aged 24 years with complaint of bent nose and desire to refinement of the nasal tip. Upon rhinoscopy, there were no endonasal abnormalities. Upon inspection there was laterorhinia to the right, a small osseous gibe and convexity of the nasal dorsum on the upper lateral cartilages and asymmetry of the nasal tip. The surgical steps carried out were described above. The open access was chosen. The postoperative evaluation with 6 months reveals a straight aesthetically well defined nasal dorsum harmonious with the facial lines (Figure 3).
Case 2. Female patient aged 40 years old with complaint of high nose and large dorsum. The surgical steps carried out were those described above through the closed access. The 24-month postoperative evaluation shows a aesthetically well defined nasal dorsum (Figure 4).
Case 3. Female patient aged 60 years old with complaint of nasal gibe and large dorsum. Upon external exam, the most notorious deformity was the large dorsum with a small gibe and tip asymmetry. The surgical steps carried out were those described above through the closed access. The postoperative evaluation with 12 months shows well-defined tip and nasal dorsum with improvement of the facial proportions (Figure 5).

Figure 3. Patient 1. Preoperative (above). 6 months of postoperative (below).
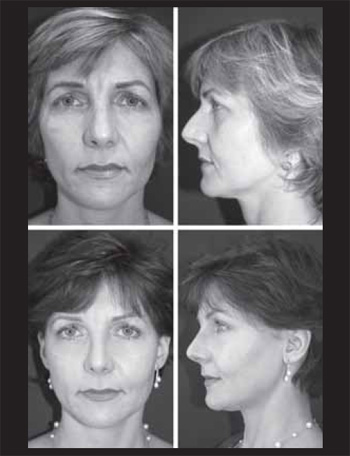
Figure 4. Patient 2. Preoperative (above). 24 months of postoperative (below).

Figure 5. Patient 3. Preoperative (above). 12 months of postoperative (below).
Alterations of the nasal dorsum is a critical step in rhinoplasty. 2.5 Subdividing a nasal surgery into purely functional and aesthetic categories is in the worst cases harmful to the patient. Therefore, each aesthetic change must be directly related to the nasal function (1).
According to the consecrated procedures, the nasal valve manipulation during rhinoplasty is essentially limited to the access to the dorsum for removal of the osseous gibe and narrowing of the nasal bones medially, correction of the inner nasal valve collapse or correction of the deviated nose with grafts (1,3,4).
The nasal valve is one of the most studied nasal structures and also the most sensitive to changes (1). The rhinoplasty steps must work carefully in this area and be meticulous in the resections.
The use of spreader type grafts or correction of valve insufficiency are techniques that work the valve region, but they may enlarge the middle third of the nose. Certainly each technique has its advantage when correctly indicated. In the case of patients with insufficiency of the inner nasal valve the use of grafts is functionally and aesthetically indicated.
In the cases of patients completely opposed to this situation, the large dorsum correction in patient without collapse of the inner nasal valve may be done with the removal of the CLS' ellipsis without functional prejudice. These patients need a refinement of the nasal dorsum without interference with the nasal flow.
In the literature there is no description of this technique. Prendiville and col. described a similar technique to refine the wide nasal dorsum, but in the junction of the lateral nasal cartilage with the septum. They described the technique as reverse spreader graft, in which they remove a strip of upper lateral cartilage along its length after releasing it from the septum and nasal bone, with good outcomes.
CONCLUSION In the correction of the large nasal dorsum, the upper lateral cartilage ellipsis resection is a useful alternative when well indicated. Care must be taken of patients with commitment of the inner nasal valve because this maneuver is contraindicated for it may aggravate the valve dysfunction.
BIBLIOGRAPHICAL REFERENCES 1. Sachs ME. Mastering Revision Rhinoplasty. New York: Springer, 2006.
2. Maniglia AJ, Maniglia JJ, Manilia JV. Rinoplastia: EstéticaFuncional-Recosntrutora. Rio de Janeiro: Revinter, 2002.
3. Clark JM, Cook TA. The butterfly graft in functional secondary rhinoplasty. Laryngoscope. 2002, 112(11):1917-25.
4. Prendiville S, Zimbler MS, Kokoska MS, Thomas JR. Middle-vault narrowing in the wide nasal dorsum: the "Reverse Spreader" technique. Arch Facial Plast Surg. 2002, 4(1):52-5.
5. Arslan E, Aksoy A. Upper lateral cartilage-sparing component dorsal hump reduction in primary rhinoplasty. Laryngoscope. 2007, 117(6):990-6.
1. Head Professor of the Otorhinolaryngology Discipline at PUC-PR. Preceptor of Rhinology and Facial Plastic Surgery of the Otorhinolaryngology residence of Hospital Angelina Caron. Coordinator of the Otorhinolaryngology Service of the Brazilian Red Cross Hospital - Paraná.
2. Otorhinolaryngologist. Fellow in Facial Plastic of the Brazilian Red Cross Hospital - Paraná.
Institution: Departamento de Cirurgia Plástica e Reconstrutiva Facial Hospital Angelina Caron e Hospital da Cruz Vermelha Brasileira. Curitiba / PR - Brazil. Mail Address: Antonio Nassif Filho - Hospital Sugisawa - Avenida Iguaçu, 1236 - Sala 305 - Rebouças - Curitiba / PR - Brazil - Zip Code: 80250-120 - Telephone: (+55 41) 3259-6663 - E-mail: nassiffilho@uol.com.br
Article received on July 26 2009. Accepted on September 14 2009.

