INTRODUCTION The rhabdomyosarcoma was initially described by WEBER in 1854 (1). It is a malignant neoplasm original from voluntary muscles. In spite of being rare in adults, it is relatively common in children and corresponds to 60% of the tumors in soft parts in this age range. The anatomic location of the rhabdomyosarcoma is variable and about 30% occur in the head and neck (2.3). However, this tumor is seldom found in the middle ear and mastoid (4).
The middle ear and mastoid rhabdomyosarcoma may present a large variety of signs and symptoms, including facial paralysis, otorrhea, otalgia etc. (5).
In 1907, GIUSEPPE GRADENIGO reported a number of patients with a syndrome characterized by otorrhea / otalgia, retro-orbital pain and abducent nerve paralysis (VI cranial pair) caused by an inflammation in the petrous apex. Afterwards, this syndrome received a name: Gradenigo's Syndrome (6).
We report the case of a 5-year-old boy who had otalgia to the right, right hemiface pain, facial nerve and abducent nerve paralysis to the right with diagnosis of rhabdomyosarcoma in the middle ear and right mastoid.
CASE REPORT The 5-year-old, male, white patient was brought to the Otorhinolaryngology and Head and Neck Surgery Service of the Base Hospital FAMERP, with a history of irritation and fall of the general state, beginning two weeks ago, and after one week he started with vomits (about 3 episodes) and difficulty to lateralize the right eye. Before this scenario, his mother sought the basic health service and it prescribed Amoxicillin (dose of 80mg/day), and the hypothesis of acute otitis media was raised. However, one day after the beginning of the medication use, the patient evolved with facial paralysis to the right and was then forwarded to our service.
Upon admission the child was irritated, crying, complaining of otalgia to the right and pain in the right hemiface. His relatives denied the presence of vertiginous symptoms. Upon physical exam, the child was full-blooded, hydrated, eupneic and afebrile. Upon inspection of the facial mimicry he presented with IV degree peripheral facial paralysis in the right hemiface. (Pictures 1 and 2) associated to the abducent nerve paralysis to the right, observed through the non-lateralization of the right eye (Picture 3). Upon otoscopy, the left tympanic membrane was integral and translucent and the right one was integral, incurved and with hyperemia. The patient did not have any other alterations in the physical exam.
Faced with this picture, the hypothesis of acute otitis media involving the right ear with right peripheral facial paralysis and commitment of the ipsilateral petrous apex (Gradenigo's Syndrome) was raised, and the child was admitted with Ceftriaxona (100mg/Kg/day), Dexametasona (0.25mg/Kg/day) antithermics and analgesics. Computed Tomography of Cranium and Mastoid was also requested, which confirmed the suggestive image of abscess in the petrous apex to the right and material with density of soft parts occupying the mastoid cavity and middle ear to the right. (Pictures 4 and 5). Before the tomographic findings, Nuclear Magnetic Resonance of Cranium and Inner Ear was requested, which showed a lesion on a plate located in a topography of cerebellar-pontine angle to the right with extension to the inner auditory meatus, paraselar region and infratemporal cavity, and determined the destruction of the petrous portion of the temporal bone and ipsilateral carotid canal (Pictures 6 and 7).
There was an attempt for audiometric exams (Tonal Audiometry and Brainstem Evoked Response Audiometry-BERA), but the child did not collaborate for their performance.
With the hypothesis of acute otitis media with intracranial complications, on the second day of internment, the patient was submitted to mastoidectomy of closed cavity in the right ear and myringotomy in the right tympanic membrane with exeresis of the material with yellow gelatinous aspect of the middle ear and mastoid cavity. This material was forwarded for anatomopathological analysis. After the surgery there was no improvement of the signs and signals, even with the use of the aforesaid medications.
On the seventh day of interment, the anatomopathological report revealed it was an Embryonal rhabdomyosarcoma of the middle ear and mastoid, which was confirmed for immunohistochemical evaluation.
Faced with this diagnosis, the patient was sent for the Oncopediatrics Service and the chemotherapy treatment began. However, the patient did not present with good evolution and then died with febrile neutropenias.

Picture 1. Picture showing facial paralysis to the right.
Picture 2. Picture showing Bell's sign to the right.

Picture 3. Picture showing paralysis of the VI pair to the right.
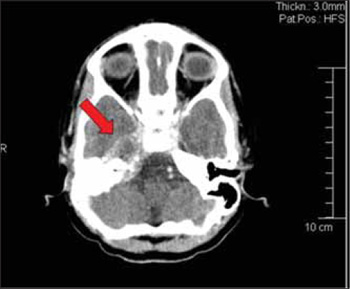
Picture 4. Computed Tomography in axial cut with arrow confirming the commitment of the right petrous apex and intracranial invasion.
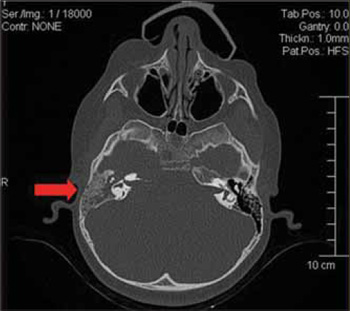
Picture 5. Computed Tomography of mastoid, in axial cut, with arrow appointing mastoid cells veiling to the right by a material with soft parts density.
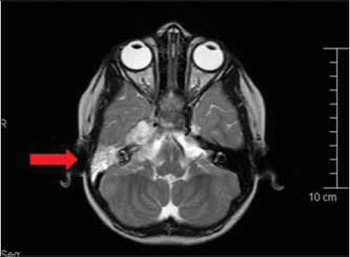
Picture 6. Magnetic Resonance with arrow indicating a lesion that occupies the middle ear, mastoid and petrous apex, and with intracranial extension.
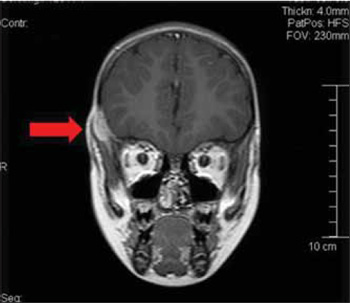
Picture 7. Magnetic Resonance with arrow showing a lesion in the temporal region to the right.
The rhabdomyosarcoma is an aggressive malignant tumor with origin from voluntary muscles and represents most of the soft parts tumors in children (5,7). The incidence of this tumor was estimated at 0.44 per 100.000 in Caucasians and 0.13 per 100000 in afro-descendents, individuals younger than 15 years old (8).
This tumor presents with a bimodal age range distribution with peaks of incidence between 2 and 5 years old and in adolescence, but more than 60% of the cases occur in children younger than 10 years old (9).
HORN and ENTERLINE carried out a classification system of rhabdomyosarcoma according to histological findings in four types: embryonal, botryoid, alveolar and pleomorphic (9). Out of these, the most common in the head and neck is the embryonal type (9) as in the case reported.
The rhabdomyosarcoma affects the region of the head and neck in approximately 30 to 40% of the cases, and may occur in regions such as the orbit, pterygopalatine cavity, parapharyngeal space, nasopharynx and more seldom in the middle ear and mastoid (3, 4, 10). When this tumor appears in the region of the middle ear and mastoid, it is considered to be aggressive due to its vicinity with noble structures, its tendency for intracranial invasion and large potential for meningeal involvement (11, 12).
The petrous apex is a pyramid-shape bone located in the most central portion of the temporal bone. The petrous apex region surrounds the internal auditory meatus and splits it into anterior and posterior portions. The anterior portion represents the cochlea, and this region is more affected by inflammations. The posterior portion represents the semicircular canals and the internal auditory meatus (13.14). In about 30% of the individuals, the petrous apex has aerated cells that facilitate the dissemination of infections from the middle ear and mastoid. Petrositis is a common complication of infections in the middle ear and mastoid, but with the development of antibiotic therapy, it became an uncommon complication currently.(15).
The Gradenigo's Syndrome with its triad of abducent nerve paralysis (VI cranial pair), deep retro-orbital or facial pain because of the commitment of the ophthalmic branch of the trigeminal nerve (V cranial pair) and otorrhea or otalgia, may not be present in its full shape in all cases of petrositis. In the description of this syndrome, carried out by GIUSEPPE GRADENIGO, in 1907, out of the 57 patients evaluated, less than a half presented with the classical triad.
In the case reported, the tumor was located in the region of the middle ear and mastoid and caused invasion of the petrous apex thus the patient presented with a picture of Gradenigo's Syndrome and peripheral facial paralysis. Initially, the patient was treated with the hypothesis of an acute otitis media complicated with the affection of the facial nerve (VII cranial pair) and the petrous apex (V and VI cranial pairs). After the anatomopathological result revealed it was Embryonal Rhabdomyosarcoma, the patient was sent to the Oncopediatrics Service for a suitable treatment.
CONCLUSION The rhabdomyosarcoma of middle ear and mastoid is a rare neoplasm, but it must be part of the differential diagnosis in cases where there are alterations in the middle ear and mastoid with a quick commitment of noble structures, such as facial nerve, trigeminal and abducent nerves, and may simulate a complicated acute otitis media and present with peripheral facial paralysis and/or Gradenigo's Syndrome.
BIBLIOGRAPHIC REFERENCES 1. Carli M, Guglielmi M, Sotti G, et al. Soft -tissue sarcomas. In Paediatric Oncology. 1997, 380-416.
2. Goto TK, Yoshiura K,Tanaka T, et al. A follow-up of rhabdomyosarcoma of the infratemporal fossa region in adults based on the Magnetic Resonance imaging findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86:616-25.
3. Viswanatha B. Embryonal rhabdomyosarcoma of the temporal bone. Ear Nose Thoroat J. 2007, 86:218-20.
4. Adrassy R. Rhabdomyosarcoma. J. Semin. Pediatr. Surg. 1997, 6:17-23.
5. Durve DV, Kanegaonkar RG, Albert D & Lavitt G. Paediatric rhabdomyosarcoma of the ear and temporal bone. Clin. Otolaryngol. 2004, 29:32-7.
6. Gradenigo G. Ueber Die Paralyse Des Nervus Abducens Bei Otitis. Arch Ohrenheilkunde. 1907, 74:149-87.
7. Mysorekar W, Harish K, Kilara N, Subramanian M, Giridhar AG.Embryonal rhabdomyosarcoma of the chest wall: a case report and review of the litrature.Indian J Pathol Microbiol. 2008, 51:274-6.
8. Young JL, Miller RW. Incidence of malignant tumors in US children. J. Pediatr. 1975, 86:254-58.
9. Rodeberg DA, Paidas CN, Lobe TL, et al. Surgical principles for children/adolescents with newly diagnosed rhabdomysarcoma: a report from the Soft Tissue Sarcoma Committee of the Childrens Oncology Group. Saroma. 2002, 6:111-122.
10. Hu J, Liu S, Qiu J. Embryonal rhabdomyosarcoma of the middle ear. Otolaryngol Head Neck Surg. 2002, 126:690-2.
11. Raney RB Jr, Tefft M, Newton WA, et al. Improved prognosis with intensive treatment of children with cranial soft tissue sarcomas arising in nonorbital parameningeal sites. A report from the Intergroup Rhabdomyosarcoma Study. Cancer. 1987, 59:1846-1902.
12. Sheity S, Abella A, Arcand P, et al.Temporal bone rhabdomyosarcoma in children. Int J Pediatr Otorhinolaryngol. 2007, 71:807-14.
13. Chole RA. Petrous apicitis: surgical anatomy. Ann Otol Rhinol Laryngol. 1985, 94:251-7.
14. Connor SE, Leung R, Natas S.Imaging of the petrous apex: a piectorial review. Br J Radiol. 2008, 81:427-35.
15. Zengel P, Wiekstrâ M, Janger L et al.Isolated apical petrositis: an atypical case of Gradenigos syndrome. 2007, 55:206-10.
1. Otorhinolaryngologist.
2. Otorhinolaryngologist. Responsible for the Otorhinolaryngology Service of the Otorhinolaryngology and Head and Neck Surgery Department of the Base Hospital / FAMERP - São José do Rio Preto - SP.
3. Otorhinolaryngologist. Responsible for the Cranio-Maxillo-Facial Surgery Service of the Otorhinolaryngology and Head and Neck Surgery Department of the Base Hospital / FAMERP - São José do Rio Preto - SP.
Institution: Hospital de Base / Faculdade de Medicina de São José do Rio Preto - SP (FAMERP). São José do Rio Preto / SP - Brazil. Mail Address: Renata Rennó Schiavetto Haber Rua Antônio Torres Penedo, 421, Sala 4 - Bairro: São Joaquim - Franca / SP - Brazil - Zip Code: 14406-352 - Telefone: (+55 17) 3212-9911 - E-mail: molinamd@terra.com.br
Article received on March 22, 2008. Article accepted on July 4, 2009.

